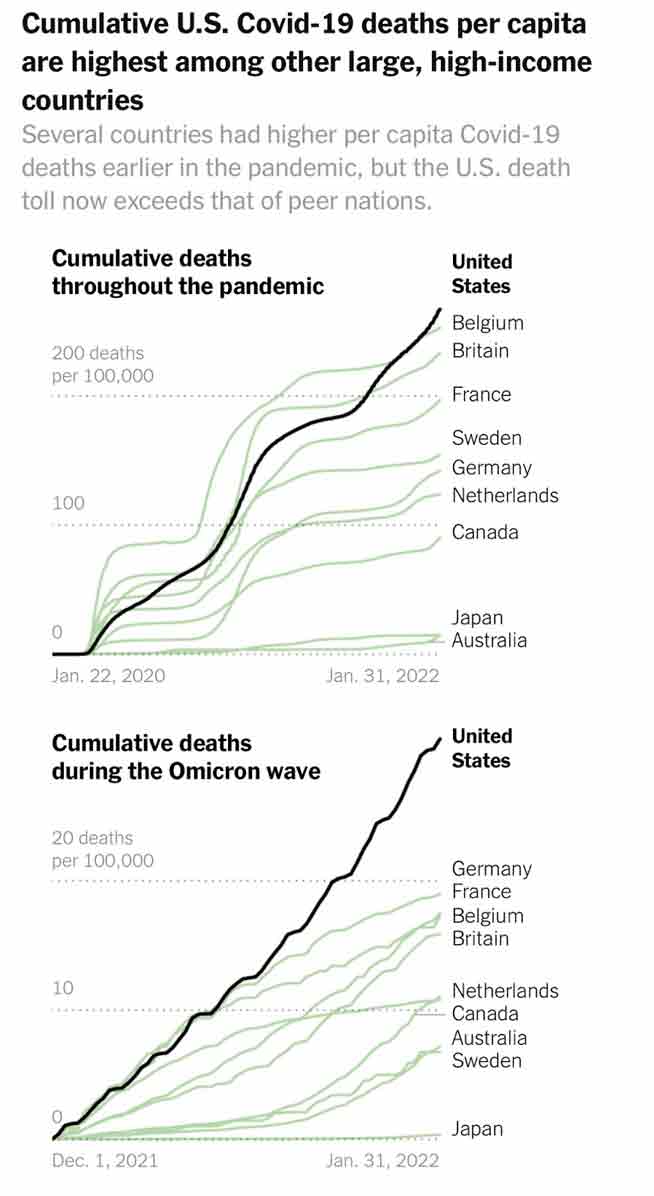
More than 1 million excess deaths have been recorded since the COVID-19 pandemic began nearly two years ago
These deaths are not all due to COVID-19, as higher numbers of deaths from heart disease, high blood pressure, dementia and other illnesses occurred during the pandemic
In separate research, a 22.9% increase in all-cause mortality was reported from March 1, 2020, to January 2, 2021, and an increase in death rates from non-COVID-19 diseases — including heart disease, diabetes and Alzheimer’s — was noted
As of January 27, 2022, U.S. excess mortality for 2021 was about 16%, compared to 13.6% in 2020; that is, excess mortality increased in 2021 — the year COVID-19 shots became prevalent
Former BlackRock portfolio manager Edward Dowd has documented a spike in mortality among younger, working-age individuals that coincided with vaccine mandates
More than 1 million excess deaths have been recorded since the COVID-19 pandemic began nearly two years ago, according to data released by the U.S. Centers for Disease Control and Prevention. These deaths are not all due to COVID-19, however, as higher numbers of deaths from heart disease, high blood pressure, dementia and other illnesses occurred during the pandemic.1
“We’ve never seen anything like it,” Robert Anderson, CDC’s head of mortality statistics, told The Washington Post.2 Health officials would have you believe that the majority of these excess deaths were due to COVID-19, but even the CDC states, on their webpage tracking provisional death counts for COVID-19:3
“Finally, the estimates of excess deaths reported here may not be due to COVID-19, either directly or indirectly. The pandemic may have changed mortality patterns for other causes of death. Upward trends in other causes of death (e.g., suicide, drug overdose, heart disease) may contribute to excess deaths in some jurisdictions. Future analyses of cause-specific excess mortality may provide additional information about these patterns.”
Excess Deaths ‘Only Partly Explained’ by COVID-19
In a study analyzing U.S. mortality data from March 2020 to July 2020, a 20% increase in excess deaths was found, but it was “only partly explained” by COVID-19. “Surges in excess deaths varied in timing and duration across states and were accompanied by increased mortality from non–COVID-19 causes,” researchers noted in a research letter published in JAMA.4
In an update to the analysis, using data for the remainder of 2020, a 22.9% increase in all-cause mortality was reported from March 1, 2020, to January 2, 2021, and an increase in death rates from non-COVID-19 diseases — including heart disease, diabetes and Alzheimer’s — was noted.5
In another example, excess mortality — that is, deaths in excess of the historical average — due to causes other than COVID-19 has also risen among males and minorities, particularly black males.
“Early evidence suggests a combination of factors, including deaths of despair, murders, uninfected Alzheimer’s patients, reduced health care use, and economic dislocation” were responsible for the significant increase in excess mortality among minorities, with researchers writing in PNAS, “Nearly half of the excess life years lost in 2020 are due to non–COVID-19 causes.”6
Excess Deaths Not Caused by COVID-19 Are Their Own Pandemic
University of Warwick researchers looked into the determinants of extra deaths that occurred during the pandemic, which were not due to COVID-19. Referring to these deaths as “collateral damage of the pandemic,” they found that “the scale of excess non-COVID deaths is large enough for it to be seen as its own pandemic.”7
Causes of the rise in non-COVID excess deaths include avoidance of health care facilities due to fear of COVID-19 and delayed diagnosis and treatment for other conditions. Non-COVID excess deaths were higher in areas with more stringent pandemic responses, like lockdowns, with researchers noting:8
“It lends some initial evidence to the theory that lockdowns increase excess deaths by providing a barrier to healthcare, worsening mental health and increasing domestic abuse and alcohol consumption.”
On Twitter, Silicon Valley software engineer Ben M. (@USMortality) revealed that, as of January 27, 2022, U.S. excess mortality for 2021 was about 16%, compared to 13.6% in 2020.9 That is, excess mortality increased in 2021 — the year COVID-19 shots became prevalent.
He tweeted, “2022 starting off with almost the same slope as 2021 … Excess mortality remains high even in 2022. Currently at around +23% for the latest week 2/2022.” In absolute numbers, he said, it comes down to nearly 15,000 more people dying per week than expected.
Previously, Ben M. revealed that in a 13-week period in late 2021, about 107,700 seniors died above the normal rate, despite a 98.7% vaccination rate.10 In another example, he used data from the CDC, census.gov and his own calculations to show excess deaths rising in Vermont even as the majority of adults have been injected.
“Vermont had 71% of their entire population vaccinated by June 1, 2021,” he tweeted in November. “That’s 83% of their adult population, yet they are seeing the most excess deaths now since the pandemic!”11
Deaths Increasing Despite Mass Injections
Excess deaths continuing into 2021, after widespread COVID-19 injections that were supposed to end the pandemic and save lives, is revealing. In one snapshot, in the week ending November 12, 2021, the U.K. reported 2,047 more deaths than occurred during the same period between 2015 and 2019. COVID-19 was listed on the death certificates for only 1,197 people.12
Further, since July 2021, non-COVID deaths in the U.K. have been higher than the weekly average in the five years prior to the pandemic.
Heart disease and strokes appear to be behind many of the excess deaths, with the Financial Times reporting, “The new phase of excess deaths raises the possibility that since the summer more people have been losing their lives as a result of strains on the NHS or lack of early diagnosis of serious illness …”13
An investigation by The Exposé, using official data from NHS and the U.K.’s Office for National Statistics (ONS), found that deaths among teenagers increased 47% since they started getting COVID-19 shots.14
Between the week ending June 26, 2020, and the week ending September 18, 2020, 148 deaths were reported among 15- to 19-year-olds. However, between the week ending June 25, 2021, and the week ending September 17, 2021, 217 deaths occurred among 15- to 19-year-olds. According to the investigation:15
“This shows that the number of deaths between June 19th 2021 and September 17th 2021 among teens aged 15 and over were 47% higher than the number of deaths in this age group during the same period in 2020, and the increase in deaths began at precisely the same time teens started receiving the Covid-19 vaccine.
Our investigation of ONS data also revealed further concerns about Covid-19 deaths in people between the age of 15 and 19. The same 2021 ONS dataset shows that since teens started getting the Covid-19 vaccine there has been at least one Covid-19 related death recorded in seven of the thirteen weeks between June 19th and September 17th 2021. A total of 8 deaths in this time frame.
Yet in the fifteen weeks prior to teens over the age of 15 receiving the Covid-19 vaccine, just a single death was recorded associated with Covid-19 among this age group.
Correlation does not equal causation, but it is extremely concerning to see that deaths have increased by 47% among teens over the age of 15, and Covid-19 deaths have also increased among this age group since they started receiving the Covid-19 vaccine, and it is perhaps one coincidence too far.”
More Younger Working-Age People Are Dying
Former BlackRock portfolio manager Edward Dowd has also pointed out “a spike in mortality among younger, working-age individuals [that] coincided with vaccine mandates. The spike in younger deaths peaked in Q3 2021 when COVID deaths were extremely low (but rising into the end of September).”16
Dowd also reported data from public funeral home company Carriage Services, which announced a 28% increase in September 2021 compared to September 2020, while August had a 13% increase. He tweeted:
“Business has been quite good since the introduction of the vaccines & the stock was up 106% in 2021. Curious no? Guys this is shocking as 89% of Funeral homes are private in US. We are seeing the tip of the iceberg.”17,18
Life insurance and disability claims, along with hospital death rates, are also revealing, and all have seen an uptick. Scott Davison, the CEO of Indiana-based insurance company OneAmerica, is among those who reported disturbing statistics — the death rate for 18- to 64-year-olds has risen 40% compared to before the pandemic.
“We are seeing, right now, the highest death rates we have seen in the history of this business – not just at OneAmerica,” Davison said, adding, “Just to give you an idea of how bad that is, a three-sigma or a one-in-200-year catastrophe would be 10% increase over pre-pandemic. So 40% is just unheard of.”19 Further, most of the deaths are not due to COVID-19. He said:20
“What the data is showing to us is that the deaths that are being reported as COVID deaths greatly understate the actual death losses among working-age people from the pandemic. It may not all be COVID on their death certificate, but deaths are up just huge, huge numbers.”
Mortality Rates and Death Claims Rising Post-Shots
Brian Tabor, president of the Indiana Hospital Association, confirmed that hospitals are also seeing widespread ill health and rising death rates. Zero Hedge reported:21
“Brian Tabor, the president of the Indiana Hospital Association, said that hospitals across the state are being flooded with patients “with many different conditions,” saying “unfortunately, the average Hoosiers’ health has declined during the pandemic.”
In a follow-up call, he said he did not have a breakdown showing why so many people in the state are being hospitalized – for what conditions or ailments. But he said the extraordinarily high death rate quoted by Davison matched what hospitals in the state are seeing. “What it confirmed for me is it bore out what we’re seeing on the front end …” he said.”
Other insurance companies citing higher mortality rates include Hartford Insurance Group, which announced mortality increased 32% from 2019 and 20% from 2020 prior to the shots. Lincoln National also stated death claims have increased 13.7% year over year and 54% in quarter 4 compared to 2019.22 Dowd tweeted:23
“Randy Frietag CFO just explained that in 2021 the share of young people dying from covid doubled in the back half of the year & that’s driven the result for Lincoln & its peers. He cited 40% in 3Q and 35% in 4Q were below the age of 65 … Mandates are killing folks … This shouldn’t be happening with miracle vaccines in a working age population period and a mild Omicron.”
US Seeks Additional $30 Billion to Fight COVID-19
Meanwhile, the White House is seeking another $30 billion to fight COVID-19, including $17.9 billion for vaccines and treatments, $4.9 billion for testing, $3 billion to cover coronavirus care for uninsured people, and $3.7 billion to prepare for future variants.24
The news comes amid a bombshell release by The New York Times, which revealed that the CDC has been collecting important data about COVID-19 all along, but hasn’t released most of it to the public. Information such as U.S. hospitalizations for COVID-19 according to age, race and injection status have been kept quiet, as has the effectiveness of COVID-19 booster shots among 18- to 49-year-olds.25
“Let’s be clear,” Steve Kirsch, executive director of the Vaccine Safety Research Foundation wrote. “The CDC hid the data because the data proves they were lying to us. That’s the real reason. If the data was favorable, I guarantee you, they would be releasing it.”26
Clarity on excess death data — specifically how many are truly attributable to COVID-19 and how many to other causes — is also essential for the public to make informed decisions about health care, shots and lifestyle during the pandemic, but such clarity is clearly lacking from the CDC.
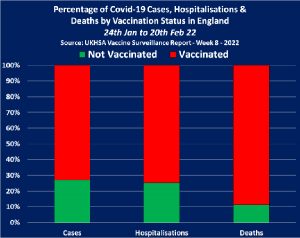
(Natural News) The UK Health Security Agency came out with their Week 8 report, which includes data on covid-19 cases, hospitalizations and deaths from January 24 to February 22. People who have been vaccinated with spike protein mRNA currently makeup 90 percent of covid-19 fatalities in England! A shocking 80 percent of these fatalities occur in people who have been vaccinated THREE times with spike protein mRNA. The data is taken from the UKHSA Vaccine Surveillance Report.
Covid-19 vaccines never stopped transmission and replication of coronaviruses and were NEVER 95 percent effective at preventing hospitalization and death, as was advertised. According to the data here, covid-19 vaccines are based on medical fraud and are a depopulation weapon that perpetuates disease and death.
Winter of 2022 becomes “winter of death” for the fully vaccinated
The official narrative is collapsing. The winter of 2022 was supposed to be a “winter of death” for the unvaccinated. However, the unvaccinated makeup only 27 percent of the caseload, 25 percent of hospitalizations, and roughly 10 percent of the deaths in England now. The United Kingdom is officially living in a pandemic of the “fully vaccinated.” To make matters worse, deaths continue to surge for populations that are triply vaccinated, proving that the third shot is not an immune booster in the slightest. This third shot is just another inflammatory dose of spike proteins – a game of Russian roulette that causes more blood clots and heart inflammation, leading to further immune system depletion, sickness and death.
While the Week 8 report paints a harrowing picture of vaccine failure, vaccine damage and propaganda exposed, the report also states, “this raw data should not be used to estimate vaccine effectiveness.” In other words, the raw data should be ignored and the covid-19 vaccination narrative should still be blindly and arrogantly believed.
According to the data, roughly 400,000 unvaccinated people tested positive for covid-19 and over one million VACCINATED people tested positive. A total of 752,126 of these cases were recorded in triply vaccinated individuals. This data is shocking because the unvaccinated are the ones who are typically coerced to take covid-19 PCR tests as a prerequisite to interact with the public. If the unvaccinated want to partake in certain public events and travel, they are more likely to be contact traced and forcibly swabbed as if they have no freedom or due process rights.
In contrast, most vaccinated individuals in the UK (who haven’t been disabled, sickened, hospitalized or killed by the vaccine) are able to show proof of vaccination and then go about their lives. However, no matter how many times the vaccinated are boosted and rebranded with vaccine passport updates, this is the group that is testing positive more often and showing up in the hospital.
Most of the positive covid-19 cases in the unvaccinated cohort (303,107) were recorded in children. This is because the children are routinely swabbed, isolated and shamed as subhuman disease spreaders. Additionally, children are classified as covid positive within 28 days of a hospital admission that had nothing to do with covid-19! According to the data, almost all of the children exhibit mild symptoms and recover. However, among the vaccinated hospitalizations, the survival rate is much lower.
The vaccinated are the ones taking up hospital beds and are the 90 percent majority who are dying
Vaccinated individuals have accounted for 73 percent of all covid-19 cases in England over the past month and are the obvious driving factor for viral transmission. The vaccinated are also the ones crowding the hospitals. There were 2,341 unvaccinated hospitalizations last month (a number that is falling rapidly). However, there were 6,889 hospitalizations for the vaccinated (a number that is rapidly increasing). Most of these hospitalizations are occurring in triply vaccinated individuals (4,936). In all, 75 percent of all Covid-19 hospitalizations are observed in the vaccinated.
When it comes to fatalities, the unvaccinated cohort is improving. The unvaccinated accounted for 559 deaths in the last reporting period and the vaccinated accounted for 4,302 deaths, with the majority of fatalities occurring in the triply vaccinated (3,120). The vaccinated population now accounts for 90 percent of the deaths overall. The triply vaccinated account for 4 of every 5 of these fatalities!
To put these figures in perspective, take a look at the Week 51 Vaccine Surveillance Report for 2021. From November 22 to December 19, 2021, there were 889 unvaccinated deaths and 2,913 vaccinated deaths. This shows that the fatality rate for the unvaccinated population is going down, while the fatality rate for the vaccinated population is getting severely worse. So, why hasn’t a strict moratorium been placed on this destructive vaccine?
Time and again, health experts and Pharma have denied that the mRNA shots go anywhere other than directly into the muscle into which they are injected. But now, a Swedish study has found that “ARS-CoV-2 RNA can be reverse-transcribed and integrated into the genome of human cells.”
What that means is they not only can enter your DNA but, according to the study, can do it within six hours of a person getting the shot.
A cost-benefit analysis shows the COVID jab increases children’s risk of dying from COVID infection. Children under 18 are also 51 times more likely to die from the jab than they are to die from COVID infection if not vaccinated
Four million doses must be administered to children, 5 to 11 years of age, to prevent a single ICU admission in this age group. Assuming two doses per child, that means 2 million children must risk potentially serious side effects to prevent a single child from requiring intensive care due to COVID-19
The Israeli Ministry of Health recently surveyed people who had received a third booster to determine the actual rate of side effects. Of the 2,068 interviewed individuals, 0.3% required hospitalization for an adverse event; three times more women than men (6.9% versus 2.1%) experienced neurological problems; 9.6% of women under the age of 54 experienced menstrual irregularities; 26.4% of those with preexisting anxiety disorder or depression experienced a worsening of their symptoms, as did 24.2% of those with preexisting autoimmune disorders
German health insurance data also show an alarming trend. After analyzing the medical data of 10.9 million insured individuals, one large health insurance company concluded that 400,000 doctors’ visits could be realistically attributed to jab side effects. Extrapolated to the total population of Germany, the total number of jab side effects requiring medical care would be 3 million, about 1,000% higher than admitted by the German Ministry of Health
Two autopsies of teenage boys who died within days of their COVID jabs revealed the shot caused their deaths
In mid-February 2022, the U.K. started rolling out the COVID jab for children aged 5 to 11. In the U.S., the shot has been recommended for this age group since October 2021.1
The question raised in a Nick De Bois interview with Jamie Jenkins,2 former head of health and labor market analysis at the British Office for National Statistics (above), is ‘Why bother injecting kids this young?’ The risk COVID-19 presents to children is minuscule.
What’s more, the British Joint Committee on Vaccination and Immunization (JCVI) estimates that by the end of January 2022, 85% of children aged 5 to 11 already had natural immunity.3 Add to that the fact that the prevailing variant, Omicron, is far milder than previous strains, causing only mild cold symptoms in most people, including children.
Together, these three facts ought to make it clear that children don’t need this jab. A cost-benefit analysis4 by Stephanie Seneff, Ph.D., and researcher Kathy Dopp, also shows the COVID jab actually increases children’s risk of dying from COVID infection. Children under 18 are also 51 times more likely to die from the jab than they are to die from COVID if not vaccinated.
Bill Gates Saddened by Widespread Natural Immunity
Bill Gates has even gone on record acknowledging that Omicron is creating widespread immunity. What’s so remarkable and revealing about his comment is the way he said it. He actually bemoaned the effectiveness of Omicron, as if it’s a horrible thing, saying:5
“SADLY, the virus itself, particularly the variant called Omicron, is a type of vaccine, in that it creates both T cell and B cell immunity, and it’s done a better job of getting out to the population than we have with vaccines.”
As noted by Jenkins, “What’s so sad about that?”6
Four Million Doses Required to Prevent a Single ICU Admission
An astounding statistic Jenkins does bring up is that 4 million doses must be administered to children, 5 to 11 years of age, to prevent a single ICU admission in this age group.7 Assuming two doses per child, that means 2 million children must take their chances with serious and potentially lifelong side effects to prevent a single child from requiring intensive care due to COVID-19. How is this justified? As explained in Jenkins’ website:8
“JCVI has said that vaccination of children aged 5 to 11 years who are not in a clinical risk group would prevent a relatively small number of hospitalizations or intensive care admissions. For a variant like Omicron, it would take around four million vaccine doses to two million children to prevent one admission to ICU.
For less severe illnesses, 58,000 child vaccinations would prevent one-child hospitalization. Children admitted recently to hospital with COVID had an average length of stay of 1-2 days. The Omicron wave saw no more children in hospital than before Omicron hit the UK.”
Pfizer Backs Off Shots for Children Under 5
While vaccine makers and health agencies have been pushing forward with COVID jabs for babies as young as 6 months, parents with children under 5 can, for now, draw a sigh of relief, as plans to roll out shots for the under-5 age group have been suspended, at least temporarily.
February 11, 2022, Pfizer withdrew its U.S. Emergency Use Authorization (EUA) application for children under 5.9,10 According to the U.S. Food and Drug Administration and Pfizer, they want to collect more data on the effects of a third dose, as two doses did not produce expected immunity in 2- to 5-year-olds.11
Three days later, former FDA Commissioner and current Pfizer board member Scott Gottlieb told CNBC12 the EUA application was pulled because COVID cases are so low among young children that the shot couldn’t be shown to provide much of a benefit.
Considering you have to give the jab to some 2 million children to prevent a single ICU stay, it’s no wonder they can’t show effectiveness in studies that have just a few thousand children. Pfizer’s youth trial on 5- to 11-year-olds had just 2,268 participants, and only two-thirds of those received the real COVID jab.13
However, the OpenVAERS team suspects there may be something far more problematic behind Pfizer’s withdrawal. In a February 21, 2022, email notice to subscribers, OpenVAERS stated:
“None of these explanations suffice because all of that information was known prior to Pfizer submitting this EUA to the FDA on February 1 [2022]. It makes one wonder whether adverse events in the treatment group might be the factor that neither Pfizer nor the FDA want to talk about?
So, we decided to look at reports of injury associated with COVID-19 vaccines in children 17 and younger. Remember, these shots have only been on the market for a short while and only children 5 to 17 are eligible. We created a separate page called Child Reports that will update automatically as new reports come in.
We were shocked by what we found — 34,223 VAERS reports in the U.S. in this age range, including infants harmed through transmission from the mother via breast milk, lots of reports of kids receiving shots who were too young (either the parents lied about their age or the doctor/pharmacy made a mistake with screening or dosing), and heartbreaking reports of myocarditis and death.”
Shocking Data From Israel Show Extent of Side Effects
While health agencies and mainstream media still insist that side effects from the COVID jab are “rare,” real-world data show a different story. An English translation of the report can be downloaded from Galileo Is Back on Substack.14 As noted in the report:
“On December 20, 2020, a vaccination program was launched in Israel using Pfizer’s vaccine for COVID-19. By the end of March 2021, more than half of the population had been vaccinated with two vaccine doses.
The decrease in immunity over time and emergence of new variants led to a renewed increase in morbidity in Israel in the summer of 2021. By the end of July 2021, a third shot of the vaccine (booster shot) was authorized for everyone who had received two shots and at least five months had passed from the second shot.
From data collection by medical teams or self-reporting by the public of side-effects in temporal proximity (passive monitoring), it appears that there is underreporting; therefore, it is important to identify side-effects in temporal proximity to vaccination with the booster in an active manner via a dedicated survey.
General goals: To determine the frequency of side-effects which appeared within 21-30 days from vaccination with the third Pfizer shot (booster) against COVID-19 among citizens above 18 years of age.
Specific goals: Examine the prevalence of side-effects in temporal proximity to the third shot grouped according to age and gender. Examine the time of onset relative to administration of the vaccine and the duration thereof, and to compare it with the side-effects of previous vaccines.”
In all, 2,894 people were contacted and 2,068 agreed to be interviewed (response rate: 71.4%). Of those 2,068 boosted individuals:
0.3% required hospitalization for an adverse event
4.5% experienced one or more neurological problems (2.1% of men and 6.9% of women), such as tingling or itching sensation, Bell’s palsy, vision damage, memory deterioration, hearing damage, convulsions, loss of consciousness and more
9.6% of women under the age of 54 experienced menstrual irregularities. Of those, “39% suffered from similar side-effects after prior COVID-19 vaccinations; however most (67%) indicated that the side-effects waned prior to the third vaccination and returned after receiving it”
26.4% of those with preexisting anxiety disorder or depression experienced a worsening of their symptoms
24.2% of those with preexisting autoimmune disorders experienced exacerbation of disease
Between 6.3% and 9.3% of those with preexisting high blood pressure, lung disease, diabetes and heart disease also reported that their condition was exacerbated after the third booster. A small number of women, but no men, also reported herpes infections (0.4% for herpes simplex infections and 0.3% for herpes zoster). Other key take-home’s from this Israeli report are that:
Side-effects are more common among women and younger people
1 in 10 women suffer menstrual irregularities
Neurological side effects typically don’t appear until about a month after the jab
In the majority of cases, the occurrence of a given side effect was not more severe after the third shot compared to the two previous doses. Put another way, the severity of side effects tends to be the same, regardless of the number of doses, so these finding can perhaps be applied to doses 1 and 2 as well
German Health Insurance Data Show Alarming Side Effect Rates
German health insurance data are also triggering alarms. Andreas Schöfbeck, a board member of a large insurance company called BKK ProVita, shared the data with Die Welt.15
They analyzed the medical data of 10.9 million insured individuals, looking for potential COVID jab side effects. To their horror, they found 400,000 doctors’ visits could be realistically attributed to the jab. According to Schöfbeck, extrapolated to the total population of Germany, the total number of doctors’ visits attributable to jab side effects would be 3 million.
“The number that resulted from our analysis are very far away from the publicly announced numbers [by the Ministry of Health]. It would be unethical not to talk about it,” Schöfbeck told Die Welt, adding that the data are “an alarming signal.” As reported by Die Welt (translated from German):16
“From January to August 2021 … around 217,000 of just under 11 million BBK policyholders had to be treated for vaccination side effects — while the Paul Ehrlich Institute keeps only 244,576 side effect reports based on 61.4 million vaccinated …
Thus, the number of vaccine side effects would be more than 1,000 percent higher than the PEI reports … With his analysis, Schöfbeck turned to a wide range of institutions — from the German Medical Association and the StiKo to the Paul Ehrlich Institute itself.
He said the figures were a ‘strong alarm signal’ that ‘absolutely must be taken into account in the further use of vaccines.’ His figures could be validated by the same data analyses of other health insurance companies, he says …
Since ‘danger to human life cannot be ruled out,’ he set a deadline of 6 p.m. Tuesday [February 22, 2022] to respond to his letter. As this passed, they turned to the public.”
Autopsy Results in Teens Reveal Heart Damage
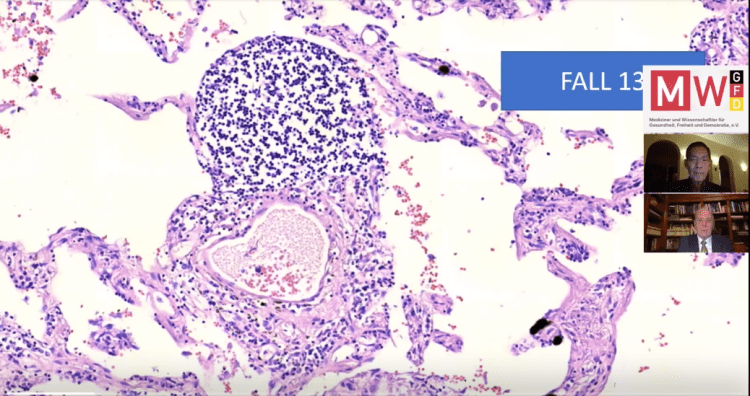
Getting back to the issue of children and the danger we’re putting them in by giving them this shot, two autopsies of teenage boys who died within days of their COVID jabs revealed the shot caused their deaths. As reported by The Defender:17
“The three pathologists, two of whom are medical examiners, published their findings Feb. 14 in an early online release article,18 ‘Autopsy Histopathologic Cardiac Findings in Two Adolescents Following the Second COVID-19 Vaccine Dose,’ in the Archives of Pathology and Laboratory Medicine.
The authors’ findings were conclusive. Two teenage boys were pronounced dead in their homes three and four days after receiving the second Pfizer-BioNTech COVID-19 dose. There was no evidence of active or previous COVID-19 infection. The teens had negative toxicology screens (i.e., no drugs or poisons were present in their bodies). These boys died from the vaccine.”
Histopathological examination revealed that neither of the boys’ hearts had signs of typical myocarditis. Instead, what they found were changes consistent with catecholamine-mediated stress cardiomyopathy, also known as toxic cardiomyopathy.
This is a temporary kind of heart injury that can develop in response to extreme physical, chemical or emotional stressors. Another common term for this kind of injury is “broken heart syndrome.” Hyperinflammatory states such as severe COVID-19 infection can also cause this kind of injury to the heart.
More details about the medical history of each of the boys and their autopsy findings are reviewed by Pam Popper of Wellness Forum Health in the video above. Curiously, neither of the boys had any symptoms of myocarditis before they died. One had complained of a headache and upset stomach. The other had not mentioned any symptoms. As noted by The Defender:19
“This is extremely concerning. These boys had smoldering, catastrophic heart injuries with no symptoms. How many others have insidious cardiac involvement from vaccination that won’t manifest until they get a serious case of COVID-19 or the flu? Or perhaps when they subject themselves to the physical stress of competitive sports?
These findings suggest a significant subset of COVID-19 deaths in the vaccinated could be due to the vaccines themselves. Furthermore, it raises this question: How often does this condition exist in a latent form in vaccinated individuals?”
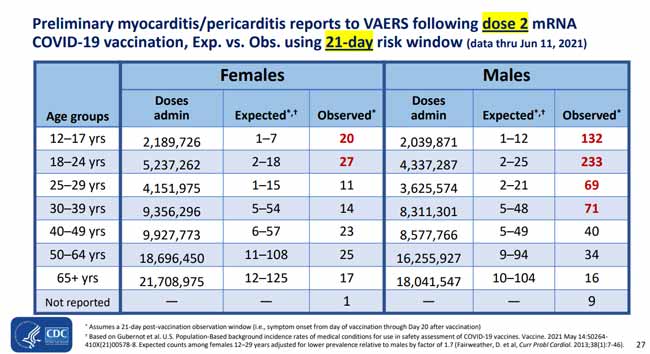
Myocarditis Risk in Young Men Is Not Rare
U.S. Vaccine Adverse Events Reporting System (VAERS) data also raise questions about the risk of potentially lethal myocarditis, especially in boys. The following slide was presented during a June 23, 2021, meeting convened by the Centers for Disease Control and Prevention’s Advisory Committee on Immunization Practices (ACIP), to discuss the risk of myopericarditis.20
As you can see, the observed rates of myocarditis and/or pericarditis for several age groups, and especially among males, are significantly higher than the expected background rate.
This is a loud and clear safety signal, yet the ACIP proceeded to recommend the shot to preteens and teens anyway, and in a public statement21 insisted that myopericarditis is “an extremely rare side effect” that “only an exceedingly small number of people will experience after vaccination.” How can they say that with data like this right in front of their noses?
Based on this VAERS data, the rate of myocarditis is about 6.5 per 100,000 doses in 12- to 17-year-olds. Going back to where we started, 4 million doses are required to prevent a single child, 5 to 11 years of age, from being admitted to the ICU for COVID.
Assuming the rate of myocarditis in 5- to 11-year-olds is identical to that of 12- to 17-year-olds, we could potentially be looking at 260 cases of myocarditis for every ICU admission for COVID that we prevent. On the whole, the COVID jab provides only risk for children under 18, so there’s absolutely no justification for it.
As Canadian Prime Minister Justin Trudeau pulled out all the stops to quash the trucker protest against vaccine mandates, it became clear that democracy has been an illusion
For many years, the technocratic elite, with their global authoritarianism goals, have infiltrated governments around the world and pushed for surveillance and national security tools intended to suppress dissent
A key part of that dissent-crushing system is the surveillance apparatus that has been erected. While sold as a tool to hunt down dangerous criminals, its primary purpose is to stifle dissent among peaceful, law-abiding citizens. Financial warfare — banning people from using financial services — is another
Dissent is also stifled by applying criminal terms to those who disagree with the narrative. Case in point: “Anti-vaxxers” and anyone who disagrees with pandemic measures are now labeled domestic terrorists or domestic extremists. Using terms of criminality allows those in power to justify the use of unconstitutional repression and punishment
The U.S. must repeal both the Patriot Act and the new biopreparedness initiative, or else all privacy and freedom will be destroyed
As Canadian Prime Minister Justin Trudeau pulled out all the stops to quash the trucker protest against vaccine mandates, without ever having actually listened to their complaints, a truth emerged, clear as day. Democracy has been an illusion. That’s the conclusion drawn by Canadian journalist Matthew Ehret in a February 18, 2022, Strategic Culture article.1
“Who would have thought that Canada would ever be a spark plug for a freedom movement against tyranny?” Ehret asks.
“Countless thousands of patriots have driven across the country to bunker down in Ottawa in peace and high festive spirits which I had to see with my own eyes to believe demanding something so simple and un-tainted by ideology: freedom to work, provide for families and a respect for basic rights as laid out in the Charter of Rights and Freedoms …
Mainstream media and political hacks have been working overtime to paint the Freedom convoy that converged on Ottawa on January 29 as an ‘insurrectionist movement’ full of ‘white supremacists,’ ‘Russian stooges,’ and ‘Nazis’ out to ‘overthrow the government.’
Even the Bank of England’s former governor (and World Economic Forum Trustee) Mark Carney chimed in on February 7 stating that ‘this is sedition’ and that ‘those who are still helping to extend this occupation must be identified and punished to the full force of the law’ …
Faced with an organic civil rights movement of blue-collar truckers, farmers and tens of thousands of supporters who have convened on Canada’s capital to demand a restoration of their basic freedoms, the current Liberal government has failed to show even an ounce of humanity or capacity to negotiate.
This shouldn’t be a surprise for those who have seen the hypocrisy of neo-liberal ‘rules-based’ order ideologues in action over the past few years who are quick to celebrate the ‘liberty’ of citizens of Ukraine, Hong Kong, or Xinjiang when the outcome benefits the geopolitical aims of detached technocrats hungry for global hegemony.
The moment genuine self-organized labor movements arise demanding basic rights be recognized, then the masks come off and the rage of tyrants show their true faces.”
Tyrants Are Showing Their True Colors
As reported by Ehret, the Deep State of Canada is now using the Emergency Measures Act to do precisely what Carney called for, namely identify and punish anyone who dares stand up for freedom.
The Act grants extraordinary powers to the banking industry to search people’s social media accounts and private bank records, and to seize the bank accounts of anyone suspected of supporting the Freedom Convoy, either in spirit or through online donations, including cryptocurrencies.
Victims will have no recourse, as the banks have been given full legal protection from lawsuits by those whose lives they destroy. Business owners in Canada who support freedom can also have their insurance policies canceled, and truckers can lose their drivers’ licenses, either temporarily or permanently.
Still, the protesters did not give up. If anything, the threats appeared to have had the opposite effect. According to Ehret, the protestors were “renewing their commitments to remain in place,” which they did until Trudeau sent in police2 to arrest protestors and tow their trucks.
While Trudeau remained dictatorial until the truckers had been cleared from the Parliament area, the political establishment, on the other hand, showed signs of cracking. Two Liberal Party members, MP Joel Lightbound and MP Yves Robillard broke with party ranks, calling for an end to the unpopular and unnecessary COVID measures.3 Then, finally, in a surprise turnabout, Trudeau buckled February 23, 2022, and said he would revoke the Emergencies Act he’d invoked earlier.4
On a global scale, the silence of leaders of democracies and republics around the world is as informative as Trudeau’s power grab. By now, we would have expected leaders of the U.S., the U.K., France and any number of others, to have stepped up to the microphone to denounce the Canadian government’s actions.
But they haven’t, and that tells you everything you need to know about where they stand on the issues of democracy and freedom. Worse, some have vocalized support for Trudeau’s dictatorial actions.
In a February 10, 2022, tweet, Juliette Kayyem, former assistant secretary of Homeland Security under U.S. President Obama and a frequent CNN commentator, suggested the Canadian regime ought to slash the truckers’ tires, empty their gas tanks, arrest the drivers, move the trucks, cancel their insurance, suspend their drivers’ licenses and prohibit their recertification in the future. In her own words, “I will not run out of ways to make this hurt.”5
The Illusion of Liberal Democracy Has Collapsed
As noted by Ehret, while we don’t yet know how it will end, one thing we can be sure of is that “the illusion of liberal democracy … has collapsed.”6 That doesn’t mean the globalist cabal will pack up their briefcases and retire. No, they’re going to fight to stay in power until the bitter end.
But the hill they’re standing on is getting steeper and slipperier by the day. Everyone can see that they’re saying one thing and doing the complete opposite. You can’t lay claim to being a defender of democracy, freedom and equal rights for all while simultaneously declaring peaceful citizens the enemy of the state. It’s just not credible. As noted by historically left-leaning journalist Glenn Greenwald:7
“When it comes to distant and adversarial countries, we are taught to recognize tyranny through the use of telltale tactics of repression. Dissent from orthodoxies is censored.
Protests against the state are outlawed. Dissenters are harshly punished with no due process. Long prison terms are doled out for political transgressions rather than crimes of violence. Journalists are treated as criminals and spies. Opposition to the policies of political leaders are recast as crimes against the state.
When a government that is adverse to the West engages in such conduct, it is not just easy but obligatory to malign it as despotic. Thus can one find, on a virtually daily basis, articles in the Western press citing the government’s use of those tactics in Russia, China, Iran, Venezuela and whatever other countries the West has an interest in disparaging …
That the use of these repressive tactics render these countries and their populations subject to autocratic regimes is considered undebatable. But when these weapons are wielded by Western governments, the precise opposite framework is imposed: describing them as despotic is no longer obligatory but virtually prohibited.
That tyranny exists only in Western adversaries but never in the West itself is treated as a permanent axiom of international affairs, as if Western democracies are divinely shielded from the temptations of genuine repression.
Indeed, to suggest that a Western democracy has descended to the same level of authoritarian repression as the West’s official enemies is to assert a proposition deemed intrinsically absurd or even vaguely treasonous.
The implicit guarantor of this comforting framework is democracy. Western countries, according to this mythology, can never be as repressive as their enemies because Western governments are at least elected democratically. This assurance, superficially appealing though it may be, completely collapses with the slightest critical scrutiny.”
The Dangers of Majority Despotism
As explained by Greenwald, the premise of the U.S. Constitution and the Bill of Rights is that “majoritarian despotism is dangerous in the extreme.” “Despotism” means government in which a single entity rules with absolute power. Usually, this entity is an individual, but despotism can also arise out of majority rule.
It’s interesting to note that while the Founding Fathers probably had no term for what we now know as the psychology of “mass formation,” they were clearly aware of the dangers posed by an irrational majority.
As noted by Greenwald, “the Bill of Rights consists of little more than limitations imposed on the tyrannical measures majorities might seek to democratically enact.”
For example, even if a majority of people agree that certain ideas and views should be criminalized, the Bill of Rights prohibits it. The Bill of Rights also prohibits the abolishment of religious freedom, even if a majority were to support it. Likewise, “life and liberty cannot be deprived without due process even if 9 out of 10 citizens favor doing so.”
The Founding Fathers were clever enough to realize that majority rule can easily become just as destructively despotic as any dictatorship. Hence, they ensured that individual freedoms were enshrined in such a way that even if you’re the last person in the country who wants to practice religion, you have the right to do so. The majority cannot take that away from you.
Waking Up to Reality as It Is
Greenwald goes on to explain how the signs of tyranny in the West have been evident for well over a decade. We just weren’t paying attention. Only now, as we stare tyranny in the face first-hand, are we starting to really see it for what it is:
“The decade-long repression of Julian Assange and WikiLeaks, standing alone, demonstrates how grave neoliberal attacks on dissent have become. Many are aware of key parts of this repression … but have forgotten or, due to media malfeasance, never knew several of the most extreme aspects.
While the Obama DOJ under Attorney General Eric Holder failed to find evidence of criminality after convening a years-long Grand Jury investigation, the then-Chairman of the Senate Homeland Security Committee, Sen. Joseph Lieberman (I-CT), succeeded in pressuring financial services companies such as MasterCard, Visa, PayPal and Bank of America to terminate WikiLeaks’ accounts and thus banish them from the financial system, choking off their ability to receive funds from supporters or pay their bills.
Lieberman and his neocon allies also pressured Amazon to remove WikiLeaks from its hosting services, causing the whistleblower group to be temporarily offline.
All of that succeeded in crippling WikiLeaks’ ability to operate despite being charged with no crime: indeed, as the DOJ admitted, it could not prove that the group committed any crimes, yet this extra-legal punishment was nonetheless meted out.
Those tactics pioneered against WikiLeaks — excluding dissenters from the financial system and coercing tech companies to deny them internet access without a whiff of due process — have now become standard weapons. Trudeau’s government seizes and freezes bank accounts with no judicial process.
The ‘charity’ fundraising site GoFundMe first blocked the millions of dollars raised for the truckers and announced it would redirect those funds to other charities, then refunded the donations when people pointed out, rightly, that their original plan amounted to a form of stealing. When an alternative fundraising site, GiveSendGo, raised millions more for the truckers, Canadian courts blocked its distribution.”
Greenwald also highlights how American politicians have pressured Big Tech monopolies and the financial system to act as a joint censorship arm of government. Blocking people and companies from being able to use servers and financial transaction services have been key strategies to silence critical voices.
Why Assange Was Targeted
According to Greenwald, Assange’s capture was precipitated by his denouncement of the Spanish government’s violence against citizens of Catalonia in 2017 and 2019. Catalonia wanted autonomy from the Madrid-based Spanish government, and the government responded with shocking force.
“Spain treated the activists not as domestic protesters exercising their civic rights but as terrorists, seditionists and insurrectionists,” Greenwald writes. “Violence was used to sweep up Catalans in mass arrests, and their leaders were charged with terrorism and sedition and given lengthy prison sentences.”
Assange did not actually express support for Catalonian independence. He objected to the Spanish government’s violent assault on civil liberties. This was why Ecuador rescinded Assange’s asylum and handed him over to British authorities in April 2020. Since then, Assange has been held in a high-security prison in Belmarsh, even though he’s never been convicted of a crime.
“All of this reflects, and stems from, a clear and growing Western intolerance for dissent,” Greenwald writes.8 “This last decade of history is crucial to understand the dissent-eliminating framework that has been constructed and implemented in the West. This framework has culminated, thus far, with the stunning multi-pronged attacks on Canadian truckers by the Trudeau government.
But it has been a long time in the making, and it is inevitable that it will find still-more extreme expressions. It is, after all, based in the central recognition that there is mass, widespread anger and even hatred toward the neoliberal ruling class throughout the West.”
Surveillance Apparatus Was Created to Crush Dissent
In response to the growing anger against the ruling class, the technocratic cabal has “opted for force, a system that crushes all forms of dissent as soon as they emerge in anything resembling an effective, meaningful or potent form,” Greenwald notes.
A key part of that dissent-crushing system is the surveillance apparatus that has been erected all around us.9 While sold as a tool to hunt down dangerous criminals, we’ve come to realize that rarely is the system ever used to go after true criminals. Instead, it’s used to identify people who disagree with a given narrative. Its primary purpose is to stifle dissent among citizens.
As noted by the ACLU,10 while most Americans think the Patriot Act’s surveillance powers are there to facilitate the identification and roundup of terrorists, it “actually turns regular citizens into suspects.” Dissent is also stifled by applying criminal terms to those who disagree with the narrative. Case in point: “Anti-vaxxers” and anyone who disagrees with pandemic measures are now labeled domestic terrorists or domestic extremists. As noted by Greenwald:
“Applying terms of criminality renders justifiable any subsequent acts of repression: we are trained to accept that core liberties are forfeited upon the commission of crimes. What is most notable, though, is that this alleged criminality is not adjudicated through judicial proceedings — with all the accompanying protections of judges, juries, rules of evidence and requirements of due process — but simply by decree …
Few things are more dangerous than a political leader who convinces themselves that they are so benevolent and well-intentioned that anything they do is inherently justified in light of their noble character and their enlightened ends …
Within the logical world where one is convinced that they really are fighting a white nationalist, fascistic, insurrectionary global movement to overthrow liberal democracy, then all the weapons we were long taught to view as despotic suddenly become ennobled …
And it is through this self-glorifying tale which Western neoliberals are telling themselves that they have become exactly what they shrilly insist they are battling.”
We Must Repeal the Patriot Act and Pandemic Powers
In September 2021, the White House announced a $65 billion biopreparedness initiative as part of the Biden administration’s Build Back Better plan.11 As I’ve explained in many previous articles, Build Back Better is part and parcel of The Great Reset, which in turn is a technocrat-led attempt to implement global authoritarianism. As reported by Biospace:12
“The first goal is to transform medical defense, including an improvement and expansion of vaccines, therapeutics, and diagnostics against known threats, and lay the groundwork for unknown pathogens … Secondly, the plan calls for ensuring ‘situational awareness’ regarding infectious disease threats. This includes early warning and real-time monitoring of these viral threats.”
In a nutshell, what this biopreparedness initiative entails is more invasive biosurveillance — meaning, the monitoring of your internal biology. Right now, claims that government wants to monitor people down to their body chemistry will earn you the title of paranoid conspiracy theorist, yet the writing is on the wall. That’s where we’re headed, even if we’re not there yet.
I believe the U.S. must repeal both the Patriot Act and the biopreparedness initiative, or else all privacy and freedom will be destroyed.
Data such as U.S. hospitalizations for COVID-19 according to age, race and injection status have been collected by the CDC for more than a year but most of it hasn’t been made public
The CDC published data on boosters’ effectiveness in adults under 65, but didn’t include data for 18- to 49-year-olds, “the group least likely to benefit from extra shots”
The CDC didn’t publish the data over concerns that it would be “misinterpreted,” but the only way the data could be interpreted as ineffective is if they show the shots don’t work
Dr. Robert Malone believes that the CDC withholding evidence about COVID-19 shot safety is scientific fraud
Malone is calling on Americans to demand the full COVID-19 data from the CDC and FDA, and for those in government who have lied to the American people to be held legally accountable
If you’ve felt like crucial data about COVID-19 have been missing since the start of the pandemic, it’s not in your head. An exposé by The New York Times has revealed that the U.S. Centers for Disease Control and Prevention has actually been collecting data all along — it just hasn’t published most of it.1
Data such as U.S. hospitalizations for COVID-19 according to age, race and injection status would have certainly been of interest to a large portion of the U.S. population. The CDC has been collecting such data for more than a year but hasn’t made the bulk of it public, the Times reported. What else has the CDC been keeping from the public?
For one thing, data on the effectiveness of COVID-19 boosters are missing. While the CDC published data on boosters’ effectiveness in adults under 65, this didn’t include data for 18- to 49-year-olds, a sizeable percentage of the population that also — coincidentally? — is “the group least likely to benefit from extra shots,” the Times pointed out.2
CDC Has Released ‘Only a Fraction’ of Its COVID Data
According to CDC spokeswoman Kristen Nordlund, the agency hasn’t released all of the data “because basically, at the end of the day, it’s not yet ready for prime time.”3 But, the Times reported, “Another reason is fear that the information might be misinterpreted, Ms. Nordlund said.”4
Among the additional data that the CDC kept quiet was wastewater data, which can give insight into COVID-19 case numbers in different areas. The CDC only recently released a wastewater data dashboard, even though certain states and cities have been providing such data to them since the pandemic began.5 Reportedly, several sources told the Times that the CDC “has published only a tiny fraction of the data it has collected.”
As the Times put it, the CDC’s refusal to post pertinent data left state and local health departments at a disadvantage:6
“Much of the withheld information could help state and local health officials better target their efforts to bring the virus under control. Detailed, timely data on hospitalizations by age and race would help health officials identify and help the populations at highest risk.
Information on hospitalizations and death by age and vaccination status would have helped inform whether healthy adults needed booster shots. And wastewater surveillance across the nation would spot outbreaks and emerging variants early.”
Data Withheld Over Fears of Creating ‘Vaccine Hesitancy’
The Times spoke with public health experts who said they had begged the CDC to release this type of COVID-19 data for two years and were “stunned” when they found out the agency had it all along.
The rational conclusion is that, had the data revealed what the CDC wanted, it would have released it. In their official reasoning, however, Nordlund said the data represents only 10% of the U.S. population, using that as an argument for why they didn’t release it. “But the CDC has relied on the same level of sampling to track influenza for years,” the Times pointed out. Further, it noted:7
“[T]he C.D.C. has been routinely collecting information since the Covid vaccines were first rolled out last year, according to a federal official familiar with the effort. The agency has been reluctant to make those figures public, the official said, because they might be misinterpreted as the vaccines being ineffective.”
Misinterpreted? “Let’s be clear,” Steve Kirsch, executive director of the Vaccine Safety Research Foundation wrote.8 “The only way the vaccine data could be interpreted as ineffective by us ‘misinformation spreaders’ is if the data shows the vaccines don’t work … The truth is the data didn’t support their narrative so they hid it. Do you think they would hide the data if it showed the vaccines worked? Of course not!”
In short, he wrote, the “CDC admits it withheld data from the public because they didn’t want to create vaccine hesitancy.”9 Transparency with data is key to building public trust and fostering open scientific debate, not to mention making sound public health guidelines. We now know the CDC has been hiding data, likely because its numbers don’t support the story they’ve been churning. The Gateway Pundit wrote:10
“So much for the bogus lie that has been pushed by public health officials for months, claiming that breakthrough infections weren’t being tracked at all. The medical elites just decided to hide the data because it didn’t fit the approved narrative, and, naturally, blamed the potential for ‘misinformation’ as justification for the coverup.”
In a tweet, Dr. Nicole Saphier, with the Memorial Sloan Kettering Cancer Center, shared her dismay in finding out that the CDC has been actively censoring which data to share with the public:11
“The CDC’s response when questioned about their withholding of Covid data and lack of transparency is essentially “we don’t trust you to be able to understand the truth.” The condescension is palpable. The wheels are finally coming off.”
Scotland to Stop Publishing COVID Data by Injection Status
It’s not only in the U.S. that health officials are cherry-picking data to support one agenda. Public Health Scotland (PHS) announced in February 2022 that it would stop publishing COVID-19 death and hospitalization data according to injection status. Like the CDC, their reasoning was concern that the data would be misrepresented by anti-vaxxers.12
The thing about data is, however, that it doesn’t lie — assuming it’s presented in full, unadulterated form. The only way such data could increase concerns about the safety and effectiveness of COVID-19 shots is if it showed that they’re ineffective and unsafe.
Now, instead of publishing full data for the public to analyze and have informed consent, the CDC plans to “do a lot more on the vaccine effectiveness side and try and make people understand how effective the vaccine is.”13 It’s this type of unified front across the globe that has many patriots, including former BlackRock portfolio manager Edward Dowd, calling foul. He said:14
“The responses from governments to this virus that doesn’t kill 99.9% of us makes no sense. And they’re all unified in their determination to put in these systems — these digital vaccination/passport systems. They’re all globally synced. They all want us to get these jabs, and it’s too unified. I suspect there’s a problem coming down the road.”
The CDC Withholding Data Is Scientific Fraud
Dr. Robert Malone, inventor of the mRNA and DNA vaccine core platform technology, believes that the CDC withholding evidence about COVID-19 shot safety is scientific fraud.15 He is calling on Americans to demand the full COVID-19 data from the CDC, and for the U.S. Food and Drug Administration and those in government who have lied to the American people to be held legally accountable:16
“If the CDC released the age stratified data for COVID, it would be clear that a vaccine for most Americans is not necessary. If the vaccine risk ratio of those vaccinated and hospitalized were published for Omicron — it would be clear that the vaccine benefit is not observed.
The FDA have not revealed what the efficacy of the boosters for children is. They have not released the safety data. They have withheld the safety data on the vaccines for children and adults.
This must stop. We are deep into outright Scientific Fraud territory. Let’s remember where this started … We have been manipulated from the VERY start of this pandemic. The government has been deciding what has been written, removed, censored by media and the big tech giants. This is propaganda.”
Even Dr. Yvonne Maldonado, chair of the American Academy of Pediatrics’s (AAP) Committee on Infectious Diseases, told The New York Times that they had been asking the CDC for data on children hospitalized with COVID-19, such as the proportion who have underlying medical conditions. On an information call with the CDC, they were told the data were unavailable.17
AAP also tried to find out from the CDC on multiple occasions how contagious people are five days after COVID-19 symptoms begin, to no avail, only to find out the information from a New York Times article they tracked down in December 2021. “They’ve known this for over a year and a half, right, and they haven’t told us,” she told the Times. “I mean, you can’t find out anything from them.”18
Should US Encourage Booster Shots for Children?
Malone is among those who have called COVID-19 injection mandates “completely unjustified” for children19 and recommends that youth who have received COVID-19 injections have their heart checked for damage,20 given the real risk of myocarditis and heart damage.
The U.S. is also an outlier globally in recommending that children ages 12 years and older should not only get COVID-19 shots but also a booster shot.21 While many countries are urging caution in COVID-19 shots and boosters for children, the CDC is moving full steam ahead, all while hiding data that could help U.S. parents make an informed decision for their children.
In the video above, author David Zweig explains that he interviewed a member of the CDC’s advisory committee and learned that a primary motivation for the agency recommending COVID-19 shots to kids isn’t to prevent severe illness, but to prevent mild or even asymptomatic infection. What’s more, an official told him that even this would likely only be beneficial for around two months, before the antibody boost begins to wane.22
Data presented at the meeting also showed that for young males, the shots increased the risk of injection-induced myocarditis enough so that it canceled out any benefit in avoiding hospitalizations from COVID-19. “So we have to really think through whether this is a worthwhile endeavor, and certainly one that should be mandated,” Zweig said.
Interestingly, the CDC officials spent one hour of the meeting discussing whether they should use the word “may” or “should” when it comes to recommending COVID-19 shots for children, and they settled on “should.” This term, Zweig said, is what can ultimately lead to mandates as the next step.23
Given the bombshell news that the CDC has been hiding COVID-19 data from the American people, parents and individuals must look beyond these official sources in their search for the truth. As Kirsch put it, “Let’s be clear. The CDC hid the data because the data proves they were lying to us. That’s the real reason. If the data was favorable, I guarantee you, they would be releasing it.”24
Recent data analysis shows the COVID jab is deadlier than COVID-19 itself for anyone under the age of 80. For younger adults and children, there’s no benefit, only risk
All age groups under 50 years old are at greater risk of dying after receiving a COVID jab than an unvaccinated person is at risk of dying from COVID-19
For those under 18, the COVID jab increases their risk of dying from COVID-19. They’re also 51 times more likely to die from the jab than they are to die from COVID if not vaccinated
Only when you get into the 60 and older categories do the risks between the jab and COVID infection become about even. In the 60 to 69 age group, the shot will kill one person for every person it saves from dying of COVID, so it’s a tossup as to whether it might be worth it for any given person
Data suggest U.S. deaths reported to VAERS are underreported by a factor of 20
According to a cost-benefit analysis by Stephanie Seneff, Ph.D., and independent researcher Kathy Dopp, the COVID jab is deadlier than COVID-19 itself for anyone under the age of 80. The cost-benefit analysis1 looked at publicly available official data from the U.S. and U.K. for all age groups, and compared all-cause mortality to the risk of dying from COVID-19.
“All age groups under 50 years old are at greater risk of fatality after receiving a COVID-19 inoculation than an unvaccinated person is at risk of a COVID-19 death,” Seneff and Dopp conclude. For younger adults and children, there’s no benefit, only risk.
“This analysis is conservative,” the authors note, “because it ignores the fact that inoculation-induced adverse events such as thrombosis, myocarditis, Bell’s palsy, and other vaccine-induced injuries can lead to shortened life span.
When one takes into consideration the fact that there is approximately a 90% decrease in risk of COVID-19 death if early treatment is provided to all symptomatic high-risk persons, one can only conclude that mandates of COVID-19 inoculations are ill-advised.
Considering the emergence of antibody-resistant variants like Delta and Omicron, for most age groups COVID-19 vaccine inoculations result in higher death rates than COVID-19 does for the unvaccinated.”
Real-Life Risk Reduction Is Negligible
The analysis is also conservative in the sense that it only considers COVID jab fatalities that occur within one month of injection. Looking at the U.S. Vaccine Adverse Events Reporting System (VAERS), we’re now seeing that many of those who are dying got the jab around April 2021 or earlier, so we know the shots can significantly cut your life short even if they don’t kill you in the first month. As detailed in Seneff’s and Dopp’s paper:
“Absolute real-life risk reductions (ARRs) … from COVID inoculations vary from a low of negative 0.00007% (an increased risk of a COVID death from inoculation) for children under age 18 to a positive 0.183% (0.00183) risk reduction of a COVID death for persons over age 80 …
COVID vaccine inoculations increase risk of death and produce a net negative benefit, aka increased risk of death … for all age groups younger than 60 years old. In other words, the COVID inoculations cause a net increase, rather than decrease, in the likelihood of death for all persons under 60 years old.
For those over 60 years old, the benefit of COVID inoculations is negligible, ranging from a 0.0016% reduction in likelihood of death for a 60- to 69-year-old persons to a 0.125% reduction in likelihood of death for those over 80 years old. Because preventative treatments are often given to well persons, a vaccine is supposed to provide very small risk compared to benefit.
Thus, such high fatality risks (VFRs) versus low benefit of risk reduction (ARRs) from the COVID inoculations are not acceptable, especially considering that low-cost, effective treatments are available that would additionally reduce COVID-19 death rates by as much as 90% or more if provided as soon as symptoms appear in high-risk persons.”
Meanwhile, data from an analysis2 by researchers Spiro Pantazatos and Herve Seligmann suggest U.S. deaths reported to VAERS are underreported by a factor of 20. Their analysis was used to calculate vaccine fatality rates (VFR), the number needed to treat/vaccinate (NNT) to prevent one COVID death, the expected number of vaccine fatalities to prevent one COVID death, and the expected number of vaccine fatalities compared to COVID fatalities by age group:3
Age group
VFR — Vaccine fatality rate
NNT to prevent one COVID death
Expected vaccine fatalities to prevent one COVID death
Expected number of vaccine fatalities compared to COVID fatalities
Under 18
0.004%
Vaccine causes higher COVID death rate
Vaccine causes higher COVID death rate
51
18 to 29
0.005%
318,497
16
8
30 to 39
0.009%
164,538
15
7
40 to 49
0.017%
55,516
9
5
50 to 59
0.016%
11,760
2
1
60 to 69
0.026%
3,624
1
1
70 to 79
0.048%
1,300
1
0
80 to 89
0.057%
547
0
0
Summary Findings
In summary, key findings in this paper include the following:
For those under 18, the COVID jab increases their risk of dying from COVID-19; those under 18 are 51 times more likely to die from the jab than they are to die from COVID if not vaccinated.
In those aged 18 to 29, the COVID jab is 16 times more likely to kill a person than save their life if they get COVID. They’re also eight times more likely to die from the jab than to die from COVID if not vaccinated.
Those aged 30 to 39 are 15 times more likely to die from the COVID jab than prevent their death, and they’re seven times more likely to die from the inoculation than to die from COVID if not vaccinated.
Those aged 40 to 49 are nine times more likely to die from the COVID jab than having it prevent their death, and they’re five times more likely to die from the jab than to die from COVID if not vaccinated.
Those aged 50 to 59 are twice (2 times) more likely to die from the COVID inoculation than to prevent one COVID death, while their risk of dying from the jab or dying from COVID if unvaccinated is about the same.
Only when you get into the 60 and older categories do the risks between the jab and COVID infection even out. In the 60 to 69 age group, the shot will kill one person for every person it saves from dying of COVID, so it’s a tossup as to whether it might be worth it for any given person.
Cost-Benefit Analysis Must Drive Public Health Policy
Common sense tells us that COVID-19 vaccination policy ought to be rooted in a rational evaluation of the true costs and benefits, and to do that, we need to assess whether the jabs are beneficial or harmful, and to what extent. So far, governments have completely ignored the cost of this mass injection campaign, focusing solely on perceived or imagined (not proven) benefit.
As a result, we’re looking at the worst public health disaster in known history. The greatest tragedy of all is that none of our public health officials has bothered to protect even the youngest among us.
The OpenVAERS team recently started looking at injury reports in children aged 17 and younger, and to their shock, they found 34,223 U.S. reports involving this age group through February 11, 2022. You can find the Child’s Report here.4 This is a staggering number, considering the 12- to 17-year-olds have only been eligible for the shot since May 2021, and 5- to 11-year-olds since October 2021.5
Pfizer Withdraws EUA Application for Children Under 5
Interestingly, February 11, 2022, Pfizer abruptly withdrew its Emergency Use Authorization (EUA) application for children under 5.6,7 The question is why? According to the U.S. Food and Drug Administration and Pfizer, they want to collect more data on the effects of a third dose, as two doses did not produce expected immunity in 2- to 5-year-olds.8
Three days later, former FDA Commissioner and current Pfizer board member Dr. Scott Gottlieb told CNBC9 the EUA application was pulled because COVID cases are so low among young children that the shot couldn’t be shown to provide much of a benefit.
But according in an email notice to subscribers, OpenVAERS stated, “None of these explanations suffice because all of that information was known prior to Pfizer submitting this EUA to the FDA on February 1 [2022]. It makes one wonder whether adverse events in the treatment group might be the factor that neither Pfizer nor the FDA want to talk about?”
Those Who Should Be in the Know Don’t Know a Thing
In related news, Jessica Rose, Ph.D., a research fellow at the Institute for Pure and Applied Knowledge in Israel, highlighted a February 5, 2022, Freedom of Information Request sent to the Therapeutic Goods Administration (TGA), the Australian equivalent of the FDA.10 The inquiry asked for documents relating to the TGA’s assessment of:
The presence and risk of micro-RNA sequences within the Comirnaty mRNA active ingredient (the mRNA genomic sequence)
The presence and risk of oncomirs (cancer-causing micro-RNA) in Comirnaty
The presence and risk of stop codon read-through (suppression of codon activity) arising as a result of the use of pseudouridine in Comirnaty
The composition of the final protein product (molecular weight and amino acid sequence) produced following injection of the Comirnaty mRNA product in human subjects
The risk of the use of AES-mtRNR1 3’ untranslated region of the Comirnaty mRNA product in human subjects
As it turns out, the TGA has none of these documents, because they’ve not assessed any of these risks. Why does this matter? Well, as explained by Rose:
“Micro-RNA (miRNAs) are small (20-22 nucleotides) single-stranded non-coding RNA molecules that function to interrupt or suppress gene expression at transcriptional or translational levels to regulate gene expression.”
Considering micro-RNA can alter gene expression, wouldn’t we want to know if micro-RNAs are present in the shot, considering we’re injecting hundreds of millions of people, including teenagers and children? The same goes for oncomirs, the suppression of codon activity, protein products and the rest.
“Stephanie Seneff has warned11 of two miRNAs that disrupt the type-1 interferon response in any cell, including immune cells: miR-148a and miR-590,” Rose continues.
“I don’t know what potential connections there are here yet, but it is safe to say that any tech that involves the introduction of foreign mRNA to be mass-produced by human cells must be thoroughly safety tested.
The fact that none of these documents ‘exist’ is proof positive that they either have no idea what the potential effects of what they made are because they did no bench work/investigations/studies, or, that they know and are hiding the results. Either choice is beyond criminal.”
The Critical Design Flaw
In an August 2021 Substack article,12 British cybersecurity researcher Ehden Biber homed in on the potential risks of using pseudouridine to optimize the codon.
The COVID shots do not contain the identical mRNA found in the SARS-CoV-2 virus. The mRNA has been genetically manipulated in a process called “codon optimization,” and this process is actually known to create unexpected and detrimental side effects.
“How come Pfizer, Moderna, AstraZeneca, Janssen etc. are using a technology that both they and the regulators know will cause unknown results?” Biber asked. The reason codon optimization was used is because it’s pretty difficult to get your body to produce a given protein by injecting mRNA.
It’s a slow and generally inefficient process. In order for the injection to work, they need higher levels of protein expression than is naturally possible. Scientists bypass this problem by making substitutions in the genetic instructions. They’ve discovered that you can swap out certain nucleotides (three nucleotides make up a codon) and still end up with the same protein in the end. But the increased efficiency comes at a terrible cost.
When substituting parts of the code in this way, the resulting protein can easily get misfolded, and this has been linked to a variety of chronic diseases,13 including Alzheimer’s, Parkinson’s disease and heart failure.14 As explained by Biber:15
“Turns out the protein which was manufactured when codon optimization has different ways it folds and a different 3D shape, and it ‘could cause immunogenicity, for example, which wouldn’t be seen until late-stage clinical trials or even after approval.’ This statement relates to the NORMAL approval cycle. The COVID vaccines went via an accelerated one.”
Now, the FDA has been fully aware of these problems since 2011, when Chava Kimchi Sarfaty, Ph.D., a principal investigator at the FDA, stated that “We do not believe that you can optimize codons and have the protein behave as it did in its native form.”
She went on to warn, “The changed form could cause immunogenicity, for example, which wouldn’t be seen until late-stage clinical trials or even after approval.”16
If the FDA knew all this back in 2011, why have they not raised objections against codon optimization being used in the making of the COVID jabs? The same question needs to be asked of the Australian TGA.
The FOIA requester was likely thinking of the March 2021 paper, “BNT162b2 Vaccine: Possible Codons Misreading, Errors in Protein Synthesis and Alternative Splicing Anomalies”17 when they put together that inquiry, because that paper highlights Pfizer’s extensive codon optimization using pseudouridine, which has known adverse effects, as well as the use of 3’-UTR sequence, the consequences of which are still unknown.
The fact that the TGA has no data on the risks of these modifications just goes to show that they, like the U.S. FDA, are not actually working to ensure these jabs are safe. They’re protecting the profits of the drug companies.
Pfizer even admits, in its BNT162b2/Comirnaty Risk Management Plan submitted to the FDA to get EUA, that the codon optimization they did resulted in elevated gamma-glutamyl transferase (GGT),18 which is an early marker of heart failure. Elevated GGT is also an indicator of insulin resistance, cardiometabolic disease,19 liver disease20 and chronic kidney disease.21
That alone should have raised some questions, were the FDA actually looking out for public health. All in all, there’s more reason than ever to question the COVID jab mandates and the use of these shots in children.
EVEN ATTACKS BY MEANS OF NEGATIVE REVIEWS CANNOT STOP THE TRUTH TO BE EXPOSED
================================================================================
ENGLISH
SGT Report
Feel Focused, Energetic and Rested Today, GET C60 EVO! https://www.c60evo.com/sgtr/
Save 20% on subscription, and use coupon code ( SGTR ) to get an extra 10% off
Author James Perloff returns to SGT Report in this 2016 rewind, this was the most watched interview on my YouTube channel, ever. Nearly 4 million views before the video along with my entire channel was nuked without cause or warning on October 15, 2020. So James asked me to repost it, and I thought that was a pretty good idea. Thanks for tuning in.
EVEN ATTACKS BY MEANS OF NEGATIVE REVIEWS CANNOT STOP THE TRUTH TO BE EXPOSED
================================================================================
ENGLISH
Kapelski
———————————————————-
Tägliche politische und Geoengineering-Nachrichten
Meine Kanäle: https://www.bitchute.com/channel/chembuster/ https://vimeo.com/chembuster
Ukraine is one of the most prominent countries in Europe for trafficking humans, with over 260,000 Ukrainian trafficking victims in the last 30 years. Soros and Hunter Biden are directly connected to these human trafficking rings, making millions off of other peoples misery.
For more than two years major media have been using their so-called “respected” fact-checkers to debunk any information on the COVID pandemic that doesn’t agree with the CDC’s and WHO’s drumbeat press releases.
U.S. Sen. Ron Johnson was just one person that The Washington Post’s fact checker, Salvador Rizzo, gave four Pinocchios to for “lying” about COVID vaccine information. Specifically, Johnson was called out for giving “false” information on the CDC’s Vaccine Adverse Event Reporting System (VAERS).
The only thing was, Johnson was the one telling the truth. It was Rizzo who was giving out false information, by trying to turn truth into lies and lies into truth. And, while people died, he and his Fourth Estate cohorts continued to spread lies as truths, including blaming the unvaccinated with natural immunity for the ongoing pandemic.
Johnson & Johnson has agreed to pay $26 billion to settle 3,000 state and local government claims that they helped contribute to the deathly opioid crisis.
In a second part of the settlement, the drug giant agreed never to sell opioid products again. “The companies said they are not admitting wrongdoing and are continuing to defend themselves against claims that they helped cause the opioid crisis that was brought by entities that are not involved in the settlements,” The Epoch Times said.
Top 5 signs you may have a vitamin D deficiency that you will notice as an individual include ongoing musculoskeletal pain, frequent or intense colds and flus, neurological symptoms such as depression, impaired cognition and headaches, unrelenting fatigue and head sweating
As a society, three key things that indicate a vitamin D deficiency are increasing or stable rates of the incidence of breast cancer, the increase in the number of preterm births and, now, an increase in the incidence of Type 1 diabetes
An estimated 40% of Americans are profoundly vitamin D deficient, defined as having a serum level below 20 ng/mL (50 nmol/L); 75% of American adults and teens are deficient when a sufficiency level of 30 ng/mL is used. If the sufficiency cutoff is moved to a healthy 40 to 60 ng/mL (100 to 150 nmol/L), as recommended by the GrassrootsHealth panel of 48 vitamin D researchers, deficiency rates in the U.S. would likely be in the high 90% bracket
20 ng/mL is grossly insufficient for good health and disease prevention. Rather, a vitamin D level between 60 and 80 ng/mL (150 to 200 nmol/L) appears to offer the greatest protection against cancer and other chronic diseases
Pregnant women need a minimum vitamin D level of 40 ng/mL (100 nmol/L) to help prevent premature birth and other pregnancy complications
Optimizing your vitamin D levels may help you prevent cancer, heart disease, autoimmune diseases, infections, neurodegenerative diseases and much more. Optimizing it is extremely simple and can be measured for success using an in-home test and some form of intake
This article was previously published January 1, 2019, and has been updated with new information.
Vitamin D deficiency is incredibly common around the world, but many mistakenly believe they aren’t at risk because they consume vitamin D-fortified foods, such as milk. However, few foods have therapeutic levels of vitamin D naturally, and even fortified foods do not contain enough vitamin D to support your health needs.
Despite its name, vitamin D is actually a steroid hormone that you obtain primarily through sun exposure, not via your diet. Since most dermatologists and other doctors recommend avoiding the sun and using sunscreen before venturing outdoors, vitamin D deficiency has reached truly epidemic proportions around the world.
Unfortunately, while the justification for sun avoidance is that it may reduce your risk of skin cancer, by avoiding sun exposure you risk vitamin D deficiency, which in turn raises your risk for many cancers — not only internal ones but also skin cancer, as well as a whole host of chronic diseases.
Considering the importance of vitamin D for disease prevention, strict sun avoidance is likely doing far more harm than good. The major problem with sun exposure is burning, not overall exposure. And, the easily treatable forms of skin cancer — squamous and basal cell carcinomas — are the ones most likely to form.
Definition of Vitamin D Deficiency
According to research1 published in June 2018, an estimated 40% of Americans are profoundly vitamin D deficient, defined as having a serum (blood) level of vitamin D below 20 ng/mL (50 nmol/L). Sufficiency is defined as having a level of 20 ng/mL or higher.
Calling someone with a vitamin D level of less than 20 ng/ml vitamin D deficient is like calling someone over 400 pounds simply overweight — in both cases a grossly serious understatement.
Seventy-five percent of American adults and teens are deficient in vitamin D when a sufficiency level of 30 ng/mL is used.2 If the sufficiency cutoff were to be moved to 40 to 60 ng/mL, sufficiency rates in the U.S. would likely be in the high 90% bracket.
It’s important to realize that 20 ng/mL has repeatedly been shown to be grossly insufficient for good health and disease prevention and, really, anything below 40 ng/mL (100 nmol/L) should be suspect. For example, research has shown that once you reach a minimum serum vitamin D level of 40 ng/mL, your risk for cancer diminishes by 67%, compared to having a level of 20 ng/mL or less.3
Most cancers occur in people with a vitamin D blood level between 10 and 40 ng/mL (25 to 100 nmol/L), and the optimal level for cancer protection now appears to be between 60 and 80 ng/mL (150 to 200 nmol/L).
Several studies also show that these higher vitamin D levels are protective against breast cancer specifically. Importantly, a 2005 study4 showed women with vitamin D levels above 60 ng/mL have an 83% lower risk of breast cancer than those below 20 ng/mL! I cannot think of any other strategy that can offer that kind of risk reduction.
More recently, a pooled analysis5 published in June 2018 of two randomized trials and a prospective cohort study came to a near-identical conclusion. The objective was to assess whether there are any benefits to having a vitamin D level above 40 ng/mL, as most studies do not venture into these higher levels.
Indeed, mirroring the 2005 findings, women with vitamin D levels at or above 60 ng/mL had an 82% lower incidence rate of breast cancer than those with levels of 20 ng/mL or less. Published research by GrassrootsHealth reveal as much as 80% of all breast cancer incidence could be prevented simply by optimizing vitamin D and nothing else.
Top 5 Signs of Vitamin D Deficiency
The only way to definitively identify vitamin D deficiency is via blood testing. However, there are some general signs and symptoms to be aware of as well. If any of the following apply to you, you should get your vitamin D levels tested sooner than later, and take proactive steps to boost your level into the 60 to 80 ng/mL range:
1.Ongoing musculoskeletal pain and achy bones — According to vitamin D researcher Dr. Michael Holick, whom I interviewed a few years ago, many who see their doctor for aches and pains, especially in combination with fatigue, end up being misdiagnosed as having fibromyalgia or chronic fatigue syndrome.
“Many of these symptoms are classic signs of vitamin D deficiency osteomalacia,6 which is different from the vitamin D deficiency that causes osteoporosis in adults,” Holick told me. “What’s happening is that the vitamin D deficiency causes a defect in putting calcium into the collagen matrix into your skeleton. As a result, you have throbbing, aching bone pain.”
2.Frequent illness/infections — Vitamin D regulates the expression of genes that influence your immune system to attack and destroy bacteria and viruses, so frequent illness and infections of all kinds, including colds and flu, is a tipoff that your immune function is subpar, which likely means you’re low on vitamin D.
3.Neurological symptoms — This includes depression, feeling blue, cognitive impairment, headaches and migraines. In 2006, scientists evaluated the effects of vitamin D on the mental health of 80 elderly patients and found those with the lowest levels of vitamin D were 11 times more prone to be depressed than those who received healthy doses.7
The same study also found low vitamin D was linked to poor cognitive performance. Several other studies8 have also linked vitamin D deficiency with poor mental function, confusion, forgetfulness and difficulty concentrating. Headaches and migraines are also associated with low vitamin D.9,10
4.Fatigue and daytime sleepiness — Studies have linked low vitamin D to persistent fatigue.11,12 In one case, a woman struggling with chronic fatigue, daytime sleepiness (hypersomnia), low back pain and daily headaches was found to have a vitamin D level below 6 ng/mL.
Her symptoms resolved once she raised it to 39 ng/mL.13 Another study14 found women with vitamin D levels below 29 ng/mL were more likely to complain of fatigue than those with levels above 30 ng/mL.
5.Head sweating — According to Holick, a classic sign of vitamin D deficiency is a sweaty head. In fact, physicians used to ask new mothers about head sweating in their newborns for this very reason. Excessive sweating in newborns due to neuromuscular irritability is still described as a common, early symptom of vitamin D deficiency.15
Top 5 Risk Factors for Vitamin D Deficiency
Several factors will influence your risk for vitamin D deficiency, including the following:
Rarely spending time outdoors and/or always wearing sunscreen — Researchers have noted that vitamin D deficiency is prevalent in adults of all ages who always wear sun protection (which blocks vitamin D production) or limit their outdoor activities.16 The ideal time for sun exposure is between 10 a.m. and 2 p.m., when the UVB rays are present.
Darker skin — Your skin pigment acts as a natural sunscreen, so the more pigment you have, the more time you’ll need to spend in the sun to make adequate amounts of vitamin D. If you have dark skin, you may need as much as 10 times more sun exposure to produce the same amount of vitamin D as a person with pale skin.
Being 50 or older — As you get older, your skin doesn’t make as much vitamin D in response to sun exposure. At the same time, your kidneys become less efficient at converting vitamin D into its active form. Older adults also tend to spend more time indoors (i.e., getting even less sun exposure and therefore vitamin D).
Obesity — Because vitamin D is fat-soluble, body fat acts as a “sink” by collecting it. If you’re overweight or obese, you’re therefore likely going to need more vitamin D than a slimmer person. In one recent study,17 vitamin D deficiency was three times more prevalent in obese individuals.
Gastrointestinal problems — Since vitamin D is fat-soluble, which means if you have a gastrointestinal condition that affects your ability to absorb fat, you may have lower absorption of fat-soluble vitamins like vitamin D as well. This includes gut conditions like Crohn’s, celiac and nonceliac gluten sensitivity and inflammatory bowel disease.
Health Benefits of Vitamin D Optimization
Optimizing your vitamin D levels has been shown to have a powerful effect on health, helping protect against a wide variety of diseases. Among them:
Dry eye syndromes18,19
Macular degeneration,20,21 which is the No. 1 cause of blindness in the elderly.
Autoimmune diseases — Vitamin D is a potent immune modulator, making it very important for the prevention of autoimmune diseases such as multiple sclerosis, inflammatory bowel disease and psoriasis, just to name a few.
Gastrointestinal diseases22 — Dysbiosis of your gut microbiome, inflammatory bowel disease and colitis are all disorders connected to vitamin D deficiency.
Infectious diseases, including influenza and HIV23,24
Inflammatory rheumatic diseases25 such as rheumatoid arthritis — A 2020 study showed that “vitamin D supplementation seemed to be an effective intervention for patients with rheumatoid arthritis. Different doses of vitamin D and durations of intervention produce different effects.”
Osteoporosis and hip fractures
Cardiovascular disease — Vitamin D is very important for reducing hypertension, atherosclerotic heart disease, heart attack and stroke, as it plays a vital role in protecting and repairing damage to your endothelium.26
It also helps trigger production of nitric oxide — which improves blood flow and prevents blood clot formation — and significantly reduces oxidative stress in your vascular system, all of which are important to help prevent the development and/or progression of cardiovascular disease.
According to Holick, vitamin D deficiency increases your risk of heart attack by 50%, and if you have a heart attack and you’re vitamin D deficient, your risk of dying from that heart attack is virtually guaranteed.
Indeed, a Norwegian study27 published in The Journal of Clinical Endocrinology and Metabolism found “a normal intake of vitamin D” significantly reduces your risk of death if you have cardiovascular disease.
Neurological diseases such as Alzheimer’s disease28,29 and epilepsy — In one study,30 epileptics given a one-time megadose of vitamin D3, ranging from 40,000 IUs all the way up to 200,000 IUs, followed by a daily dose of 2,000 to 2,600 IUs a day for three months to bring each individual’s vitamin D status to at least 30 ng/mL, resulted in significant improvements.
Ten out of 13 had a decrease in the number of seizures, five of whom experienced more than a 50% reduction. Overall, the group had a 40% reduction in the number of seizures.
Lupus — According to researchers in Cairo,31 most patients with systemic lupus erythematosus have some level of vitamin D deficiency, defined as a level of 10 ng/mL or less, or insufficiency, a level between 10 and 30 ng/mL.
Obstructive sleep apnea — In one study, 98% of patients with sleep apnea had vitamin D deficiency, and the more severe the sleep apnea, the more severe the deficiency.32
Bone health, falls and fractures — A 2006 review33 looking at vitamin D intakes and health outcomes such as bone mineral density, dental health, risk of falls, fractures and colorectal cancer, found “the most advantageous serum concentrations of 25(OH)D begin at 30 ng/mL, and the best are between 36 to 40 ng/mL.”
Obesity and diabetes — Research34 has shown vitamin D supplementation (4,000 IUs/day) combined with resistance training helps decrease your waist-to-hip ratio, a measurement that is far better at determining your risk for Type 2 diabetes and heart disease than body mass index.
Type 1 diabetes — Data from GrassrootsHealth’s D*Action project to prevent Type 1 diabetes35 suggests maintaining a vitamin D level between 40 and 60 ng/mL (100 to 150 nmol/L) may prevent Type 1 diabetes, and stop the progression of the disease, which is a growing problem.
Neurodegenerative diseases, including Alzheimer’s, Parkinson’s and multiple sclerosis (MS)36 — Research shows MS patients with higher levels of vitamin D tend to experience less disabling symptoms.37 Vitamin D deficiency is also common among patients with Parkinson’s38 and seniors with severe vitamin D deficiency may raise their risk for dementia by 125%.39
DNA repair and metabolic processes — One of Holick’s studies showed healthy volunteers taking 2,000 IUs of vitamin D per day for a few months upregulated 291 different genes that control up to 80 different metabolic processes, including DNA repair and autoxidation (oxidation that occurs in the presence of oxygen and/or UV radiation, which has implications for aging and cancer).
Preterm birth — A level of 40 ng/mL has also been shown to offer powerful protection against preterm birth if you’re pregnant.40 Women with a vitamin D level of at least 40 ng/mL may lower their risk of preterm birth by as much as 62%, compared to having a level of just 20 ng/mL. Women with a history of preterm birth gain even greater protection — an 80% reduction — when raising their vitamin D level above 40 ng/mL.
Pregnancy complications — Having a vitamin D level above 40 ng/mL also protects the mother by reducing her risk of preeclampsia, gestational diabetes and prenatal infections by approximately 50%.41
All-cause mortality — Studies have also linked higher vitamin D levels with lowered mortality from all causes.42,43,44
Vitamin D Levels Can Affect COVID Risk
Evidence showing vitamin D lowers your risk of SARS-CoV-2 infection, hospitalization, severe complications and death continues to mount, with study after study showing that your vitamin D status before you become infected can greatly affect not only your risk of getting COVID, but how well you recover (or don’t) from it.
Included in those studies is a scientific review45 in the journal Nutrients, which I co-wrote with William Grant, Ph.D., and Dr. Carol Wagner, both of whom are part of the GrassrootsHealth expert vitamin D panel. We found that at least 14 observational studies offer evidence that serum 25-hydroxyvitamin D concentrations are inversely correlated with the incidence or severity of COVID-19.
The evidence to date generally satisfies Hill’s criteria for causality in a biological system, namely, strength of association, consistency, temporality, biological gradient, plausibility (e.g., mechanisms), and coherence, although experimental verification is lacking. Thus, the evidence seems strong enough that people and physicians can use or recommend vitamin D supplements to prevent or treat COVID-19 in light of their safety and wide therapeutic window.
As of October 31, 2021, our paper, “Evidence Regarding Vitamin D and Risk of COVID-19 and Its Severity” — which you can download and read for free — was the second most downloaded study from this journal in the previous 12 months. It was also No. 2 in citations and No. 4 for views.
Other studies have also confirmed that higher vitamin D levels lower your risk of complications and death from COVID-19. Among them is an August 2020 study46,47 published in the journal Nutrients, which found patients who had a vitamin D level below 12 ng/mL (30 nmol/L) had a 6.12 times higher risk of severe disease requiring invasive mechanical ventilation, and a 14.7 times higher risk of death compared to those with a vitamin D level above 12 ng/mL.
Other Conditions Affected by Vitamin D Levels
In January 2022 Mayo Clinic research on vitamin D was featured by WEAU 13 News in Wisconsin. The clinic’s list of conditions affected by vitamin D include:48
Cognitive health — Research shows that low levels of vitamin D in the blood are associated with cognitive decline.
Inherited bone disorders — Vitamin D supplements can be used to help treat inherited disorders resulting from an inability to absorb or process vitamin D, such as familial hypophosphatemia.
Multiple sclerosis — Research suggests that long-term vitamin D supplementation reduces the risk of multiple sclerosis.
Osteomalacia — Vitamin D supplements are used to treat adults with severe vitamin D deficiency, resulting in loss of bone mineral content, bone pain, muscle weakness and soft bones (osteomalacia).
Osteoporosis — Studies suggest that people who get enough vitamin D and calcium in their diets can slow bone mineral loss, help prevent osteoporosis and reduce bone fractures. Ask your doctor if you need a calcium and vitamin D supplement to prevent or treat osteoporosis.
Psoriasis — Applying vitamin D or a topical preparation that contains a vitamin D compound called calcipotriene to the skin can treat plaque-type psoriasis in some people.
Rickets — This rare condition develops in children with vitamin D deficiency.
Check Your Vitamin D Level Twice a Year
Regular, sensible sun exposure is the best way to optimize your vitamin D status, but many will need to take an oral vitamin D3 supplement, especially during winter months.
The only way to gauge whether you might need to supplement, and how much, is to get your level tested, ideally twice a year, in the early spring, after the winter, and early fall when you level is at its peak and low point. This is particularly important if you’re pregnant or planning a pregnancy, or if you have cancer.
Again, the level you’re aiming for is between 60 and 80 ng/mL, with 40 ng/mL being the low cutoff point for sufficiency to prevent a wide range of diseases, including cancer.
GrassrootsHealth makes testing easy by offering an inexpensive vitamin D testing kit as part of its consumer-sponsored research. By signing up, you are helping further vital health research that can help millions in coming years. (All revenues from these kits go directly to GrassrootsHealth. I make no profit from these kits and only provide them as a service of convenience to my readers.)
All women are also encouraged to enroll in the Breast Cancer Prevention project,49 to track your vitamin D level and help prevent an initial cancer occurrence, or, if you’ve already had it, to help prevent a recurrence. In addition, anyone affected by Type 1 Diabetes is invited to enroll in the Type 1 Diabetes Prevention Project.
Required Dosage Is Highly Individual
Research50 suggests it would require 9,600 IUs of vitamin D per day to get 97% of the population to reach 40 ng/mL, but individual requirements can vary widely, and you need to take whatever dosage required to get you into the optimal range.
In 2018 I interviewed Carole Baggerly, director and founder of GrassrootsHealth, a nonprofit public health research organization dedicated to moving public health messages regarding vitamin D from research into practice, and she said:
“Our first paper, published in 2011, showed the dose response relationship. You can easily see that two people taking the same dose (e.g., 4,000 IU/day) could have very different results. That’s why testing … is so important.”
If you’ve been taking a certain amount of vitamin D3 for a number of months and retesting reveals you’re still not within the recommended range, then you know you need to increase your dosage.
Over time, with continued testing, you’ll find your individual sweet spot and have a good idea of how much you need to take to maintain an ideal level year-round. GrassrootsHealth also has an online vitamin D calculator you can use to estimate your vitamin D3 dosage once you know your current serum level.
Additional Guidelines When Using Oral Vitamin D3
Aside from determining your ideal dose of vitamin D3, you also need to make sure you’re getting enough vitamin K2 (to avoid complications associated with excessive calcification in your arteries), calcium and magnesium.
Research51,52 has shown that if you’re taking high doses of vitamin D while having an insufficient magnesium level, your body cannot properly utilize the vitamin D you’re taking. The reason for this is because magnesium is required for the actual activation of vitamin D. If your magnesium level is too low, the vitamin D may simply get stored in its inactive form.
This may actually help explain why many need rather high doses of vitamin D to optimize their levels. According to this scientific review, as many as 50% of Americans taking vitamin D supplements may not get significant benefit due to insufficient magnesium levels.
On the other hand, when you have an optimal magnesium level, your vitamin D level will rise even if you’re taking a much lower dose.53 In fact, previous research54 has indicated that higher magnesium intake helps reduce your risk of vitamin D deficiency — likely by activating more of it.
February 21, 2022, the Canadian Parliament approved Prime Minister Justin Trudeau’s motion to invoke the Emergencies Act in response to the peaceful trucker protest against vaccine mandates
Under the Act, Canadian banks can seize the personal bank accounts of anyone suspected of participating in or supporting the protest, and these financial surveillance powers are intended to become permanent
February 14, 2022, Canadian finance minister Chrystia Freeland said the government was using the Emergencies Act to broaden Canada’s anti-money-laundering and terrorist financing rules to cover crowdfunding platforms and their payment service providers. The broadened surveillance power requires all digital transactions, including cryptocurrencies, to be reported to the Financial Transactions and Reports Analysis Center of Canada. (Fintrac)
What’s happening in Canada should be a sobering wakeup call for the whole world. Governments intend to control dissent through financial blackmail, which is why they’re also pushing for programmable central bank digital currencies (CBDCs)
Programmable currency is digital cash programmed to ensure it can only be spent on essentials or goods that an employer or government deems to be sensible. In other words, the issuer of the money would have complete control over how you spend your own money, and could punish you for undesirable opinions or behavior by restricting your purchasing ability or seizing your funds altogether
February 21, 2022, the Canadian Parliament approved Prime Minister Justin Trudeau’s motion to invoke the Emergencies Act, with 185 votes for and 151 against, in response to the peaceful trucker protest against vaccine mandates.1 While Trudeau in a February 14, 2022, press conference (above) promised the Act would be limited in time, geographical location and scope, he’s already reneging on that promise.
Financial Surveillance Powers Will Be Permanently Expanded
The act was invoked to allow the government to physically disperse the trucker convoy without actually listening to their complaint, and to punish anyone who has supported the protest.
Under the act, banks are empowered to seize the personal bank accounts of anyone suspected of participating in the protest, or supporting it with as little as a $25 donation. Disturbingly, the surveillance powers over financial transactions granted by the act are actually intended to become permanent. As reported by National Review:2
“In a February 14 news conference, Canadian finance minister Chrystia Freeland said that the government was using the Emergencies Act to broaden ‘the scope of Canada’s anti-money-laundering and terrorist financing rules so that they cover crowdfunding platforms and the payment service providers they use.’
That broadened power requires all forms of digital transactions, including cryptocurrencies, to be reported to the Financial Transactions and Reports Analysis Center of Canada. (I.e., ‘Fintrac’).
‘As of today, all crowdfunding platforms and the payment service providers they use must register with Fintrac, and they must report large and suspicious transactions to Fintrac,’ Freeland said.
She justified the move as a way to ‘mitigate the risk’ of ‘illicit funds’ and ‘increase the quality and quantity of intelligence received by Fintrac and make more information available to support investigations by law enforcement’ …
Freeland said the trucker convoy, which had assembled to protest coronavirus restrictions, had ‘highlighted the fact’ that digital assets and funding mechanisms ‘weren’t captured’ by the Canadian government’s pre-existing surveillance powers.
As a result, she said, ‘the government will also bring forward legislation to provide these authorities to FinTrac on a permanent basis.’”
As noted by the National Review, we can already tell what the Canadian government will do with those expanded surveillance powers. We’re seeing their intentions in action. By invoking the Act, Trudeau has given himself the unilateral power to destroy the lives of Canadians who happen to disagree with him, regardless of the issue at hand.
Without court order or due process, the government can now freeze bank accounts, cancel insurance policies and revoke drivers’ licenses, and the victims have no recourse or remedy.
“All this, of course, flies in the face of Trudeau’s promise that the Emergencies Act powers would be temporary,” National Review notes, adding:3
“When he announced his invocation of the order, he promised the Canadian people that his expanded authorities would ‘be time-limited, geographically targeted, as well as reasonable and proportionate to the threats they are meant to address.’ Not a single part of that sentence has proved to be true.”
Government Wants to Decide How You Spend Your Money
What’s happening in Canada should be a sobering wakeup call for the whole world. They’re showing us exactly what’s in store for all of us. Governments will basically control dissent through financial tyranny and blackmail.
The next step in that direction is the implementation of programmable digital currencies, worldwide. As reported by The Telegraph in June 2021, the Bank of England has already started moving on a programmable central bank digital currency (CBDC), and there’s no doubt that this is the plan of all central banks worldwide.4
Executive board member of the European Central Bank, Fabio Panetta, mentioned it in his December 10, 2021, lecture on the future of digital money in Rome, Italy.5
What’s meant by a “programmable” currency? As explained by The Telegraph,6 “Digital cash could be programmed to ensure it is only spent on essentials, or goods which an employer or government deems to be sensible.” In other words, the issuer of the money would have complete control over how you, the recipient, spend it.
“Tom Mutton, a director at the Bank of England, said during a conference … that programming could become a key feature of any future central bank digital currency …” The Telegraph reported.7
“He said … what happens if one of the participants in a transaction puts a restriction on [future use of the money]? There could be some socially beneficial outcomes from that, preventing activity which is seen to be socially harmful in some way. But at the same time it could be a restriction on people’s freedoms.’”
Absolute Control Through Financial Slavery
That programmable currency might restrict freedom is probably the understatement of the century. It’s an absolute given. Imagine your employer, your government and the central bank itself having the privilege to dictate how you spend your own money!
Imagine a third party deciding how much you’re allowed to spend on rent, what kind of food or clothing you’re allowed to buy, or what hobbies you’re allowed to spend money on and when. That’s the power they intend to obtain, and current events in Canada prove it.
The “socially beneficial outcomes” Mutton is hinting at are basically that an unelected cabal will have the ability to micromanage your personal finances, and hence dictate your behavior in every area of your life. As noted by British activist and radio presenter Maajid Nawaz in the Joe Rogan clip above, with a programmable CBDC, the British government would have complete control over anyone who disagrees with their policies or activities.
For example, with other surveillance, they could determine that he was planning to appear on Rogan’s show and simply reprogram his CBDCs with the click of a button, such that he would not be allowed to purchase a plane ticket. So much for that plan then.
Of course, CBDCs will exist by themselves. They’re designed to be used together with digital ID and a social credit score, like that in China. The COVID vaccine passports are one type of platform that could be used for this, but even if a state or country rejects vaccine passports, don’t for a moment think you’re out of the woods, not by a long-shot. Chances are, they’ll introduce a digital ID system instead, which will serve the exact same function.
Global Leadership Has Been Infiltrated
In the full Rogan interview, Nawaz goes on to discuss how governments around the world have been infiltrated by World Economic Forum (WEF) members whose agenda it is to implement global authoritarianism. As reported by Life Site News:8
“… the WEF has installed its members in national leadership roles around the world to further the organization’s sprawling authoritarian agenda. Explaining that government leaders worldwide have begun lifting COVID-19 mandates and restrictions while leaving in place an apparatus of digital tracking and identification that forms the embryonic stages of a digital social credit score.
Nawaz said the WEF under Schwab has worked on ‘embedding people in government who are subscribed to’ the Great Reset agenda. ‘That’s what they say themselves,’ Nawaz said, pointing out that the so-called Great Reset, whose advocates have famously asserted that by 2030 people will ‘own nothing and be happy,’ is explained in detail on the WEF’s website.9
In a 2020 book entitled ‘COVID-19: The Great Reset,’ Schwab openly argued that the COVID-19 response should be used to ‘revamp all aspects of our societies and economies, from education to social contracts and working conditions’ …
The WEF has clearly articulated10its interest in pursuing a global digital ID system. ‘So this is going to be this never-ending process to slowly move the goal posts,’ Rogan surmised. ‘Towards more and more authoritarianism,’ Nawaz added. ‘Checkpoint society. It’s all there. They’ve told us this.’”
How exactly has the WEF infiltrated governments and leadership roles around the world? In part by getting members of its Young Global Leaders group elected or installed in key positions. Would it surprise you to learn that Trudeau went through Schwab’s Young Global Leaders program?
Other members whose dictatorial mindset cannot be disguised any longer are New Zealand Prime Minister Jacinda Ardern and French President Emmanuel Macron. Bill Gates and Facebook founder Mark Zuckerberg have also gone through the program, and both are clearly supporting and promoting The Great Reset agenda through their respective business ventures.
Globalists Plan to Seize Control of Health Systems Worldwide
Your money isn’t the only thing the globalist cabal wants to control, however. In a February 18, 2022, article, Dr. Peter Breggin, author of “COVID-19 and the Global Predators: We Are the Prey,”11 warns that the next move in the globalists’ war on humanity is to seize control over the health care systems of the entire world:12
“We have discovered the next move of the global predators — already in progress — in their escalating assaults against individual and political freedom. The next big assault on human freedom involves a legalized takeover of national healthcare systems by the World Health Organization (WHO).
This stealth attack — with its initial plans already backed by many nations — will begin full implementation in 2024 if it is not quickly recognized and fought! … The Chinese Communist influence over WHO has been solid for more than a decade, and the party was able to install Tedros without any competition.
He became the first and only Director-General who is not a physician and instead is a communist politician. Now the Director-General of WHO, Tedros Adhanom Ghebreyesus — known simply as Tedros — has unveiled plans to take charge of all global health.
While addressing the WHO Executive Committee on January 24, 2022, Director-General Tedros spelled out his global health plan, including his final priority for his enormous scheme: ‘The fifth priority is to urgently strengthen WHO as the leading and directing authority on global health, at the center of the global health architecture.’
Tedros’s closing words to his report to the executive committee are chilling in their grandiosity and echo Marxist exhortations to cheering mobs by a Stalin, Mao, or Xi Jinping: ‘We are one world, we have one health, we are one WHO.’ Tedros seeks to become super-Fauci for the world, and, like Fauci, he will do it on behalf of the global predators.”
Health Fascism
As explained by Breggin, the global health care takeover really began with Gates’ Decade of Vaccines, announced in 2010 at the WEF’s annual meeting in Davos. At that time, Gates installed Dr. Anthony Fauci on his vaccine advisory board, thereby guaranteeing his plans would receive support from the U.S. National Institute of Allergy and Infectious Diseases (NIAID), which Fauci is the head of. Breggin continues:13
“A theme for the Decade of Vaccines was ‘Public-Private Partnerships Drive Progress in Vaccine Development, Delivery’ — essentially the precursor to the Great Reset establishing a world governance of public and private health united in the spirit of fascism.
By 2012, Gates achieved official UN approval for his scheme, establishing a broad network of global predators aimed at exploiting and dominating humanity through public health. Communist China would play a prominent role through its control over the UN and WHO and through its close relationships with global predators like Bill Gates, Klaus Schwab, Mike Bloomberg, Big Tech executives, and many other billionaires and world leaders.
A decade and more later, during COVID-19, WHO has proven its usefulness to the predators in orchestrating science, medicine, and public health in the suppression of human freedom and the generation of wealth and power for the globalists.”
Under the guise of a global pandemic, the WHO, the WEF and all of its installed leaders in government and private business, were able to roll out a plan that has been decades in the making. The pandemic was a perfect cover. In the name of keeping everyone “safe” from infection, the globalists have justified unprecedented attacks on democracy, civil liberties and personal freedoms, including the right to choose your own medical treatment.
Now, the WHO is gearing up to make its pandemic leadership permanent, and to extend it into the health care systems of every nation. “The idea is ‘the principle of health for all’ — universal health care organized by WHO as part of the Great Reset,” Breggin explains.
Pandemic Treaty Is Being Established
May 24, 2021, the European Council announced it supported the establishment of an international Pandemic Treaty, under which the WHO would have the power to replace the constitutions of individual nations with its own constitution under the banner of “pandemic prevention, preparedness and response.”14
“The world has already seen how any pandemic emergency, real or concocted, now or in the future, could then justify WHO taking over the entirety of government operations of sovereign nations, robbing all individuals of their freedoms, and fully crushing the democratic republics of the world,” Breggin warns.15
“The spirit of Communism can be felt throughout the document. We are told that the ‘purpose’ of the new strategy will be ‘guided by a spirit of solidarity, anchored in the principles of fairness, inclusion, and transparency.’ Notice, as in all pronouncements by global predators; there is no mention of individual rights, political liberty, or national sovereignty.
The great engine of human progress, human freedom, will be replaced by the great destroyer of humanity, collectivism, under the rule of the elite. Tucked into the report were the real goals … Here are three main purposes or goals of the proposed treaty:
1.response to any future pandemics, in particular by ensuring universal and equitable access to medical solutions, such as vaccines, medicines, and diagnostics
2.a stronger international health framework with the WHO as the coordinating authority on global health matters
3.the ‘One Health’ approach, connecting the health of humans, animals, and our planet
The report adds, ‘More specifically, such an instrument can enhance international cooperation in a number of priority areas, such as surveillance, alerts, and response, but also in general trust in the international health system.’ Clearly, they were building support for Tedros’s January 24, 2022 announcement that WHO would take over the international health care system.”
Even Your Food Will Be Under Their Control
In addition to your finances and your health care, the global cabal also intend to control the food supply and dictate what you can and cannot eat, in the name of combating climate change and saving the planet. The Great Reset16 is indeed the reset of life and society as we know it. Not a single area will be left untouched.
Sustainable development, Agenda 21, the 2030 Agenda, the New Urban Agenda, the Fourth Industrial Revolution,17 “Build Back Better,”18 green economy, the Green New Deal, the Paris Climate Agreement and the global warming movement in general all refer to and are part of The Great Reset agenda and its resource-based economics.
The common goal of all these movements and agendas is to capture all of the resources of the world — the ownership of them — for a small global cabal that has the know-how to program the computer systems that will ultimately dictate the lives of everyone.
When they talk about “wealth redistribution,” what they’re really referring to is the redistribution of resources from us to them. The goal is for you to own nothing. Everything you need, from the shirt on your back to a roof over your head, you’ll have to rent from the globalist owners.
Even the food you put into your mouth is planned to be under their complete control. To this end, the WEF has partnered with the EAT Forum, which will set the political agenda for global food production. The EAT Forum was cofounded by the Wellcome Trust, which in turn was established with the financial help of GlaxoSmithKline.
EAT collaborates with nearly 40 city governments across Africa, Europe, Asia, North and South America and Australia, and maintains close relationships with imitation meat companies such as Impossible Foods, which was cofunded by Google, Jeff Bezos and Bill Gates.19 Gates has also been gobbling up farmland, becoming one of the largest private land owners in the U.S.20
EAT has developed a “Planetary Health Diet” that is designed to be applied to the global population and entails cutting meat and dairy intake by up to 90%, replacing it largely with foods made in laboratories, along with cereals and oil.21
Not surprisingly, Gates is on record urging Western nations to stop eating real meat altogether,22 and articles have been published in the past three years insisting people need to get used to eating bugs and drinking reclaimed sewage,23 all in the name of sustainability and saving the planet.
Being able to see the globalists’ plan as clearly as we can see it now, we have an obligation to future generations to resist, denounce and refuse any and all implementations of the technocratic agenda. We can win, for the simple fact that there are more of us than there are of them, but we have to be vocal about it — we need to join forces and present a united front, resisting peacefully, like the Canadian truckers.
2017 Video Of Explosion At Ukraine Military Depot Shared As Recent Attack by fake news.
BOOM found that the video shows explosions at a military ammunition depot in central Ukraine in 2017.
A video showing a massive explosion at a military depot in Ukraine in 2017, has been revived and is being shared as recent footage of Russia’s invasion of Ukraine. The video is being shared in the backdrop of full-scale invasion of Ukraine launched by Russian President Vladimir Putin in the early hours of February 24, 2022. Social media has been inundated with unrelated images and videos passed off as the ongoing war. The caption with one such video reads as, “Massive explosion at Ukraine #RussiaUkraineConflict”.
BOOM did a reverse image search on one of the key frames of the video using Yandex – a Russian search engine. We found the same image in an article by the Irish Times, published on September 27, 2017. The caption with the video says, “Explosions at a military ammunition depot in central Ukraine were seen in the early hours of Wednesday, September 27th, 240 km from the capital. Ukrainian Prime Minister Volodymyr Groysman said ‘external factors’ were behind the incident.” Taking a cue from this, we performed a related keyword search on the internet and found several news articles about the incident. According to a Reuters report published on September 28, 2017, “Massive explosions at a military depot in the Vynnytsya region, 270 km (170 miles) west of Kiev, forced the authorities to evacuate 24,000 people…” The report further stated, “It is not clear if the explosions were accidents or sabotage, either of which would underscore poor security at the bases, but officials traded blame for the resulting losses.” The Guardian also uploaded the video on its official YouTube channel on September 28, 2017. The same clip has been used in the viral posts.
It may well be that Russia is saving the world from new American made bioweapons, being more enriched in Ukraine. If it comes out who are behind these biolabs and what kind of bioweapons are being developed and for what purpose, Putin will very likely be able to flip the entire narrative that will boomerang and hit the EU and Americans badly. Most people will be up for a surprise about how much their politicians really care for them and who is calling the shots. Ultimately, the focus has to be on the Satanic banking cartel at the top of society, and the few banking families at the very top.
(Natural News) The financial sanctions Biden has announced against Putin are nothing compared to the Canadian government’s own financial terrorism that it has unleashed against its own peaceful citizens. Donate just $20 to the freedom convoy and all your bank funds can be stolen without notice, completely outside of due process. But we’re told that Putin is the worst villain on the planet. Yet Putin hasn’t stolen anyone’s bank accounts in the USA or Canada (for starters).
For the record, I don’t see Putin demanding Americans and Canadians be injected with spike protein bioweapons that have already killed nearly one million Americans right here at home, either. Those demands came from our own corrupt governments, media propagandists, fraudulent science institutions and pharma-infiltrated Big Tech giants.
Similarly, when the fake Biden president decries Putin’s violation of Ukraine’s “sovereign borders,” the corporate media is utterly silent about America’s invasions, attacks and military violence committed against Yemen, Libya, Iraq, Somalia, Afghanistan, Syria and dozens of other countries. Over the years, the media cheered those attacks, never once caring about how many innocent people would be “displaced” in those countries.
When America attacks innocent nations, it’s never described by the western media as a “brutal onslaught that’s killing innocents.” It’s always described as an effort to “defend freedom.”
Funny, isn’t it, how America’s violence is dressed up as “peace,” but when anybody else does it around the world, suddenly it’s a “brutal onslaught.”
The corporate media is so dishonest in its coverage of conflict that if Ukraine were being invaded by Black Lives Matter with the exact same weapons as the Russian military, we would all be told the incursion was “mostly peaceful” with only “rare” episodes of bombs or missiles.
The lying media has been complicit in the vaccine holocaust that has already killed millions around the globe
Missiles and bombs aren’t the only forms of violence that kill people. Vaccine violence is another concept that’s become crystal clear these days as literally millions of people are now dead from the covid vaccines that were pushed onto innocent people by pharma-controlled governments and complicit corporate media giants over the last 18 months or so.
Thanks to a bombshell “smoking gun” analysis of the covid-19 spike protein, it turns out that Moderna actually patented a particular genetic sequence three years before the covid outbreak… and that sequence is found in the covid-19 spike protein. This is proof that Moderna helped synthesize the virus that got released onto the world, which in turns generated tens of billions of dollars in revenues for Moderna.
In other words, the entire covid outbreak and all its damage — lives lost, economies destroyed, liberties demolished — was done on purpose and was engineered by powerful corporations and governments (NIH, Fauci) in order to deliberately harm humanity. In the world of pure evil, Putin doesn’t even hold a candle to Fauci.
That crime against humanity dwarfs the current events in Ukraine, as devastating as they are. While Putin has launched missiles at targets in Ukraine, global governments and pharma corporations launched a deadly biological weapon against the entire planet, causing untold death, suffering and destruction on a scale that has never been witnessed in the history of human civilization.
Big Media, Big Tech, Big Science, Big Government and Big Pharma all went along with it. They pushed the false narrative that “vaccines are safe and effective” while deliberately conspiring to destroy the reputation of ivermectin and other interventions that could save lives. In a world where Joe Biden claims Russia is “attacking the people of Ukraine,” it was actually Biden’s own government (and Trump’s before) that attacked the people of America with a biological weapon and a fraudulent “vaccine.”
So to anyone that’s going to scream about Putin and Russia, get your crisis hierarchy sorted out correctly so that you at least recognize that Putin’s attack of Ukraine pales in comparison to the USA / CCP attack on the entire world via biological weapons and deadly jabs that transform the bodies of innocent people into spike protein weapons factories.
For the record, we are opposed to all forms of violence against innocent people. That includes kinetic violence, of course, but it must also consider vaccine violence, medical violence, hospital homicide and gain-of-function biological weapons development. Yes, war is bad. Kinetic war is horrible. But so is biological warfare, economic warfare, censorship, government propaganda, journo-terrorism and everything else we’ve all been subjected to under the fraudulent covid narrative.
Putin didn’t make our children wear masks and lock our elderly in nursing homes and hospital beds where you’re not even allowed to visit them. America’s own medical tyrants did that. And they tried to force deadly spike protein shots on everyone, all in the effort to achieve global depopulation and extermination of the human race.
Remember that when you’re watching the propaganda media whine about Russia. CNN has killed far more Americans than Putin has Ukrainians, just from the network’s vaccine propaganda alone.
Get more details in today’s Situation Update podcast here:
Find more information-packaged podcasts each day, along with special reports and emergency updates, at:
Download my current audiobooks — including Ghost World, Survival Nutrition, The Global Reset Survival Guide and The Contagious Mind — at: https://Audiobooks.NaturalNews.com/
A German health insurer BKK ProVita said an analysis of data collected from more than 10 million people suggests COVID vaccine side effects are “significantly” underreported. The company said its analysis revealed a “significant alarm signal” and said “a risk to human life cannot be ruled out.”
By
A German health insurance company this week said an analysis of data collected from more than 10 million people suggests COVID vaccine side effects are “significantly” underreported.
Based on the data collected, BKK said the number of vaccine side effects is many times higher than the number officially announced by the Paul Ehrlich Institute (PEI), Germany’s federal health agency that monitors the safety of vaccines and biomedicines.
The PEI announced in a press release there were 244,576 suspected cases of vaccine side effects reported in 2021 following COVID vaccination, but BKK said its analysis revealed more than 400,000 cases.
BKK board member Andreas Schöfbeck told WELT, a German news publication, “The numbers determined are significant and urgently need to be checked for plausibility.”
In a letter, Schöfbeck said BKK analyzed doctors’ billing data from 10.9 million insured people and found 217,000 people received medical treatment due to vaccine side effects.
“In our opinion, there is a significant underreporting of the side effects of the vaccination,” said Schöfbeck. “According to our calculations, we consider 400,000 visits to the doctor by our insured persons due to vaccination complications to be realistic to date.”
Schöfbeck said if figures are extrapolated over a year for the entire German population of 83 million people, it is likely 2.5 – 3 million people in Germany received medical treatment for COVID vaccine adverse events.
“The data available to our company gives us reason to believe that there is a very considerable under-recording of suspected cases of vaccination side-effects after they received the [COVID-19] vaccine,” Schöfbeck wrote.
Schöfbeck sent the letter to PEI President Dr. Klaus Cichutek, the National Association of Statutory Health Insurance Funds, the German Medical Association, National Association of Statutory Health Insurance Physicians, the Standing Vaccination Commission and BKK’s umbrella organization.
In another letter, the company suggested vaccine side effects across Germany are at least 10 times more common than what was reported by the PEI, the German newspaper Nordkurier reported Wednesday.
The letters did not disclose symptoms, the severity of adverse events or which vaccines caused the side effects.
Federal health officials in the U.S. and Germany have emphasized the benefits of COVID vaccines outweigh the potential risks, and side effects are rare.
In the U.S. last month, an executive at an Indiana life insurance company reported a “stunning” 40% increase in the death rate among 18- to 64-year-old adults compared to pre-pandemic levels, The Defender reported.
During the same call, OneAmerica’s CEO J. Scott Davison also described a major uptick in both short- and long-term disability claims.
The insurance executive rated the extraordinarily high death rate as “the highest … we have seen in the history of this business,” adding the trend is “consistent across every player in that business.”
To further underscore the import of his statements, Davison said, “Just to give you an idea of how bad [40%] is, a … one-in-200 catastrophe would be a 10% increase over pre-pandemic. So 40% is just unheard of.”
Contrary to what the public might assume — given the media’s unremitting coverage of COVID-19 — Davison reported most of the death claims listed causes of death other than COVID.
Commenting on the news, Steve Kirsch, executive director of the Vaccine Safety Research Foundation, wrote, “It would take something REALLY BIG to have an effect this big.”
Moreover, Kirsch said, the culprit would have to be something first introduced in 2021 — “something new … that a huge number of people would be exposed to” — such as COVID shots.
Last year, Philip Dormitzer, the chief scientific officer at Pfizer, described Israel as “a sort of laboratory” to “see the effect” of his company’s vaccines. Well, it took over a year into the vaccine drive that injected most Israelis with three shots and some with four to finally publish information on adverse events. What Israel published earlier this month based on a health ministry survey of 2,049 people who got booster shots is not only damning, but unmistakably revealing that there is no way Pfizer did not see these adverse events during the clinical trials in 2020. What did they know and when did they know it?
On Feb. 10, the Israeli Health Ministry published (English version here) the results of a survey of adverse events among roughly 2,000 random Israelis who received booster shots. It’s shocking that it took this long for them to conduct such a survey and didn’t do this a year ago, but it’s better late than never. Just the top-line numbers from the survey should alarm us all. A total of 75% of women and 58% of men reported experiencing at least one side effect within the 21- to 30-day follow-up period of the interview. Obviously, the majority of these were minor, but 51% of the women and 35% of the men who experienced a side effect reported that as a result, they had difficulty performing daily activities.
Full stop right there. Even before we get into more serious problems. Just the fact that the shot knocked out such a massive percentage of people clearly violates the informed consent through which the shots were marketed and most certainly makes any mandate immoral. Right off the bat, it’s clear that this is not like taking a vitamin D pill. Moreover, the fact that we have zero long-term studies, but such a massive percentage get at least a sick feeling from it in the short run should concern everyone. Again, why wasn’t such a survey done in January 2021 after the first dose?
Just take a look at the massive percentage of reports, especially for females, experiencing weakness, muscle ache, shaking, high temperature, and even dizziness and vomiting.
That is a massive percentage for a product ubiquitously marketed, endorsed, distributed, and then mandated by global governments as the safest and most effective vaccine of all time. And all for a virus that, with most younger people, would cause roughly the same symptoms anyway even after being vaccinated. The fact that this shot was even marketed to younger and healthier people is insane. Yes, some people might have willingly taken a shot if they thought they’d get some flu-like symptoms, but that confidence – that the flu-like symptoms don’t portend more severe long-term damage – can only work for an established vaccine that already has long-term safety data.
Now, let’s get to some of the more serious or potentially serious issues. The same table shows that 5.5% reported experiencing chest pain. We already know that there are major safety concerns for cardiovascular issues and that the spike protein is very pro-inflammatory and potentially thrombotic. And remember, this is 5.5% of just one dose. If you extrapolate that to America, where 551 million doses have been administered, that would be approximately 30 million cases of chest pain! It doesn’t necessarily mean that it causes short-term or long-term damage, but again, with a new vaccine with a novel and dangerous mechanism of action and no long-term safety studies, how can this be allowed to continue without further study?
A total of 4.5% of those who received booster doses reported neurological side effects. Assuming the doses are all relatively the same, that would extrapolate to roughly 25 million cases of neurological side effects in the United States. It would lend a lot of credence to the military whistleblowers who reportseeing more than a tenfold increase in nervous system diagnoses in 2021 and leaves no doubt that the DOD was bluffing when it responded with “revised” data showing not even a modest increase.
There’s no doubt that the spike protein of the pathogen causes nervous system disorders in some people, just like it causes cardiovascular disorders, but clearly the shots do as well, and remember they don’t prevent you from getting the pathogen.
Most of the nervous system disorder reports, on the surface, don’t appear to be that serious, but 0.5% reported Bell’s palsy, which certainly can become very serious. If 0.5% of doses caused Bell’s palsy in the U.S., that would account for 2.7 million doses!
Moving on to more serious issues, 0.29% reported being hospitalized within 30 days. That might sound like a small number, but that is a huge deal for a shot being pushed upon an entire country at once and mandated for many. Assuming the boosters aren’t worse than the previous doses, that would extrapolate to 1.6 million hospitalizations in the U.S. since the beginning of the vaccines 14 months ago, and 270,000 for the boosters, which certainly harmonizes with recent German health insurance claims data, life insurance claims increases in 2021, and Medicare billing data.
Additionally, roughly 24% of people with pre-existing autoimmune disorders, and 5%-10% of those with diabetes, hypertension, and lung and heart disease, also reported a worsening of their condition. Auto-antibodies and autoimmune disorders are always a concern with novel antibody therapies, especially one like this for which the manufacturers brag about a hyper-antibody response.
Also, roughly 10% of women under 54 experienced menstrual irregularities, for which 31% sought medical attention. Delayed menstruation was the most common side effect. While we can’t say definitively that this will cause reproductive issues, such a safety signal is not normal, and in conjunction with the Japanese biodistribution document from Pfizer’s animal study showing lipid nanoparticles, which are pro-inflammatory, depositing in the ovaries, it is the job of the government to prove conclusively that this is not a problem, not the other way around.
And remember, this is all just a survey of the first month following the shots. There is no study on the long-term effects of micro-clotting, heart inflammation, neurological inflammation, immune suppression, antibody-dependent disease enhancement, or auto-immune disorders. We already know that the spike protein circulates potentially for months in some people.
To be clear, this is a randomized survey, not concrete proof of diagnosis. So for those “fact checkers” out there, we are not asserting based on scientific law that the shots absolutely cause X percentage of specific adverse events. But that is not our job. We are not the ones endorsing, marketing, distributing, and mandating the shots. It is their job, after multiple avenues of safety signals showing unprecedented issues, to clean up their act before even continuing the distribution, much less making it mandatory.
There is no way the public would have initially embraced the shots had they been told even the most conservative estimate of adverse events we likely experienced, not to mention the waning efficacy. Which begs the question: What did Pfizer know and when did they know it?
It’s because the life insurance industry is starting to prove there’s a lot of excess deaths happening and it’s not related to covid.
And Wall Street analysts are paying attention to that, many of those Wall Street analysts got vaccinated believing the party line that it was safe and effective, and they’re really pissed off now that they’re finding out the truth.
And yes the vaccine manufacturers were granted liability immunity for the EUA, however as Wall Street knows, if you made a contractual agreement where fraud was occurring then the agreement is null and void.
So if big pharma fudged the clinical test data to get the FDA’s EUA approval, and the vaccine actually caused more deaths in the vaccinated test group, then there was fraud.
So the liability ends up back on the pharma companies.
The life insurance industry dwarfs the pharmaceutical industry and will be looking to place the blame correctly for the liability. Wall Street knows this.
Read this through to its entirety, you’re going to want to see how this plays out.
Wall Street investors are dumping their Moderna and Pfizer stock faster than the world can drop the mandates. Moderna is down 70 percent from its high, while Pfizer is off 19 percent. Former Blackrock Executive and investment adviser Edward Dowd calls for Moderna to go to zero and Pfizer to end under ten dollars per share.
How is this possible given that Pfizer now enjoys record earnings per share and a market capitalization of some $270 billion, making it the 29th largest corporation globally? With nothing but profits in sight for the Pharmaceutical giant, what could be the problem?
After all, in December, a Forbes’ headline read, “The Vaccine Maker Can Dominate The Covid Market For Years to Come, Wells Fargo Predicts.” In addition to the enormously profitable mRNA vaccines, Pfizer is rolling out potent antivirals like Paxlovid, which could earn $22 billion in 2022.
Compared to the $81 billion in 2021 revenue, the earnings from the vaccines and the antivirals could top $102 billion for 2022, which is music to shareholders’ ears. However some are hearing shrieks, and these happen to be Wall Street’s finest, the smart money that beats the rest of the herd to the exits like clockwork.
These sophisticated investors make it their business to not go with the conventional wisdom but to do their own research, which often pays spectacular dividends.
Edward Dowd is one such investor. He saw the dot com bubble ready to burst and acted accordingly. But, unfortunately, other not-so-savvy investors later saw their dot com heavy portfolios collapse as the NASDAQ Composite Index lost 40% of its value in 2000.
Dowd, a graduate of Notre Dame University and former Portfolio Manager at Blackrock, grew his fund from $2 billion to $14 billion and commanded the respect of his investment community peers.
Today, after semi-retiring to the shores of South Maui, he remains a voice of stock market wisdom that many hedge funds continue to rely upon. LinkedIn lists him as a Consultant to Founder & Partner of Symphonic Capital, LLC.
But the dot com collapse is not the only one Dowd successfully navigated. While many other portfolio managers placed their client’s money in highly rated and lucrative mortgage-backed securities, Dowd hesitated and questioned. He considered that those might be grossly over-rated, and he was correct.
It turns out that the mortgage rating system was corrupted by the high profitability of predatory financial products tied to home mortgages. According to Edward Dowd, a large portion of the blame was shouldered by the rating agencies, those trusted organizations whose job it was to judge the risk of these subprime mortgage-backed securities – agencies like Moody’s, Standard & Poor’s and Fitch.
Dowd says they turned a blind eye to the true risk because it was profitable. So, in essence, these rating agencies were captured by the institutions backing these risky subprime securities.
Joseph Stiglitz, a Nobel Prize-winning economist, put it this way, “The incentive structure of the ratings agencies also proved perverse. Agencies such as Moody’s and Standard & Poor’s are paid by the very people they are supposed to grade. As a result, they’ve had every reason to give companies high ratings, in a financial version of what college professors know as grade inflation.”
Dowd has sounded the alarm on Moderna and Pfizer as sinking ships that investors need to abandon. So what does the man who foresaw the dot com and the subprime mortgage crisis have to say about Moderna and Pfizer, and what trouble could exist in the paradise of COVID vaccine profits?
Here are Dowd’s words:
I want to liken here to what’s gone on in the Great Financial Crisis. We had rating agencies, third-party verification sources that were able to perpetuate the fraud because the money got too big, their institutions became corrupted with the institutional imperative, and they got triple-A ratings which we all know in hindsight were not triple-A ratings – let’s move forward to today.
The FDA is the trusted third-party verification of pharmaceutical products. 50% of their budget comes from Pharma…due to the institutional imperative that was in place at the time and the speed with which they tried to approve these unproven products with this unproven technology, fraud did occur, and what’s my proof of that? The FDA, together with Pfizer, were trying to hide the clinical data.
And it’s come out recently…that the all-cause mortality for the Pfizer product failed – that means there were more deaths in the vaccine group than the placebo group. Normally in such a case, you have NO drug approval for such drugs. It’s the gold standard. I’ve been told by all my people in the Biotech Industry they were horrified… See mark 25:10.
And unfortunately, that is not all. Dowd feels that although he has successfully predicted three large frauds in his career, he now expects a global financial market collapse with the debt bubble getting ready to burst.
“So I’ve seen three frauds; the corporate fraud of the dot com boom, the bank fraud of the Great Financial Recession, and I believe the fraud has moved on to central banks and governments – because that’s the nature of our monetary system – you have to constantly create credit to keep this thing going.” See mark 2:22.
“The global debt bubble is at its peak…we are at the end…we are going to see lots of crazy things in the financial markets…we are going to see the credit markets become unhinged, the equity markets become unhinged. The Fed got a reprieve…under the cover of COVID, they were able to print 65% more money to keep this thing afloat, but we are at the end days here.” See mark 3:41.
He clarifies that the emergence of global totalitarianism is not purely about power and profit. Instead Dowd feels it is to control the masses when they realize the economy is collapsing – the ramifications of which may be the loss of pensions and social security income.
“A lot of what you are seeing in the response of global governments is setting up a system – under the guise of medical tyranny – to prevent the riots that are going to ensue once this thing all unwinds – that’s my personal belief…” See mark 4:04.
For the skeptics, consider that Pfizer stock lost $20 billion in market capitalization on February 8, 2022, when their record earnings fell short of more optimistic expectations.
Dowd predicts Moderna will drop to zero with bankruptcy as fraud related to concealing the COVID vaccine dangers surfaces, and he predicts Pfizer will become a sub-ten-dollar stock. Dowd explains that the smart money has already left Moderna and will soon be exiting Pfizer.
Dowd foresees an avalanche of lawsuits coming as the insurance industry continues to uncover the legions of mounting deaths coming from the complications of the mRNA COVID-19 vaccines.
Dowd teamed up with an insurance industry analyst and researched the life insurance claims. They found that since OneAmerica shocked the world by announcing a 40% rise in non-COVID deaths in younger working-class employees, multiple other insurance companies worldwide have seen the same thing – massive rises in non-COVID deaths. And the evidence inescapably points to the vaccines as the cause. See mark 13:16.
Meanwhile, the funeral company stocks have outperformed the S&P. “Funeral Home companies are growth stocks. They had a great year in 2021 compared to 2020, and they outperformed the S&P 500. The peer group of Funeral Home stocks was up 40 plus percent while the S&P was up 26 percent – and they started accelerating price-wise in 2021 during the roll-out of the vaccines – You don’t need to be a rocket scientist to connect the dots here.” See mark 5:55.
Other insurance companies have reported the same or worse death numbers as OneAmerica. For example, “Unum Insurance is up 36%, Lincoln National plus 57%, Prudential plus 41%, Reinsurance Group of America plus 21%, Hartford plus 32%, Met Life plus 24%, and Aegon – which is a Dutch insurer – saw in their US arm plus 57% in the 4th quarter – in the 3rd quarter they saw a 258% increase in death claims.” See mark 07:55.
“They raised (mortality) expectations 300,000 for 2022 over 2021 due to COVID plus ‘indirect COVID,’ which I think we know what that’s code for… They (Aegon) did a
$1.4 billion reinsurance deal with Wilton Reinsurance…what they were reinsuring were high face amount individual policies from 1 million to 10 million… (So) I think there is an asymmetric information situation going on in the insurance industry where some people have figured out something’s going on. They are off-loading their risk – they are not going to say what it is as they don’t want that information to get out as they unload the risk.” See mark 08:49.
“Someone is going to be the bag holder here.” And Dowd is confident it won’t be the insurance industry. A court in France has already held that a life insurance company cannot be held liable for a death because of the mRNA vaccine.
But that does not explain how mRNA manufacturers can be held responsible for an emergency product they were told was liability-free. Aren’t the vaccine manufacturers immunized from lawsuits?
After all, they were granted EUA, the specialized Emergency Use Authorization, which means they cannot be held legally accountable for deaths or adverse effects stemming from the experimental vaccines.
The idea is that no company – upon government request – should have to pay for unforeseen complications resulting from an emergency product that they released to the world out of their goodness of the hearts, with the best of intentions. Right?
Wrong – not when your company accomplishes this through deceit, also known as fraud.
Fraud undoes all these protections. If a company or person intentionally deceives another to profit, we have fraud. If Pfizer’s data showed increased all-cause mortality and hid this to motivate people to take the vaccine while claiming it was safe, then fraud exists.
Under common law, the required elements to prove fraud amount to:
#1. A materially false statement or purposeful failure to state or release material facts which non-disclosure makes other statements misleading.
#2. The false statement is made to induce Plaintiff to act.
#3. The Plaintiff relied upon the false statement, and the injury resulted from this reliance.
#4. Damages include a punitive award as a punishment that serves as a public example to discourage any future similar fraud. Punitive damages are generally proportional to the Defendant’s assets.
Dowd has been researching the COVID-19 vaccines and what he considers obvious evidence of knowing concealment of the actual risks of death – and he points to the Herculean efforts of Pfizer with FDA in withholding their data despite legal challenges to release it. He likens the FDA today to the rating agencies during the Mortgage Crisis.
“FDA is the trusted third party, just like the rating agencies were. And a lot of doctors in this country, a lot of local governments are placing their trust in the FDA which gets 50 percent of its budget from large cap pharma. It wasn’t any one person…I think they overlooked things…An all-cause mortality end-point should have stopped this thing in its tracks – and it didn’t.” See mark 1:51.
There were more deaths in the vaxxed group than in the unvaxxed. Dowd assumes fraud based upon the FDA backing Pfizer in not releasing their data. He believes this is a knowing attempt to conceal the deaths.
“When one party enters into a contract…and fraud was occurring when they entered into that contract, and the other party did not know that – the contract is void and null. There’s no indemnity if this can be proven, and I think it will be.” See mark 4:45.
“Pfizer got blanket immunity with EUA. If fraud occurred, to my mind and what I’m seeing from their refusal to release the data – if there is fraud and it comes out – and we need whistleblowers – and it’s looking more apparent that this product is deadly –
fraud eviscerates all contracts – that’s case law. So you go down the daisy chain, and that’s liability – that’s bankruptcy for Moderna, definitely Pfizer.” See mark 00:51.
He notes that the deaths skyrocketed after the vaccine rollout when they should have dropped. And the deaths are what distinguished the 2021-2022 vaccine scandal as far worse than what happened with Enron.
“People are dying and being maimed. This is a fraud that goes beyond the pale…We have the VAERS data…We have the DoD leak…And now we have the insurance company results and the funeral home results…We don’t need to think too hard about this…Deaths should have gone down after the vaccines rolled out. This is the most egregious fraud in history of the nation – and it’s global…Pfizer’s involved, and they committed fraud,” Dowd explained. See mark 10:25.
“My job is to be ahead of the news and be a lead steer…when I use my stock picking skills outside the realm of stock picking, I am called a conspiracy theorist.” See mark 6:45.
Dowd emphasized that he is not short on Pfizer or Moderna stock. He explained that he does not profit from their share prices dropping. He also points out that his predictions are not the cause of the steep declines as these occurred before he came out with this analysis. See mark 13:45.
“So we don’t need the mainstream media…And I want you to know – Wall Street is rallying to this – I’m getting lots of inquiries from former colleagues. Nothing will convince a sleeping public more than red stocks or collapsing stocks. My goal is to awaken the country by seeing something is going on. And Wall Street is AWAKE!” See mark 2:33.
If money is any indicator, Edward Dowd is correct that insurance will win a fight between the insurance and the vaccine industries. The life insurance market in the US is worth some $900 billion, while the vaccine market pales in comparison.
If someone is left holding the bag, it will not be the insurance industry, but it just might be you and me, the average citizen. However, there is one major caveat – if Edward Dowd succeeds in awakening the citizens, then they – the oligarchs – cannot get away with this – the Vaccine Fraud, the Great Reset, the Fourth Industrial Revolution and Global Totalitarianism.
“There’s lots of people who got the jabs that didn’t understand what was going on. A lot of them are in the investment world. A lot of them are smart people – they were duped too. Some of these people that got the jab are doing the work on shorting these stocks because – you know, you can guess – because they are mad as hell – and you’ve awakened the sleeping giant known as Wall Street. And Wall Street is on the move. The smart money is moving first – as always there’s lead steers. Nothing gets going faster than a red momentum down-trending stock.” See mark 3:26.
Those of you who still think nothing’s going on, you don’t want to be – what I call – the bag holder. You don’t want to be the guy taking the fourth jab booster and holding these stocks (on their way) down – Moderna’s going to zero – I think Pfizer goes sub ten dollars once the lawsuits come out. ” See mark 4:06.
Dowd’s forecast can awaken not only Wall Street but the ordinary citizen. We are those sleeping giants of the world, those who can move mountains with the force of our stock sales and non-violent protests, the great silent majority who can remove dictators from power and elect new and fair leaders.
There is power in numbers, as the Canadian Truckers recently found. Courage is contagious as freedom convoys have sprung up everywhere. We hold the power if we choose to exercise it while we lose that power if we passively comply.
As this Freedom Trucker fireman said, “I don’t know what happened to our country. It’s disgusting. There’s nothing that’s going to be taken from us here today that they’re not going to take anyways – And people need to stand. With enough of us, they can’t do this.” See mark 1:58:10.
If enough of us speak out NOW, collectively, we have the power to not only end the mandates, but to restore ALL freedoms in Canada, Australia, the UK, Europe and the United States, and we will win the day. We will never consent to authoritarian rule.
We will not leave a world of slavery to our children and grandchildren. We will protest every single day until the government realizes who truly is in charge. We believe in government of the people, by the people, and for the people. The cure for 1984 remains 1776.
Edward Dowd cautions those who continue to slumber, “If you are long these two stocks, you are long mandates, you are long government control, and you are long the selling of your freedoms.” Let us get everyone on board the freedom train. See mark 15:16.
One of the most important realizations emerging from the fake Ottawa “police” (many of whom turned out to be UN troops with no legal authority whatsoever) is that the globalist cabal doesn’t have enough people to carry out their tyranny. They have to recruit mercenaries from other regions and pay them to brutalize the local people under tyrannical authoritarianism.
— Is this the Holy Grail in Medicine?
Denied by Big Pharma, MMS has proven to be a cheap and effective treatment/cure for virtually every ailment under the sun!
Trump was right… chlorine dioxide cures. It is NOT Bleach as the media claimed, it is safe and natural.
This documentary (mirror) produced by Adam Abraham working with Jim Humble in Mexico tells the story of MMS and many of the accomplishments that has occurred since Jim first wrote the book that is sold on his site – The Miracle Mineral Solution of the 21st Century. There are excerpts and testimony from doctors and scientists in Mexico and the US.
Jim is an ex miner who first witnessed it’s use for treating malaria and has since gone on to investigate the possibility of treating a variety of other ailments and diseases ranging from coughs and colds, flu, tuberculosis, lime disease, psoriasis and cancer.
Quite a number of other people give their opinions and observations who all attest to the effectiveness of MMS.
This documentary is very professional done and it gives you a very interesting look into the new world of MMS. The observations and happenings are all factual.
Please enjoy this documentary and share it with all your friends and family.
The Universal Antidote Getting Started Series-Complete Series
Training Video 6 – How to Make the Acid Activator
Training Video 5 – How to make 22.4% Sodium Chlorite Solution (MMS)
How to make fresh cds every day Last updated 02/23/22
Vaccination Detox
MMS/ Jim Humble/ sodium chlorite- Great Detox claims it cures cancer… ALSO DEACTIVATES GRAPHENE FUNCTION. I do use MMS on a daily basis, be very careful start off with 2 drops of each solution. Add 2 drops MMS then 2 drops activator in small glass, swirl for 30 sec, add 4 oz of water, drink on empty stomach, no food 1 hour before/after. Move up to 3 drops after a couple weeks. Read Jim’s book above.
Detox Bath Recipe Removes: Radiation Poisoning / Pesticides / Heavy Metals / Parasites / Nano Bots / Graphene Oxide (Black Goo) / Chemtrails / Jabs & More
A. External Detox
Take a hot bath with:
2 cups of Baking Soda
2 cups of Epsom Salt
1 cup of Bentonite Clay (Aztec Secret Indian Healing Clay)
1 cup of Borax (removes Nano Bots)
Scrub down for 20 minutes.
Then shower with Dr Bonner peppermint liquid soap and scrub your body after soaking.
Cure 4 the VAXXED to DETOX Toxic Chemicals
100 mg of Zinc per day. A virus cannot replicate in the cell when there is enough Zinc in the cell.
Preventative dosage:
* IVERMECTIN: 12 mg / wHCQ: 300 mg / w
* Vitamin C – minimum 5000 mg / d (work upto 10000 mg / d)
* Magnesium – 500 mg / d
* Selenium – 200 mcg / d
* Apple Pectin – 700 mg x 2 / d for the jabbed 6 months.
* Zinc – 100 mg / d
* Vitamin D – minimum 5000 IU / d
Pass this around I hope and pray it works for the vaxxed! We can also do the detox even if you did not take the jab. We all have nanobots and will help with the spreading of spike proteins from the jabbed.
STORY AT-A-GLANCE
Nebulized hydrogen peroxide is a safe, inexpensive and incredibly effective way to prevent and treat viral illnesses of all kinds
While hydrogen peroxide kills viruses, it also kills other pathogens that can contribute to an unhealthy gut and/or oral microbiome. As such, it may also improve your microbiome and help resolve a wide variety of other chronic ailments, including gut problems and periodontitis
Hydrogen peroxide is part of your body’s natural defense against pathogens. So, when you nebulize hydrogen peroxide, you’re really just augmenting your body’s natural defense system
Being able to treat yourself at home at the rst signs of COVID-19 symptoms will also virtually eliminate your risk of long-haul syndrome. So far, medical doctors who have treated COVID-19 patients agree that if treatment begins early enough, patients almost always fully recover and have no longstanding side effects from the infection
Buy the required supplies before you need them, so you have everything and can treat yourself at the rst signs of symptoms. Most of the time, after two or three treatments, the infection will be stopped in its tracks.
I used these to make .5% H2O2, less than $15 for both.
(Natural News) From now on, Public Health Scotland (PHS) will no longer publish its weekly data reports on Wuhan coronavirus (Covid-19) “cases,” hospitalizations, and deaths because the government agency claims that the information is being “misused” by people who oppose the “vaccines.”
The announcement came after a former adviser to the Trump administration told a United States Senate committee hearing that data from Scotland “demonstrates conclusively that the vaccine is driving massive infections in the vaccinated,” which is clearly seen in the numbers.
Paul E. Alexander, an epidemiologist and Canadian health researcher, has long advocated for a strategy of mass infection of the public, rather than mass injection, in order to build herd immunity. His strategy rings truer than ever amid growing evidence that the jabs are sickening and killing people.
During a hearing chaired by Sen. Ron Johnson (R-Wisc.), Alexander explained how the PHS data is a “big, big problem” because it clearly shows that the shots, which were introduced by Donald Trump under Operation Warp Speed, are dangerous and ineffective at preventing infection.
Alexander presented PHS data for the week beginning on January 22 showing that the age-standardized covid case rate per 100,000 in Scotland was 381.5 among the unvaccinated compared to 570 in the double injected. In the triple injected, that figure was 447 per 100,000.
“It was the first time that the case rate among boosted individuals had overtaken the unvaccinated, with the case rate among the double-vaccinated first pulling ahead of the unvaccinated group in December as the Omicron wave exploded,” reports Herald Scotland.
“Similar patterns are being seen in other countries including England and Ontario in Canada, but PHS officials stress that it has been misunderstood.”
Scotland now intentionally concealing jab injuries, deaths
PHS still plans to publish data monthly rather than weekly, however that data will change to report information on jab efficacy against infection based on trials and real-world studies, reports explain.
Scottish officials are accepting the fact that these sudden changes will be viewed as a “cover-up” by people who are paying attention to the situation, but they simply do not care what people think anymore.
Another thing to consider is that the decision to scrap the old ways of reporting occurred after the hospitalization and mortality rate doubled among the vaccinated in Scotland, overtaking the unvaccinated for the first time during the spread of omicron (moronic).
Because this clearly showed that the jabs were not working, Scotland scrapped the reporting and is now switching to something less damning for the injections.
“The main important point around all of the analysis is we understand whether the vaccines are working against catching it and against getting severe Covid, and that’s where the vaccine effectiveness studies come in which are a completely different methodology,” claimed a spokesman for PHS.
“The case rates, hospitalisation rates, the death rates are very simple statistics, whereas for the vaccine effectiveness studies we use modelling, we compare people who have tested negative to those who have tested positive and match them on their underlining co-morbidities.”
The spokesman went on to claim that the new method is “much more robust and that’s what we want people to focus on.”
In other words, the authorities do not want people focusing on the truth, but rather the deflection. Anything to make the jabs look good rather than bad is on the table as an option moving forward.
“The problem is this vaccine does not stop transmission, does not sterilise the virus … you can never get the population herd immunity to 100% with these vaccines – impossible,” stated Alexander during the Johnson hearing.
More of the latest news about covid injections can be found at ChemicalViolence.com.
In an article that hasn’t received much attention from mainstream media, Chris Martenson, cofounder and CEO of Peak Prosperity, details a report from a January 2022 issue of the medical journal JAMA.
The bottom line is that getting an mRNA shot increases your risk of myocarditis by 133 times.
A survey conducted by the Israeli Minister of Health found so many reports of serious adverse events after getting the COVID-19 shots that they started wiping them from their Facebook page.
Literally thousands of comments had piled up before the ministry started deleting them. What’s concerning is that instead of investigating the reports or asking why so many weren’t returning for their second shots, the ministry simply erased the reports. Then, to add insult to injury, the ministry claimed they’d received “so few reports” after the booster shots that it showed that getting a booster was “extremely safe.”
Interestingly, a look at publicly available data tell a different story, with tens of thousands of reports of major injuries such as Bell’s palsy, seizures, shingles, neurological problems and worsening of diabetes, hypertension and heart and lung disease after receiving the shots.
A ground-breaking review of U.S. and U.K. data shows that all age groups under age 50 are at greater risk of dying after the COVID-19 shots than an unvaccinated person is at risk of a COVID-19 death.
Not only that, the younger ages “incur significant risk,” the study finds. Specifically, the results by age cohort are that within the same or subsequent month of receiving a COVID “vaccine” inoculation:
• For those under age 18, vaccination increases their COVID death rate, and those under 18 are 51 times more likely to die from the inoculation than to die from COVID if not vaccinated.
• Those aged 18 to 29 are 16 times more likely to die from COVID vaccination than to prevent one COVID death and are eight times more likely to die from vaccination than to die from COVID if not vaccinated.
• Those aged 30 to 39 are 15 times more likely to die from COVID inoculation than to prevent one COVID death, and seven times more likely to die from the inoculation than to die from COVID if not vaccinated.
• Those aged 40 to 49 are nine times more likely to die from the COVID inoculation than likely to prevent one COVID death in this age group, and five times more likely to die from the inoculation than to die from COVID if not vaccinated.
• Those aged 50 to 59 are twice (two times) more likely to die from the COVID inoculation than to prevent one COVID death and are slightly more likely to die from the inoculation than to die from COVID if not vaccinated.
• Those aged 60 to 79 are virtually equally likely to die from the COVID inoculation as to prevent one COVID death or die from COVID if not vaccinated.
• Those aged 80+ are 0.13% less likely to die from the COVID inoculation than to die from COVID if not vaccinated.
This article was written by John Roulac and originally published here.
Until recently, most Americans had little trust in the FDA. But when COVID arrived in early 2020, a scared nation deepened in tribal identity and then turned its faith and trust over to FDA and CDC. Interestingly, during COVID, medical professionals’ trust in the FDA and CDC plummeted. Let’s explore how American perceptions of the FDA have changed and what this faith has delivered to our nation.
In 2008 I obtained a letter written by an FDA official, which was sent to a competitor of Nutiva (the organic foods brand I founded in 1999). It warned firms to remove any reference to ‘non-GMO’ on food labels. Virtually every natural food brand quickly changed their labels. As CEO of Nutiva I determined that the warning was not based on any FDA regulation, but was an illegal abuse of power by an FDA official serving the interests of the GMO industry.
We chose to ignore the letter, and luckily I never heard from the agency. This is just one of many examples of the FDA’s suspect moves over the past decades.
The FDA has failed to regulate a toxic food system of dis-ease, inflammation, and the destruction of nature via harsh pesticides, leaving Americans with weakened immunity and vulnerability to pathogens. Tragically the U.S.A. has one of the highest COVID death rates in the world.
The FDA Has Been a Case Study of a Captured Agency
From the 1980’s thru 2019, the FDA was not considered trustworthy by the American people and was often described as “corrupt, filled with cronyism, or a captured agency”.
During the 1980s groundswell of the organic food movement, many Americans realized that Monsanto and the chemical industry’s cozy relationship with the FDA was a major issue. Most liberals were not happy with FDA policies that became the target of many legal campaigns over the safety and efficacy of GMO foods, pesticides and drugs.
In 1990, the FDA set out to make dietary supplements prescription only. The industry unified and rallied to pass the DSHE Act, legalizing supplements as foods.
There has been a revolving door of chemical and pharma executives between the FDA and industry, as was the case in 2009 when ex-Monsanto executive Michael R. Taylor was hired as the FDA’s food czar. Corn oil and corn syrup were given a pass, while eggs and beef were considered unhealthy.
Then came Scott Gottlieb MD, the former FDA Commissioner from 2017 to April 2019, where in June of 2019, he became a Director at Pfizer and Chair of their Regulatory and Compliance Committee.
In fact, as documented by the international news organization Quartz, “as of 2019, nine out of the last 10 FDA commissioners – representing nearly four decades of agency leadership – have gone on to work for pharmaceutical companies.
FDA approval of dangerous drugs such as Prozac and Vioxx has been standard operating procedure. Back in 2012, CBS’ 60 Minutes exposed collusion between the pharmaceutical industry and the FDA on anti-depressants. The majority of FDA’s drug budget is in fact funded by the pharmaceutical industry.
In 2013, a report published in the Journal of Law and Medicine summarized by Dr. Donald W. Light highlighted that ‘about 90 percent of all new FDA approved drugs over the previous 30 years were found to be little or no more effective for patients than existing drugs’, that ‘the bar for “safe” was equally low, even when properly prescribed’, and that ‘125K excess deaths occurred in the United States each year among people taking properly prescribed drugs to be healthier.’
A fall 2019 Gallup Poll ranked the pharmaceutical industry as the most poorly regarded industry in Americans’ eyes. Americans were more than twice as likely to rate the pharmaceutical industry negatively (58%) as positively (27%).
The deepening of tribal identities, Trump zig-zagging at the helm of the pandemic response, and the presence of the QAnon conspiracy movement caused an even deeper distrust of anything associated with Trump, including the FDA. By October 2020, trust in the FDA was at an all-time low.
Shifting Tides
Ironically, this all changed when Joe Biden assumed office. Liberals and democrats flipped rapidly from FDA skeptics to FDA cheerleaders in a matter of months, the perverse logic seeming to be “We hate Trump and now we are on Team FDA-Pharma”.
In May 2021, a Pew Research Poll found that the share of adults who are “basically content” with the federal government had risen to the highest point since 2004, driven by Democrats. In July 2021, an Annenberg Public Policy Center Poll found that 77% of Americans were confident that the FDA was providing trustworthy information about treating and preventing COVID-19.
Interestingly enough, at the exact same time that the general public’s trust in the FDA and CDC was soaring, healthcare professionals’ trust in the FDA and CDC was dramatically decreasing. A group of 20 + medical professionals spoke at a U.S. Senate Roundtable on January 24, 2022 (skip ahead to 51:28).
Perhaps the views of many of these healthcare professionals have not been able to reach the general public because MDs and nurses regularly face termination or threat of medical board decertification for publicly speaking of vaccine injuries, low cost effective treatment protocols, or on other matters that don’t fit the current approved narratives.
The FDA Now Is Trustworthy, Credible and Authoritative … Really?
It appears the majority of left-leaning Americans believe that the FDA has their best interests at heart regarding COVID policies and are obeying them without question. As leading clinical MDs remind me, much of what Americans base their opinion on is often simply pharma marketing claims disguised as medical science.
In a world of corruption, brainwashing, and dishonesty, it’s not easy to know whom to trust. It’s a classic example of mass formation psychosis, where people adhere to groupthink in order to find meaning and resolution in uncertain times, no matter how irrational.
It’s a stunning sociological study to see a mass population trusting leaders of companies with very low ethical standards. Just months ago, most would never agree to be injected with an experimental genetic drug therapy every six months based on FDA edicts. Upon shot five or six under threat of job loss or travel ban, and mounting vaccine injury reports, will more Americans resume asking good questions?
Repeat After Me …
Many Americans are repeating the FDA and the pharma sector’s slogan of “Vaccines are Safe and Effective”, almost like the pledge of allegiance to the flag, while ridiculing or ignoring other proven preventative and early treatment measures (as outlined in my recent article ‘Pharma’s Culture War’).’
Thousands of practicing MDs along with the Front Line COVID-19 Critical Care Alliance (FLCCC) agree that having more tools in the toolkit is wise and that “Early Treatment of COVID is Safe and VERY Effective”.
MDs and countries from around the world who focus on early treatment send very few patients to the hospitals, whereas countries with high vaccine rates such as the EU, UK, and the U.S.A. have some of the highest death rates in the world. Regions such as Africa and Northern India (until recently) had very low rates of vaccination and very low COVID cases and deaths.
Tokyo, Japan and Delhi, India’s COVID cases in the latter half of 2021 were 175 to 2000 times less than London or NYC (see graphic and data below) and their COVID hospital beds were virtually empty. These regions often used early treatment protocols to reduce the spread.
Oddly many Americans cheering on the FDA have little awareness of why other countries are doing much better than the USA. Why is that not in the news? What is the connection of early treatment, inflammation, diet, toxic pesticides, soil health, gut biome and industrial agriculture?
Suppression of Safe and Effective Treatments
The FDA, media, and the pharma sector have ignored the overwhelming benefits of Vitamin D and lifestyle choices. An Israeli study offers the strongest proof yet of Vitamin D’s power to fight COVID. “We found it striking, to see the difference in the chances of becoming a severe patient when you are lacking in Vitamin D compared to when you’re not,” said Dr. Amiel Dror, a Galilee Medical Center physician.
The U.S. media virtually never publishes positive articles on Vitamin D, which often appear in international media. Why has the FDA and the media not published statistical COVID hospitalization and death data on Vitamin D levels or on inflammation? Why have most Americans not bothered to pay attention to their Vitamin D levels?
Before COVID, the FDA never issued edicts preventing doctors from prescribing low cost and re-purposed medicines. 20% of all medicines prescribed in the U.S.A. today are generic repurposed, (e.g. a heart drug given to a cancer patient). Clinicians do this every day and no long term studies are required, since safety data is already established.
Fluvoxamine, !vermect!n, Nitazoxanide and Hydroxychloroquine are safe, commonly prescribed medicines and are part of the FLCCC COVID treatment protocols. According to Pierre Kory, MD “Since the summer of 2020, U.S. public health agencies have continually shut down the use of generic treatments.
The National Institutes of Health (NIH) funded 20 large research studies of patented pharmaceutical industry drugs before only recently agreeing to study repurposed generic medicines.”
The fact that doctors at the bedside are being fired or prevented from providing life saving vitamins and medicines is truly a black mark in America and has likely contributed to a significant number of unnecessary deaths. Instead they are told to use the highly toxic Remdesivir which can cause renal failure and hospitals are paid bonuses for treating COVID patients with this drug.
Censorship Is Now a Liberal Value?
Many liberals now want to cancel, restrict or censor their perceived ‘tribal enemies’. Some scream about medical issues that they have little or no training in as if they are judge and jury, and maybe even represent science itself as Dr. Fauci has alluded to. Easily triggered, they often refuse to even listen to the world-renowned MDs and scientists that they are criticizing or read the published science themselves.
Recently, Joe Rogan’s podcast came under fire, accused of promoting ‘COVID misinformation’, for hosting Dr. Peter McCullough and Dr. Robert Malone. Dr. Peter McCullough is the former Vice Chief of Internal Medicine at Baylor University Medical Center and is one of the most published authors in his field with 600 citations in the National Library of Medicine.
Dr. Robert Malone is one of the principle inventors of mRNA vaccine technology. Both hold views on COVID treatment and COVID vaccines that fall outside the mainstream ‘FDA-and-CDC-approved’ narratives, though neither are anti-vaccine. Neil Young and Joni Mitchell jumped in (unsuccessfully) to help ‘cancel’ Joe’s podcast as other artists followed with support from the woke mob (see: Not Your Cuppa Joe? Here’s a Thought: Move ON).
It seems absurd, yet Americans and our media now tar and feather anyone who dare question the approved narratives. Wokeism is now becoming the tip of the spear for the pharma industrial complex to cancel those that fall out of line. Facebook is now even starting to ‘fact check’ regenerative agriculture posts that mention holistic grazing with climate benefits.
Dissent = Misinformation
Dissent, and even skepticism is now being dangerously characterized as “misinformation”, while pharma marketing claims are now often labeled as “science”. It’s almost as if Orwell’s ‘newspeak’ is coming to life in realtime.
To even question the “Vaccines are Safe and Effective” narrative means possible loss of work or family drama. The ‘take the vaccine not for your health but to protect your mother’ mantra was repeated ad nauseum, despite the fact that you can still get COVID, spread COVID, and die from COVID even if you are vaccinated.
With the growing vaccine injury issues of the mRNA jabs, Israel (which currently has one of the highest COVID death rates in the world- despite 4 jab booster regime) recently ordered 5 million non-genetic, non mRNA ‘old school’Novavax vaccines.
A report reviewing data in the U.S. Vaccine Adverse Event Reporting System, co-authored by Dr. McCullough and Dr. Jessica Rose, a virologist and epidemiologist in Canada, found that the relative risk for myocarditis is increased by 19-fold in age 12 to 15-year-old males following the second mRNA vaccination compared to background myocarditis rates for this age group.
Interestingly, the report was pulled without a clear reason or explanation one week before the CDC deadline to review vaccine safety data in children.
A recent preprint from Kaiser Permanente Northwest also concluded that ‘the true incidence of myopericarditis is markedly higher than the incidence reported to US advisory committees’ and that ‘the VSD should validate its search algorithm to improve its sensitivity for myopericarditis.’
“Vaccine effectiveness” is another interesting term. Early epidemiological data is showing reduced rates of hospitalization and death in groups that are at higher-risk for developing severe COVID. However, there is now overwhelming evidence that the vaccines are not effective in preventing you from getting or transmitting COVID. Thus is this term ‘safe and effective’ based on sound science or should it have a qualifying statement to go along with it?
Weaponization of Vaccination Status
Mandates and vaccine passports based on experimental genetic vaccines (many of which were never officially approved by the FDA) are violations of the Geneva Convention, and arguably violations of the Nuremberg Code and human rights in general. One’s right to a job or going to your favorite café is now dependent on draconian and ever-changing rules.
California governor Gavin Newsom’s announcement of the lifting of indoor mask mandates only for those vaccinated, besides not being based on science, is divisive and antagonistic. Two shots were not enough and shortly three will be required to be a “member of society”, and soon perhaps four, five or more. Do Americans still have the right to life, liberty, and the pursuit of happiness?
Waking Up (From the Woke?)
It’s truly strange times when your close friends or family would unwittingly rather have untold numbers of Americans die of a treatable disease (which must all be “misinformation”). However, a growing number of people are beginning to question the failed COVID policies.
Sweden, Switzerland, Denmark, Norway, Finland, Ireland, Netherlands and the UK have all started to lift COVID restrictions. Remember when liberals used to suggest the U.S.A. should follow Scandinavian countries like Denmark?
Every day more people learn of the growing vaccine injuries or censorship of low cost repurposed medicines. Many are beginning to worry about the lack of transparency, misleading narratives, mandates and censorship, yet are afraid to say anything for fear of attacks on their reputation.
Regeneration
It’s certainly fascinating to watch this unfold. Will public support fade for vaccine mandates, vaccine passports, school masking, and firing MDs for practicing medicine at the bedside? Will we gain the understanding of the linkage between soil health, pesticides, our gut biome health and regenerative agriculture (my 2021 article discusses this issue in more depth) as a key to boosting our personal and planet’s health?
As we shift from this pandemic to endemic phase, let’s make an extra effort to play more and nurture ourselves and our community. It’s time. Let’s regenerate.
As the media are abandoning COVID, they’re taking aim at AIDS instead. The timing of AIDS-related articles and announcements is indicative of a coordinated PR campaign, which must have a specific purpose
While Prince Harry’s fame is milked for all it’s worth to get people to start thinking about getting HIV-tested, the discovery of a new HIV variant in The Netherlands has also been announced. The variant is more contagious, and causes more severe disease, twice as fast. There are 109 known cases of the HIV variant in The Netherlands
The COVID jab may be causing AIDS-like illness by decimating immune function. Researchers have also warned the COVID jab may raise your risk of HIV infection. Is the media’s focus on AIDS an attempt to cover up COVID jab effects?
The same week as Prince Harry’s media appearance and the publication of the new HIV strain, Moderna announced its launch of a human trial for the world’s first mRNA HIV vaccine
The parallels between Dr. Anthony Fauci’s AIDS campaign in the ‘80s and COVID are strikingly similar. In the ‘80s, Fauci pushed the deadly drug AZT as the only permissible way to treat AIDS. During the COVID pandemic, Fauci’s failed and lethal Ebola drug remdesivir got the greenlight at the expense of far safer treatment alternatives. Fauci has also been pushing for a transition from conventional vaccines to the mRNA platform
When media start raising an issue all at the same time, it’s usually a coordinated campaign directed by a PR company on the behalf of a client. There’s a reason for it, and the reason is to sow a desired narrative in the minds of people. They plant ideas so that when something happens, people are already prepped with certain prejudices or assumptions.
So, what then might be the reason for everyone suddenly talking about AIDS? In December 2021, President Biden announced a White House plan to “end the HIV/AIDS epidemic by 2030.”1 The same exact vow had been announced by the British Health Security Agency a week earlier.2
Meanwhile, Prince Harry was out there urging everyone to get an HIV test, and Dutch researchers announced the discovery of a concerning HIV strain. All of this is happening at the same time that COVID is starting to fade out.
As noted by Off-Guardian,3 “just because they’re giving slack on COVID does not mean the agenda behind COVID is gone. Far from it. In fact, even as they seek to dump this pandemic in a shallow grave, they are already prepping the public for the next health scare — AIDS.”
Prince Harry Urges Everyone to Get Tested for HIV
In recent weeks, Prince Harry has been making the rounds urging people to get an HIV test. According to a February 10, 2022, report by the BBC,4 “the Duke of Sussex … wants to continue his mum’s ‘unfinished’ work in removing the stigma around the virus.”
Prince Harry has pointed out that during the last two years, HIV testing among heterosexual men and women in the U.K. has dropped by 33%, compared to just 7% lower testing rates among gays and bisexuals. At the same time, AIDS diagnoses among heterosexuals are outpacing those among gays for the first time in a decade.5
Similarly, a February 9, 2022, opinion piece by Ian Green, chief executive of the Terrence Higgins Trust (a British charity that provides HIV-related services), in The Guardian highlighted the need for a “new strategy” to combat HIV. “Continuing to solely target those traditionally most at risk won’t work,” he said. The answer, according to Green, is more widespread testing of all people, regardless of preconceived assumptions about risk.
New, More Infectious HIV Variant Discovered
While Prince Harry’s fame is milked for all it’s worth to get people to start thinking about getting HIV-tested, the discovery of a new HIV variant in The Netherlands has also been announced.6 Is that a coincidence?
According to researchers, this mutated HIV virus, dubbed the VB variant, is more infectious and causes more severe illness, twice as fast. As of early February 2022, there were 109 known cases of the VB variant in The Netherlands. Curiously, scientists said the variant had been circulating for decades. As reported by NPR, February 4, 2022:7
“They discovered a total of 109 people who had this particular variant and never knew it, dating all the way back to 1992. The variant probably emerged in the late ’80s … picking up steam around 2000 and then eventually slowing down around 2010.
People with this variant have a viral load that is three to four times higher than usual for those with HIV. This characteristic means the virus progresses into serious illness twice as fast — and also makes it more contagious …
There’s no need to develop special treatments for this variant … It shows no signs at all of resisting medications, as some HIV variants do. But because the variant moves quickly, people need to receive medicine as fast as possible.”
Researchers said they also observed a large rise in viral load in individuals with this variant by a 3.5 to 5.5 point increase. What this means is that infected persons could develop AIDS faster without immediate treatment; which could explain the sudden call for mass testing, They wrote:8
“By the time they were diagnosed, these individuals were vulnerable to developing AIDS within 2 to 3 years … Without treatment, advanced HIV — CD4 cell counts below 350 cells per cubic millimeter, with long-term clinical consequences — is expected to be reached, on average, 9 months after diagnosis for individuals in their thirties with this variant.”
Are We Looking at Vaccine-Induced AIDS?
To all of this we can also add the concern that the COVID jab may be causing AIDS-like illness by decimating immune function.9 This is not to imply the shot is causing HIV/AIDS.10,11 Rather, a Lancet preprint12 that compared outcomes among “vaccinated” and unvaccinated Swedes found that six months’ post-jab, some of the more vulnerable vaccinated groups were at greater risk for symptomatic COVID than their unvaccinated peers.
Clearly, the jabs are making some people MORE prone to infection and serious disease rather than less so. According to a December 2021 article posted by the American Frontline Doctors:13
“Doctors are calling this phenomena in the repeatedly vaccinated ‘immune erosion’ or ‘acquired immune deficiency,’ accounting for elevated incidence of myocarditis and other post-vaccine illnesses that either affect them more rapidly, resulting in death, or more slowly, resulting in chronic illness.”
In other words, they suspect myocarditis and other chronic health problems associated with the jabs could be the result of vaccine-acquired immunodeficiency syndrome or “VAIDS,” which is basically very similar to AIDS. The main difference is the initial trigger. In November 2021, the U.K. also reported a 50% increase in ICU admissions of patients with immune system problems in the preceding two months.14
America’s Frontline Doctors warn the shots are creating “vaccine addicts,” in the sense that their immune system won’t be able to ward off COVID without them. However, it’s still a losing venture, as each shot only worsens the immune erosion, making you ever more vulnerable to all kinds of infections — including HIV! As reported by Off-Guardian:15
“We have already seen a plethora of predictions of increases in strokes and heart attacks, all attributed to very much non-vaccine causes. Everything from increased energy prices to lockdown-related depression has been blamed. That certainly appears to be pre-emptive ass-covering behavior. And this ‘new variant’ of AIDS could be too.
If the COVID ‘vaccines’ cause millions of people to suddenly develop dysfunctional immune systems, or some kind of antibody-dependent enhancement a ‘more dangerous new strain of AIDS’ is a pretty good cover story, don’t you think? …
In October 2020 one group of researchers, quoted in Forbes, warned that any potential COVID ‘vaccine’ could increase your risk of being infected with HIV.
One of the few abandoned COVID vaccine candidates, from the University of Queensland, actually used a protein from HIV as a ‘molecular clamp’ to bind their artificial spike proteins together, the researchers claimed. This potential ‘vaccine’ was apparently discarded after test subjects returned ‘false positives’ on HIV tests.16”
What’s the PR Campaign Trying to Hide?
We’re looking at several big puzzle pieces here:
Prince Harry and others reminding everyone about the importance to get tested for HIV
U.K. and U.S. governments simultaneously promising to eradicate AIDS by 2030
The discovery of a new, more infectious and dangerous HIV strain
Emerging data suggesting the COVID jabs erode your immune function
The theoretical possibility that the COVID jab might raise people’s risk of HIV infection, thus possibly triggering an avalanche of AIDS cases in the near future
Could the focus on HIV testing, especially in combination with the warning of a new HIV strain, be an effort to hide the fact that the COVID jabs are destroying people’s immune function, and possibly promoting HIV infection?
Perhaps. But there’s also another possibility. The same week as Prince Harry’s media appearance and the publication of the new HIV strain, Moderna also announced its launch of a human trial for the world’s first mRNA HIV vaccine. The timing of all of these reports strongly indicate that this is a coordinated PR plan.
Human Trial for mRNA HIV Vaccine Is Underway
As reported by Bloomberg:17
“Like Moderna’s COVID vaccine, the shot uses mRNA technology to deliver the instructions for key proteins needed to build an immune response … Researchers have spent decades working out a possible way to inoculate people against HIV, and mRNA will make it possible to test the theory much faster than expected.
This work should help companies including Pfizer, BioNTech and Sanofi, all accelerating their own efforts to design and test mRNA vaccines, to understand when the technology can — and can’t — make a difference in disease prevention …
Creating an mRNA vaccine for HIV is trickier than making the kind of SARS-CoV-2 shots we’ve become familiar with. The mRNA COVID vaccines deliver the recipe for the spike protein … This causes immune cells to produce neutralizing antibodies against COVID, much as they would do if they had experienced a COVID infection.
With HIV, there’s no such simple recipe. HIV’s equivalent to the spike protein — its envelope glycoprotein — is wilier. It hides its vulnerable aspects, making it difficult for immune cells to generate antibodies against it. An even bigger problem is that HIV starts to mutate within hours of infecting someone …
HIV behaves like ‘a swarm of slightly different viruses’ … People with HIV rarely develop neutralizing antibodies, and in the very few who do, the antibodies take years to evolve — far too long for them to effectively fight the virus. The immune system can’t keep up.
But what if the immune system could be given a head start? That’s the idea behind the Moderna/IAVI vaccine … The researchers will administer a series of shots to try to coax the immune system along that years-long process ahead of time so that when it is exposed to HIV, it can spring into action.”
Hiding Injuries or Manufacturing Need for Vaccine, or Both?
So, to recap, the media’s focus on AIDS testing and the emergence of a more infectious strain of HIV may well be a coordinated effort to both:
a)Hide devastating COVID jab effects, and
b)Manufacture the perception that we have an urgent need for an HIV vaccine
If true, just think how sick that is. A widely-pushed mRNA injection for one pandemic causes a second pandemic that is worse than the first, allowing them to roll out a second mRNA “vaccine.” That second injection then erodes immune function even more, giving rise to a third epidemic and another injection. Where does it end? This plan has failure written all over it.
When I first learned of the mRNA COVID jab, it immediately struck me as a bad idea. There were several blatantly obvious mechanisms by which they might cause harm. Today, those concerns are borne out in injury and death statistics. The possibility for things to go wrong with an mRNA HIV vaccine is also assured, if you ask me. As reported by Bloomberg, the entire premise behind it is speculative.
The Moderna HIV vaccine will target a certain subset of B-cells known to loosely bind to HIV. The idea is that by prodding these B-cells with mRNA instructions, delivered through a series of shots, they might develop the capacity to produce neutralizing antibodies against HIV.
My fear here is that if the COVID shot can cause immune depletion after repeated doses, what kind of dysfunction might a series of HIV shots trigger? Endless COVID-19 booster shots are being presented as the solution to the pandemic, as repeated injections increase the level of antibodies in your body,18 but artificially inflated antibodies caused by repeated booster shots signal to your body that you’re always infected.
The resulting immune response may actually do more harm than good, and may accelerate the development of autoimmune conditions such as Parkinson’s, Kawasaki disease and multiple sclerosis, for example.19 Will an HIV vaccine based on a similar process be any safer? I doubt it.
The Fauci Connection
As noted by James Corbett in the video at the top of this article, there’s another interesting parallel between COVID and AIDS, namely Dr. Anthony Fauci himself. He was in charge of both of these epidemics, and without doubt — unless our justice system wakes up before then — he’ll be in charge of the coming AIDS campaign as well.
The parallels between Fauci’s AIDS campaign in the ‘80s and COVID are so strikingly similar, it’s almost like a handbook that’s being repeated, Corbett says. In the ‘80s, Fauci pushed the deadly drug AZT as the only permissible way to treat AIDS. During the COVID pandemic, Fauci’s failed and lethal Ebola drug remdesivir got the greenlight at the expense of far safer treatment alternatives.
Fauci is also a connecting link between the COVID shots and the HIV jab, as he’s been eagerly pushing for a transition from conventional vaccines to this new mRNA platform. As recently as October 2019, he participated in a panel discussion about how this transition might be achieved in light of regulatory hurdles and public distrust of gene transfer technologies.20
Fauci acknowledged it would indeed be very difficult to change people’s perception about vaccines (in this particular case he was referring to the flu vaccine). His advice? “Do it from within and say, ‘I don’t care what your perception is, we’re going to address the problem.’”
Not only does Fauci not care about public perception, he doesn’t care who he hurts either. He didn’t care about AIDS patients in the ‘80s, and he doesn’t care about COVID patients today. If he did, he’d insist on doctors using whatever works, and not just the products that he’s personally vested in.
HIV Discoverer Dies
An odd coincidence in the middle of all this is the unexpected death of Dr. Luc Montagnier, who together with Harald zur Hausen and Françoise Barré-Sinoussi in 2008 won the Nobel Prize for Physiology or Medicine for the discovery of the human immunodeficiency virus (HIV).21
Montagnier, who was 89 years old, died February 8, 2022, at the American Hospital of Paris in Neuilly-sur-Seine. No specifics about the cause of death have been released.22 Montagnier was an outspoken critic of the COVID jab from the start. He also suspected SARS-CoV-2 was genetically engineered, as the spike protein shared similarities with HIV.23
Is the AIDS Hype a Real Threat?
So, does the emerging AIDS hype reflect a real threat? Is it just an attempt to keep the population in fear? Or are they simply trying to cover up COVID jab effects? If it’s a cover-up, was HIV infection an accidental consequence or an intentional effect of the jab?
Might the new HIV variant actually be the result of mass COVID injection? After all, the timing of this “super strain” of HIV is interesting, to say the least. Why did it take 40 years for it to emerge?
Will HIV testing now be pushed the way COVID testing has been, and if so, why? As noted by Off-Guardian,24 for all we know, AIDS screening may simply be another way of monitoring this massive health experiment. For now, we have far more questions than answers, but if we keep asking them, eventually we’re bound to unearth the truth.
Business is booming at funeral homes across the U.S. as death rates creep up, particularly among young, working-age individuals
Ex-Blackrock fund manager Ed Dowd has been analyzing data about mortality rates before and after COVID-19 shots became widespread, and found that death rates worsened in 2021 — after the shots became prevalent — compared to 2020
Insurance companies are seeing increases in payouts for death and disability; Lincoln National stated death claims have increased 13.7% year over year and 54% in quarter 4 compared to 2019
Scott Davison, the CEO of insurance company OneAmerica, reported the death rate for 18- to 64-year-olds has risen 40% compared to before the pandemic
A study by Dr. Peter McCullough and colleagues suggests people who’ve received COVID-19 shots may have damage to their innate immune system that’s leading to a form of acquired immunodeficiency syndrome
Business is booming at funeral homes across the U.S., as death rates creep up, particularly among young, working-age individuals.1 Ex-Blackrock fund manager Ed Dowd has been analyzing data about mortality rates before and after COVID-19 shots became widespread, and found that death rates worsened in 2021 — after the shots became prevalent — compared to 2020.
As reported by Zero Hedge, Dowd pointed out “a spike in mortality among younger, working-age individuals coincided with vaccine mandates. The spike in younger deaths peaked in Q3 2021 when COVID deaths were extremely low (but rising into the end of September).”2
Dowd also reported data from public funeral home company Carriage Services, which announced a 28% increase in September 2021 compared to September 2020, while August had a 13% increase. He tweeted:3,4
“Business has been quite good since the introduction of the vaccines & the stock was up 106% in 2021. Curious no? Guys this is shocking as 89% of Funeral homes are private in US. We are seeing the tip of the iceberg.”
Life Insurance Payouts on the Rise
Insurance companies are also seeing increases in payouts for death and disability. Dowd tweeted February 1, 2022, that financial insurance company Unum reported a 9% increase in their benefit ratio (payouts versus premiums) in their life segment.5 Dowd tweeted:6
“In 2021 they saw a 17.4% increase vs 2020. This is higher than the 13.3% increase vs 2019. So the higher payouts in 21 are occurring with a miracle vaccine & less virulent strains … In 2019 the unit had $266 million profit, last year a profit of $82 million & this year a loss of -$192 million. A swing of $458 million lower over 2 years. Important to remember these are employed working age folks.”
Scott Davison, the CEO of Indiana-based insurance company OneAmerica, also reported disturbing statistics — the death rate for 18- to 64-year-olds has risen 40% compared to before the pandemic.7
“We are seeing, right now, the highest death rates we have seen in the history of this business – not just at OneAmerica,” Davison said, adding, “Just to give you an idea of how bad that is, a three-sigma or a one-in-200-year catastrophe would be 10% increase over pre-pandemic. So 40% is just unheard of.” Further, most of the deaths are not due to COVID-19. He said:8
“What the data is showing to us is that the deaths that are being reported as COVID deaths greatly understate the actual death losses among working-age people from the pandemic. It may not all be COVID on their death certificate, but deaths are up just huge, huge numbers.”
Disability Claims and Hospital Death Rates Rise
Disability claims, initially short-term claims and now long-term claims, have also seen an “uptick.” At a news conference where Davison spoke, Brian Tabor, president of the Indiana Hospital Association, confirmed that hospitals are also seeing widespread ill health and rising death rates. Zero Hedge reported:9
“Brian Tabor, the president of the Indiana Hospital Association, said that hospitals across the state are being flooded with patients ‘with many different conditions,’ saying ‘unfortunately, the average Hoosiers’ health has declined during the pandemic.’
In a follow-up call, he said he did not have a breakdown showing why so many people in the state are being hospitalized — for what conditions or ailments. But he said the extraordinarily high death rate quoted by Davison matched what hospitals in the state are seeing. ‘What it confirmed for me is it bore out what we’re seeing on the front end …’ he said.”
Other insurance companies citing higher mortality rates include Hartford Insurance Group, which announced mortality increased 32% from 2019 and 20% from 2020 prior to the shots. Lincoln National also stated death claims have increased 13.7% year over year and 54% in quarter 4 compared to 2019.10 Dowd tweeted:11
“Randy Frietag CFO just explained that in 2021 the share of young people dying from covid doubled in the back half of the year & that’s driven the result for Lincoln & its peers. He cited 40% in 3Q and 35% in 4Q were below the age of 65 … Mandates are killing folks … This shouldn’t be happening with miracle vaccines in a working age population period and a mild Omicron.”
As ZeroHedge noted, what we need to know from the insurance companies is what the leading causes of death were for 2020 and 2021, as well as how many received COVID-19 shots among those who died.
It continued, “Reinsurance Group of America, for example, reported a profit in Q4 2020 when the most of the population was unvaccinated and amid a deadlier strain of Covid-19, yet they registered a loss in Q4 2021 with more than 60% of the country fully vaccinated (and around 75% who have received at least one dose).”12
In other words, they paid out more in death and disability benefits in late 2021, after the shots became widespread, then they did at the peak of the pandemic, when no shots (or only a small number) had been issued.
Deaths Keep Rising Despite Mass Injection Campaign
Around the globe, it’s become clear that excess deaths continue to explode, despite the mass injection campaign that was supposed to save us. In the week ending November 12, 2021, the U.K. reported 2,047 more deaths than occurred during the same period between 2015 and 2019.
However, COVID-19 cannot be entirely to blame, as it was listed on the death certificates for only 1,197 people.13 Further, since July, non-COVID deaths in the U.K. have been higher than the weekly average in the five years prior to the pandemic.
Heart disease and strokes appear to be behind many of the excess deaths, with Financial Times reporting, “The new phase of excess deaths raises the possibility that since the summer more people have been losing their lives as a result of strains on the NHS or lack of early diagnosis of serious illness …”14
On Twitter, Silicon Valley software engineer Ben M. (@USMortality) similarly revealed that in a 13-week period alone, about 107,700 seniors died above the normal rate, despite a 98.7% vaccination rate.15 In another example, he used data from the U.S. Centers for Disease Control and Prevention, census.gov and his own calculations to show excess deaths rising in Vermont even as the majority of adults have been injected.
“Vermont had 71% of their entire population vaccinated by June 1, 2021,” he tweeted. “That’s 83% of their adult population, yet they are seeing the most excess deaths now since the pandemic!”16
An investigation by The Exposé, using official data from NHS and the U.K.’s Office for National Statistics (ONS), also found that deaths among teenagers increased 47% since they started getting COVID-19 shots.17 Not only that, but deaths from COVID-19 also went up among 15- to 19-year-olds after the shots were rolled out for this age group.
A study by board-certified internist and cardiologist, and editor of two medical journals, Dr. Peter McCullough and colleagues suggests people who’ve received COVID-19 shots may have damage to their innate immune system that’s leading to a form of acquired immunodeficiency syndrome.18
The mRNA COVID-19 shots use genetically modified mRNA encoding spike proteins. This results in mRNA being hidden from cellular defenses, “promote[s] a longer biological half-life for the proteins, and provoke[s] higher overall spike protein production,” the study suggests.19
The researchers state that experimental and observational evidence show that the human immune response to COVID-19 shots is very different than the response induced by exposure to SARS-CoV-2:20
“[T]he genetic modifications introduced by the vaccine are likely the source of these differential responses. In this paper, we present the evidence that vaccination, unlike natural infection, induces a profound impairment in type I interferon signaling, which has diverse adverse consequences to human health.
We explain the mechanism by which immune cells release into the circulation large quantities of exosomes containing spike protein along with critical microRNAs that induce a signaling response in recipient cells at distant sites.
We also identify potential profound disturbances in regulatory control of protein synthesis and cancer surveillance. These disturbances are shown to have a potentially direct causal link to neurodegenerative disease, myocarditis, immune thrombocytopenia, Bell’s palsy, liver disease, impaired adaptive immunity, increased tumorigenesis, and DNA damage.”
The study includes evidence from the Vaccine Adverse Event Reporting System (VAERS) to support its hypothesis. While health officials refuse to acknowledge that COVID-19 shots have caused deaths, clinically trained reviewers analyzed a sample of COVID-19 vaccine deaths reported in VAERS and found that only 14% of them were certainly not due to the vaccine.21
This means that the remaining 86% may have been related to the shots. Further, while it’s often stated that VAERS reports are made by laypeople, and therefore suggested to be unreliable, the review found that at least 67% of the COVID-19 vaccine death reports they analyzed were made by health service employees.22
Overall, McCullough and colleagues warn that COVID-19 shots subvert innate immunity, which could reduce the ability to combat future infections. Further, once damaged by the shots, the immune system may be less able to detect and prevent malignant transformation within cells.
They also suggest that exposure to spike protein-containing exosomes and mRNAs may induce an inflammatory cascade that further leads to disease. In concluding that COVID-19 shots are not positive contributors to public health, the study notes:23
“In the end, we are not exaggerating to say that billions of lives are at stake. We call on the public health institutions to demonstrate, with evidence, why the issues discussed in this paper are not relevant to public health, or to acknowledge that they are and to act accordingly.
Until our public health institutions do what is right in this regard, we encourage all individuals to make their own health care decisions with this information as a contributing factor in those decisions.”
Can You Lessen the Potential Damage?
Those considering COVID-19 shots must carefully weigh the evidence of risks before making a decision. But if you’ve already been injected and want to reduce your risk of any potential complications, there are a few basic strategies I recommend:
Measure your vitamin D level and take enough vitamin D orally (typically about 8,000 units/day for most adults) and/or get sensible sun exposure to make sure your level is 60 to 80 ng/ml (150 to 2000 nmol/l).
Eliminate all vegetable (seed) oils in your diet, which involves eliminating nearly all processed foods and most meals in restaurants unless you can be sure the chef is cooking only with butter. Avoid any sauces or salad dressings in restaurants, as they are loaded with seed oils. Also avoid chicken and pork, as they are rich in linoleic acid, the omega-6 fat that nearly everyone consumes far too much of and contributes to oxidative stress.
Consider taking around 500 milligrams a day of NAC, as it helps prevent blood clots and is a precursor for your body to produce the important antioxidant glutathione.
Consider taking fibrinolytic enzymes, which digest the fibrin that leads to blood clots, strokes and pulmonary embolisms. The dose is typically two, twice a day, but must be taken on an empty stomach, either an hour before or two hours after a meal. Otherwise, the enzymes will digest your food and not the fibrin in the blood clot.
U.K. football legend and sports commentator, Matt Le Tissier, has been speaking out about the large number of athletes who have collapsed or died on the field, and has lost his job as a result
Le Tissier says he has never seen anything like it in the 17 years he played football; he is calling for an investigation into the events and says ignoring it is a “massive dereliction of duty” by the officials
Fact-checkers and government officials are trying to negate or discredit information that supports the theory that mRNA injections are behind the sudden onslaught of injury and death, and they are studiously ignoring investigating the allegations
The Vaccine Adverse Events Reporting System (VAERS) reflects injuries to athletes in the general population, but it’s possible that the reports are nowhere near current
With every passing day, the list of people suffering tragic consequences from the COVID mRNA shots grows longer. Data1 show 23,149 people have died after a COVID jab as of January 28, 2022. There also are 13,575 reports of people with Bell’s palsy, 41,163 who are permanently disabled, 31,185 with myocarditis, 11,765 who have had heart attacks and 3,903 women who have lost their babies after getting the shots.
Many of these people and their stories have remained hidden from public view. YouTube, Instagram, Facebook and other social media platforms have censored the personal stories and videos of individuals documenting their injuries and permanent disabilities, so those who only read mainstream media are unaware of the overwhelming damage being done in the name of science.
However, there is a population of people whose injuries and death have been made public. In the past six months, a slew of professional and amateur athletes have collapsed and died on the field. Yet, mainstream media appear to take this in stride, acting as if what is happening is completely normal.
But, as described by Matt Le Tissier in the first seconds of the video above, this is far from normal. Le Tissier was a soccer legend2 (a sport called football in the U.K.). His prowess on the field earned him the nickname “Le God”3 before leaving the sport to become a sports commentator, most recently with Sky Sports.
As he describes in the interview, he lost that job for speaking out and bringing attention to the large number of unexplained sudden cardiac deaths happening to professional and amateur athletes around the world.
Athletes Are Dying on the Field in Large Numbers
Red Voice Media asks in a headline, “400 Athletes Collapsing & Dying Just in the Last 6 Months?”4 then mentions “small stories coming out about perfectly healthy athletes mysteriously dying.” During the interview, Le Tissier is asked about his thoughts on the surge of cardiac events in the sporting world, to which he responds:5
“I’ve never seen anything like it. I played for 17 years. I don’t think I saw one person in 17 years have to come off the football pitch with breathing difficulties, clutching their heart, heart problems …
The last year, it’s just been unbelievable how many people, not just footballers but sports people in general, tennis players, cricketers, basketball players, just how many are just keeling over. And at some point, surely you have to say this isn’t right, this needs to be investigated.”
Le Tissier acknowledges there may be other factors that have caused this massive rise in cardiac events in athletes. He mentions that the athletes may have had COVID, and this could be a consequence of the illness, or it could be the vaccine. But the point he makes is that it should be investigated and it’s not.
This may cause you to wonder why health experts are not placing blame on the infection, but are in fact ignoring the issue completely. It begs the question: Do they already know the answer?
Le Tissier goes on to talk about player safety and how the sport protects the players from playing too long or too many games, yet they are watching players collapse on the field and apparently are content acting as if this is normal. He calls it a “massive dereliction of duty” that no one in a position of power is calling for an investigation.6
“It’s absolutely disgusting that they can sit there and do nothing about the increase in the amount of sports people who are collapsing on the field of play. And it’s not just what I’ve noticed this season as well. Again, in my career, I don’t remember a single game being halted because of an emergency in the crowd, a medical emergency in the crowd …
I would like somebody to look into that and go well, hang on a minute, can we go back for the last 15 or 20 years and … have a look and see how many times it happened 10 years ago and then how many times it happened in the last year. I’ve been watching a lot of sports and a lot of reports on football, and I’ve never seen anything like it, the amount of games that have been interrupted because of emergencies in the crowd.”
The interviewer pointed out that correlation does not necessarily mean causation, to which Le Tissier agreed, but stressed that an investigation is required to find out if it does. “To my naked eye, this is happening a lot more than it has in the past. I can’t be the only one who is seeing this.”7
Who Are These Athletes?
While an overwhelming number of professional and amateur athletes have collapsed on the field, they are not just numbers. They all have a high probability of having one thing in common — they took the COVID shot. This four-minute video features a compilation of athletes who “suddenly” collapsed within a six-month period.
Kyle Warner is one of those athletes.8 He’s 29 years old and at the peak of his career as a professional mountain bike racer. After getting a second dose of Pfizer’s mRNA jab in June 2021, he suffered a reaction so severe that by October he was still spending many of his days in bed.
In an effort to get the word out that COVID-19 shots are not always as safe as you have been led to believe, Warner shared his experience with retired nurse educator John Campbell in November 2021. Warner, in his 20s and in peak physical condition, was still severely harmed by the shot.
“I believe where there is risk, there needs to be choice,” he says.9 But right now, people are being misled. “People are being coerced into making a decision based on lack of information versus being convinced of a decision based on total information transparency.”10
Warner’s story is not unlike many others’: As Campbell learned in this interview, many doctors are unwilling to acknowledge that the COVID-19 shots might be related to patients’ injury complaints. While health officials have begun to acknowledge that myocarditis may be related to the injections, they continue to ignore other adverse events.
Vaccine Injured Unlikely to Get Help
Fact-checkers are quick to negate the possibility that an overwhelming number of deaths and injuries in professional and amateur athletes is not related to the COVID shots,11 but embalmers are telling12 a different story.
Funeral director Richard Hirschman has been a professional, board-certified embalmer since 2004 and currently travels to several funeral homes to embalm bodies. He appeared on the “Dr. Jane Ruby” show to share some shocking findings he’s been seeing in his work the past few months.13
In mid-2021, he began noticing some individuals who died of heart attacks and strokes had strange clots in their veins and arteries. He showed images of fibrous-looking clots he’d pulled out of the patients’ bodies, some of which are the length of a person’s leg, and explained that normal clots usually fall apart when handled. These fibrous clots — which he said he’s seeing more and more of — maintain their integrity and can be manipulated without disintegrating.
Unfortunately, whether they die or not, when it comes to getting help for someone who believes they’re injured by the COVID shots, it’s unlikely that they get it without intensive efforts. One reason is because, while people are increasingly calling for support for the vaccine-injured, the only way to get recompense is through the obscure Countermeasures Injury Compensation Program (CICP).14
To give a little background, injury claims for regular vaccines go through the National Vaccine Injury Compensation Program (NVICP).
Initially set up as a “no-fault” system to resolve injury claims, this U.S. law ultimately protects drug companies with a complete liability shield, and if you win through this vaccine “court,” payouts come from a special fund set up just for that purpose, sparing vaccine makers, their insurance companies and vaccine providers from costly payouts for vaccine injuries and deaths.15
However, if you believe you’ve been injured by a COVID shot, and you want compensation for it, you have to go through a different vaccine “court” run by what Fortune describes as an “obscure office within the U.S. Health and Human Services Department.” And, this system not only protects manufacturers and health care providers from liability, but has hoops to jump through and limits to it that make compensation much more difficult than going through the NVICP.
The bottom line is, even if you can prove you were injured by a COVID shot, you can’t sue the drug company and the compensation you receive from the program is capped at $50,000 for lost wages and $370,376 for wrongful death.16
Officials Try to Discredit VAERS
The law that protects Big Pharma from regular vaccine injury claims is the 1986 National Childhood Vaccine Injury Act.17 The CICP claim process for COVID shots is conducted under the Public Readiness and Emergency Preparedness (PREP) Act, passed in 2005,18 which authorizes the government to take countermeasures against a public health emergency. The latest declaration under this Act was issued March 17, 2020, that provided:19
“… liability immunity to certain individuals and entities (Covered Persons) against any claim of loss caused by, arising out of, relating to, or resulting from the manufacture, distribution, administration, or use of medical countermeasures (Covered Countermeasures), except for claims involving “willful misconduct” as defined in the PREP Act.”
In other words, unless willful misconduct can be proven, any person covered by the act also has indemnity against claims from citizens. This is not limited to manufacturers and Big Pharma, but can also include government officials. The thing is, both claims systems are actually at the tail end of the process and don’t reflect all the possible injuries that might be occurring.
So how can you tell how many actual injuries may be occurring with a certain vaccine? That’s where another system kicks in: the National Vaccine Adverse Event Reporting System (VAERS).20 As I’ll explain later, anyone can make a report to VAERS, and it’s this key component that critics use to claim that VAERS can contain errors and even false claims.
While the system has a mechanism to help weed out false reports, top government officials, such as NIAID director Dr. Anthony Fauci and CDC director Dr. Rochelle Walensky, have attempted to discredit it. Most notably, this occurred during a Senate hearing when both individuals implied that if a person had been vaccinated and was then killed in a car accident, it’s possible it could be recorded in VAERS as a vaccine injury.21
It is important to note that the VAERS system is coadministered by the CDC and the FDA.22 However, as David Martin, whose self-described work involves ethical engagement and stewardship of community and commons-based value interests,23 points out in an interview excerpt posted on Twitter:24,25
“The fact is, that as much as the CDC and the FDA try to hide behind what they reportedly say is an error in the VAERS database, the Vaccine Adverse Event Reporting System, what they don’t seem to realize is that by saying that there are errors they are violating the 1986 Act …
If you go back and read that [the ACT] what you’ll find is that manufacturers of vaccines are required to keep VAERS accurate. That’s actually a statutory requirement. So, if they are telling you that it is not accurate, they are admitting to violating the law.”
By law, VAERS26 is a mandatory reporting system for health care professionals. The system is not set up to analyze causation, but may be used as raw data for detecting unexpected adverse events that may indicate a safety signal.
In total, the system must be maintained by health care professionals and drug manufacturers as a statutory requirement for maintaining indemnity against vaccine injury. Martin points out:27
“And that’s the quid pro quo in getting the immunity. If VAERS is wrong, then the immunity is pierced because it’s the manufacturer’s legal responsibility to make sure VAERS is accurate.”
VAERS Is Overwhelmed With Reports
Anyone can make a report to VAERS — both patients and health professionals can use this system to report health concerns they suspect may be connected to any vaccine, including the COVID shots. But since the system is passive, whether the reports get filed depends entirely on each individual living up to that responsibility.
The reports must contain all hospital records and any other relevant medical information. Unfortunately, as Brittany Galvin, a young woman who says she was injured by a COVID shot, succinctly notes in a video,28 the system is not efficient, and the data may be woefully out of date. This has a significant impact on monitoring the effects of the COVID inoculation program since it’s possible what you see on any given day in the VAERS database isn’t anywhere near current.
Galvin has created several videos talking about the journey she’s been on trying to report her adverse events to VAERS. In a video posted in January 2022,29 she recorded her phone conversation with an investigator from VAERS to discuss why her report filed in late May 2021 had not yet been counted in the system.
In one conversation she learned that the process takes many steps through different departments. The first stop for the VAERS reports is in a department with only 50 employees.30 Once the package of information is completed by this department, it is sent to a team of nurses who read and review every page.
If the staff have any concerns or if they feel they need more information, the package will be sent back to the first department for further information gathering.31 Galvin expressed her concern that there were hundreds of thousands of people like her and just 50 VAERS employees trying to process these reports.32
“Meanwhile the whole government is trying to force everyone to get this thing. Lying to the people telling them that “no one has gotten GBS from it” but here I sit barely able to walk and my case isn’t going to be ‘technically’ reported because the CDC hasn’t investigated yet because the hospitals are dragging their feet … it’s like a revolving crazy door and all of us humans on this planet and in this country are being lied to, and it’s unfair.”
At the end of the conversation with the investigator, Galvin learned that while her report was filed in May 2021, it wasn’t assigned to someone at VAERS until September or November 2021.33 It could be many months before the CDC receives the report of her vaccine injuries that can be published.34
“We found other coronaviruses in bats, a whole host of them, some of them looked very similar to SARS. So we sequenced the spike protein: the protein that attaches to cells. Then we… Well, I didn’t do this work, but my colleagues in China did the work. You create pseudo particles, you insert the spike proteins from those viruses, see if they bind to human cells. At each step of this, you move closer and closer to this virus could really become pathogenic in people. You end up with a small number of viruses that really do look like killers.”
This statement was said by EcoHealth Alliance President Peter Daszak at a 2016 forum discussing “emerging infectious diseases and the next pandemic”. Daszak, who received more than $118 million in grants and contracts from federal agencies, including $53 million from USAID, $42 million from DOD, and $15 million from HHS, appeared to boast about the manipulation of “killer” SARS-like coronaviruses carried out by his “colleagues in China” at the now infamous Wuhan Institute of Virology.
According to investigative research done by independent-journalist Sam Husseini and The Intercept, much of the money awarded to EcoHealth Alliance did not focus on health or ecology, but rather on biowarfare, bioterrorism, and other dangerous uses of deadly pathogens.
EcoHealth Alliance received the majority of its funding from the United States Agency for International Development (USAID), a State Department subsidiary that serves as a frequent cover for the Central Intelligence Agency (CIA). Their second largest source of funding was from the Defense Threat Reduction Agency (DTRA), which is a branch of the Department of Defense (DOD) which states it is tasked to “counter and deter weapons of mass destruction and improvised threat networks.”
The United States Agency for International Development (USAID) has a long history of acting as a contract vehicle for various CIA covert activities. With an annual budget of over $27 billion and operations in over 100 countries, one former USAID director, John Gilligan, once admitted it was “infiltrated from top to bottom with CIA people.” Gilligan explained that “the idea was to plant operatives in every kind of activity we had overseas; government, volunteer, religious, every kind.”
In 2013, a US cable published by WikiLeaks outlined the U.S. strategy to undermine Venezuela’s government through USAID by “penetrating Chavez’s political base”, “dividing Chavismo”, and “isolating Chavez internationally.” In 2014, the Associated Press disclosed that USAID contracted out a project to develop a rival to Twitter in order to foment a rebellion in Cuba.
From 2009 to 2019, USAID partnered with EcoHealth Alliance on their PREDICT program which identified over 1,200 new viruses, including over 160 coronavirus strains; trained roughly 5,000 people around the world to identify new diseases; and improved or developed 60 research laboratories.
What better way for the CIA to collect intelligence on the world’s biological warfare capabilities?
Dr. Andrew Huff received his Ph.D. in Environmental Health specializing in emerging diseases before becoming an Associate Vice President at EcoHealth Alliance, where he developed novel methods of bio-surveillance, data analytics, and visualization for disease detection.
On January 12, 2022, Dr. Andrew Huff issued a public statement (on Twitter) in which he claimed, Peter Daszak, the President of EcoHealth Alliance, told him that he was working for the CIA.
Dr. Huff continued, “…I wouldn’t be surprised if the CIA / IC community orchestrated the COVID coverup acting as an intermediary between Fauci, Collins, Daszak, Baric, and many others. At best, it was the biggest criminal conspiracy in US history by bureaucrats or political appointees.”
What exactly did they cover-up?
Peter Daszak’s EcoHealth Alliance—financed by USAID, DOD, and other U.S. Government agencies—partnered with Dr. Ralph Baric of the University of North Carolina and Dr. Shi Zhengli of the Wuhan Institute of Virology to conduct gain-of-function research on bat-borne coronaviruses.
Baric successfully created a “chimeric” coronavirus in 2015. There is a well-documented scientific paper trail that details how Dr. Baric and Dr. Zhengli continued to collaborate on gain-of-function research together to create what went on to be a potential precursor to the SARS-CoV-2 virus.
Dr. Anthony Fauci, Dr. Francis Collins, and Dr. Peter Daszak, who were proponents of this type of international collaboration on gain-of-function research were heavily incentivized to cover up the possibility of a lab origin because they previously had funneled U.S. taxpayer money to the Chinese lab.
At the start of 2020, there was a lot of chatter about where the virus SARS-CoV-2 actually originated from. Two papers published in March 2020—one in Nature Medicine and one in The Lancet—controlled the direction of the dialogue on the origin of the virus.
Both papers were repeatedly cited by Fauci, Collins, Daszak, the corporate media, and big tech as evidence to shut down and even censor any discussion of the possibility that the virus originated at the Wuhan Institute of Virology.
Only later through redacted emails released by FOIA did we learn that Fauci, Collins, and Daszak were intimately involved in crafting the two papers which dismissed the lab origin hypotheses as “conspiracy theory.”
In February 2020, Daszak told University of North Carolina coronavirus researcher Dr. Ralph Baric that they should not sign the statement condemning the lab-leak theory so that it seems more independent and credible. “You, me and him should not sign this statement, so it has some distance from us and therefore doesn’t work in a counterproductive way,” Daszak wrote.
More unredacted emails have revealed that while these scientists held the private belief that the lab release was the most likely scenario, they still worked to seed the natural origin narrative for the public through the papers published in Nature Medicine and The Lancet.
In April 2020, Daszak opposed the public release of Covid-19-related virus sequence data that has been gathered from China, as part of the U.S. Agency for International Development (USAID) PREDICT program because he said it would bring “very unwelcome attention” to the aforementioned “PREDICT and USAID” programs.
In September 2020, scientists were outraged when Daszak was chosen to lead the World Health Organization task force examining the possibility that Covid-19 leaked from the Wuhan Institute of Virology.
Despite many clear attempts to cut off a legitimate scientific inquiry into the Wuhan lab origin hypothesis, the theory continued to persist predominantly due to the fact that the Chinese government was unable to provide a single shred of evidence in support of the natural origin theory.
In May 2021, the narrative turned when, Nicholas Wade, a former science reporter at the New York Times published his seminal column outlining the case for the Covid lab-leak theory.
For SARS1, an intermediary host species was identified within four months of the epidemic’s outbreak and the host of MERS was identified within nine months. Yet some 15 months after the SARS2 outbreak began, and a presumably intensive search, Chinese researchers had failed to find either the original bat population, or the intermediate species to which SARS2 might have jumped, or any serological evidence of a natural origin.
Every step of the way, Fauci, Collins, and Daszak have done everything in their power to obfuscate, mislead, and misinform the world about the possibility of SARS-CoV-2 originating at the Wuhan Institute of Virology.
If Dr. Andrew Huff is telling the truth, Fauci, Collins, and Daszak are not covering up the lab origin only for themselves, but also for the Central Intelligence Agency, the Department of Defense, and the U.S. Government.
THE DOWNLOAD:
Dr. Robert Malone Publishes Photograph Of Uttar Pradesh Ivermectin Covid Kit: Densely populated, relatively poor, and they have absolutely crushed the COVID-19 death curve. Malone was able to acquire a photograph of a treatment kit that included; Paracetamol, Multivitamin W/ Zinc, Vitamin D3, Ivermectin, and Doxycycline. Read more.
Dr. Tyson And Dr. Fareed Publish #1 New Release In Communicable Diseases: Dr. Tyson and Dr. Fareed publish their new book, Overcoming The Covid Darkness: How Two Doctors Successfully Treated 7,000 Patients. The book tells the stories of how the doctors used early treatment protocols to successfully treat 7,000 (now 8,000) Covid-19 patients. Read more.
UChicago Must End Its Booster Mandate—We Are Not Lab Rats: The Editorial Board of The Chicago Thinker publishes an immaculately sourced scientific takedown of booster mandates for university students. We will not play pretend— COVID is not the plague, the vaccine is still experimental, and the risk of myocarditis and menstrual cycle issues is very real for young people. Read more.
Defeat The Mandates In D.C. On Sunday, January 23 Starting At 11:30 AM: Featured speakers include RFK, Jr., Dr. Peter McCullough, Dr. Robert Malone, Del Bigtree, Dr. Paul Marik, Dr. Richard Urso, Dr. Christina Parks, Dr. Bret Weinstein, Dr. Pierre Kory, Dr. Chris Martenson, Dr. Ryan Cole, Steve Kirsch, and more. Read more.
Thanks to the tyrannical actions of Chrystia Freeland — a Davos group devotee and the Deputy Prime Minister of Canada — the people of Canada are now rapidly withdrawing their funds from Canada’s largest banks. Two days ago, Freeland announced that Canada’s financial terrorism laws would be expanded to seize all funds — bank accounts, crypto, crowdfunding hubs, etc. — belonging to individuals who supported the peaceful convoy trucker protest… even if that person merely donated $10 to the convoy.
Around the U.S., COVID-19 patients are being killed by inappropriate medical protocols, and they have no say-so in the treatment they receive. They’ve literally been stripped of their patient rights
COVID patients are refused basic drugs like antibiotics and steroids. They’re even denied basic nutrition and fluids, which amounts to a war crime. Instead, COVID patients are over-treated with remdesivir, narcotics and mechanical ventilation, a combination that more often than not results in death
Hospitals are paid by the government for COVID tests, COVID diagnoses, admission of COVID patients, use of remdesivir and ventilation, and COVID deaths. This payment scheme has created a kind of institutionalized killing machine, where hospital revenue is tied to patients dying in-hospital with a COVID label, be it true or false
The Canadian press reports that COVID-19 patients are often given excessive doses of medications such as opioids, benzodiazepines and anticholinergics that could result in a lethal overdose, and in the U.K., senior care homes have been accused of killing off COVID patients with midazolam, a powerful sedative
Collectively, patient neglect, mistreatment, overtreatment and the COVID jabs have resulted in massive disability and death. Deaths among working age Americans (18 to 64) as of the third quarter of 2021 were 40% higher than prepandemic rates. Compare that to the 15.4% increase seen between 2019 and 2020, which was reported as the highest life insurance payout increase in 100 years
Something truly unthinkable is happening in America’s hospitals. Around the country, COVID-19 patients are being killed by inappropriate medical protocols, and they have no say-so in the treatment they receive. They’ve literally been stripped of their patient rights.
They’re refused basic drugs like antibiotics and steroids. They’re even denied basic nutrition and fluids, which amounts to a war crime under Rules 531 and 1182 of the Geneva Convention, which state you may not starve a person and you must provide basic necessities even to prisoners.
Instead, COVID patients are over-treated with dangerous and ineffective therapies like remdesivir, narcotics and mechanical ventilation, a combination that more often than not results in death. Many doctors who understand the importance of early and appropriate treatment are perplexed and horrified by what they’re seeing, and for good reason. It’s truly beyond comprehension at this point.
A Case of Medical Kidnapping for COVID Bounty?
Perhaps the most shocking example I’ve come across is the case of a perfectly healthy man involved in a car accident. In a talk with Stew Peters on Rumble, Benjamin Gord claims to have been given an unknown knock-out drug by the attending EMT and woke up on life support in a COVID ward.
He pulled out the vent all by himself, as he was unharmed from the accident. When he demanded to know why he’d been placed on mechanical ventilation, the shocked staff told him he was being treated for COVID.
In other cases, patients have been put on COVID standard care even though they came in for something else. Patients are also being denied release and are basically held as prisoners in the hospital. Many are refused the right to deny treatment.
On the other hand, they’re forced to accept do-not-resuscitate orders that they don’t want. There are also reports of COVID patients being given potent central nervous system respiratory depressants otherwise known as “euthanasia cocktails” — combinations of sedatives like morphine, fentanyl and midazolam.3
The medical kidnapping and mistreatment of patients against their will has become so widespread, human rights attorney Thomas Renz asked the Truth for Health Foundation to set up a medical advisory team, called the COVID Care Strategy Team, to help families physically liberate their loved ones from hospitals where they’re kept captive.4
Incentivizing the Killing of Patients
While one can speculate about the ethics of hospital administrators and doctors all day long, one of the most obvious answers to how this could have happened is that hospitals are receiving massive incentives to over-treat COVID patients to death. In the simplest terms, every patient has what amounts to a $100,000+ bounty on their head. Hospitals receive bonus payments for:5,6
• COVID testing and COVID diagnoses — Hospitals receive a 20% “bonus” on top of the standard cost for the treatment of a COVID patient7
• Admission of a “COVID patient”
• Use of remdesivir — The U.S. government actually pays hospitals an additional bonus when they use remdesivir,8,9,10 and that’s in addition to the 20% upcharge. Remdesivir was developed as an antiviral drug and tested during the Ebola breakout in 2014. Results were beyond disappointing. In the early months of 2020, the drug was entered into COVID trials.11
Those trials were also beyond disappointing.12,13,14 Not only was the drug ineffective against the infection but it also had significant and life-threatening side effects, including kidney failure and liver damage.15 Despite its clear dangers and lack of effectiveness, the U.S. Food and Drug Administration authorized remdesivir for emergency use against COVID in May 2020,16 and then gave it full approval in October 2020.17
• Use of mechanical ventilation, which CMS whistleblowers claim kill 84.9% of COVID patients within as few as 96 hours,18 typically due to barotrauma19 (trauma to the lungs from the elevated pressure).
• COVID deaths — In August 2020, former director of the U.S. Centers for Disease Control and Prevention, Robert Redfield, agreed hospitals had a financial incentive to overcount COVID deaths.20
According to Renz, hospitals are raking in a minimum of $100,000 extra for each and every “COVID patient” when they follow the directive to only treat with remdesivir and ventilation. On the other hand, hospitals that refuse to follow this deadly protocol and use things like ivermectin, antibiotics and steroids forfeit all government payments.
Still, financial incentives dictating drug treatment don’t explain why some hospitals are now withholding basic nutrition and fluids, quite literally torturing — starving — the patients to death. Such cases make it clear that death simply must be the desired outcome. Why else would you withhold food and water?
Initially, these COVID incentives were justified as a way to make sure hospitals would not be financially destroyed by the pandemic as they were losing revenue from routine care and elective surgeries they could no longer provide.21
Now, however, it seems this payment scheme has created a kind of institutionalized killing machine, where hospital revenue is tied to patients dying in-hospital with a COVID label, be it true or false.
Excessive Drugging of COVID Patients
Other countries are reporting similar trends. The Canadian press reports that COVID-19 patients are often given excessive doses of medications such as opioids, benzodiazepines and anticholinergics that could result in a lethal overdose.22
In the U.K., senior care homes have been accused of killing off COVID patients with midazolam, a powerful sedative. In April 2020, 38,352 out-of-hospital prescriptions for midazolam were issued, while the monthly average for the five years before was only 15,000, which is explained in detail in the above video.
“Midazolam depresses respiration and it hastens death. It changes end-of-life care into euthanasia,” retired neurologist Dr. Patrick Pullicino told MailOnline.23
And speaking of euthanasia, at the end of 2021, the government of New Zealand OK’d “voluntary euthanasia” by lethal injection for COVID patients if the doctor believes the COVID patient won’t recover.24 The doctor performing the euthanasia gets paid $1,087 by the government for this service.25
Deadly Prevention
Everywhere you look, the focus seems to be on maximizing the death toll, not saving lives. That includes the COVID jabs, which are touted as the only way to prevent serious infection and death. Yet data from the U.S. Department of Defense suggest the jabs are causing unprecedented injuries and deaths. The Defense Medical Epidemiology Database (DMED) data were obtained by Renz from DOD whistleblowers, and was released on the Renz Law website.26
The data show that, compared to the previous five-year averages, miscarriages were up 279% among DOD personnel in 2021, breast cancer went up 487%, nervous system disorders 1,048%, male infertility 350%, female infertility 471%, ovarian dysfunction 437% and on and on. As noted by Renz during U.S. Sen. Ron Johnson’s “COVID-19: A Second Opinion” panel:27
“The Whistleblower data, this DMED database, has provided a control group of sorts. It’s military records dating back several years that supply medical codes for various medical issues that our military face such as cancers, miscarriages, neurological disorders etc.
These records provided by three military doctors … show a historical baseline of what the health of the American military was like before 2021, the year the COVID vaccine was released. What you see is quite disturbing.
From 2016 to 2020 all variations of medical conditions stay consistent. But in 2021, when the variable of the vaccine is mandated, the spike in cancers, miscarriages, infertility, you name it, jumps by factors of hundreds to thousands of percent.
Let me be crystal clear. These vaccines are injuring and sometimes even killing our military, and those in the public that are buying the ‘safe and effective’ marketing. These numbers prove it beyond a shadow of a doubt.”
Pentagon’s Response — An Even Bigger Story
In response to the leaked DMED data, the Pentagon is now claiming that “a glitch” in the database resulted in incomplete data sets being shown for the five years Renz is using as a baseline. The real medical diagnoses for 2016 through 2020 are far higher, they claim, and that made the 2021 numbers appear falsely elevated.
According to Maj. Charlie Dietz, a task force public affairs officer for the DOD, the DMED was taken offline “to identify and correct the root cause of the data corruption.” Once the supposed “missing” medical diagnoses were added back in, the reported number of diseases and injuries for 2021 were 3% LOWER than 2020, and the lowest it’s been in six years. As reported by The Blaze:28
“Where those true numbers existed, why they weren’t in the system for five years, what exactly was in the system, and why the 2021 numbers were accurate according to the DOD account remain a mystery.
However, one by one, the military public health officials have been adding back random numbers to the 2016 through 2020 codes. I’m told by Renz and two of the whistleblowers that throughout the past week, they have queried the same data again, and in most of the ICD categories, they have found that the numbers from 2016 through 2020 were ‘increased’ exponentially to look as though 2021 was not an abnormal year.
This has been done without any transparency, any press release, any statement of narrative, and sloppily in a way that makes the already unbelievable narrative simply impossible to believe.
In addition to believing that every epidemiological report for five years was somehow completely tainted with false data … we would have to believe that the minute they discovered this from Renz, they suddenly discovered the exact numbers. A five-year mistake fixed overnight!”
Incompetence, Corruption, Both — or Worse?
Making this clown show even more indefensible is that the Centers for Disease Control and Prevention’s Advisory Committee on Immunization Practices (ACIP) has admitted that they’ve been monitoring the DMED data from the start.29
Either way you slice it, we have a serious problem. If the DoD just now discovered corrupted data in the DMED, then there’s incompetence in its ranks. And if ACIP was looking at the DMED data and kept pushing for vaccination despite alarming safety signals, then ACIP is incompetent — or worse.
If there’s nothing wrong with the database and the numbers Renz initially obtained were accurate, then people within the DOD are falsifying data to cover up COVID jab injuries and sacrificing our military to protect Big Pharma profits — an action that, if true, seems dangerously close to treason.
As noted by Steve Kirsch,30 founder of the COVID-19 Early Treatment Fund, the DOD’s “explanation” for the discrepancy in its 2021 injury statistics is just riddled with holes. First of all, they’ve not explained why 2016 through 2020 data were affected, yet 2021 was not.
Secondly, they’ve not explained how they were able to correct “underreporting” of health problems in 2016 through 2020. How did they know there was underreporting? And why didn’t they fix it earlier? Thirdly, and perhaps most importantly:
“Only symptoms that were elevated by the vaccine were affected; that’s impossible for a computer glitch to have caused that … That makes their ‘corruption’ explanation hard to explain. Very hard to explain.”
Pfizer Warns Investors of Possible Business Impacts
Meanwhile, Pfizer appears poised for the emergence of bad news. In its fourth quarter earnings release and risk disclosure,31,32 the company admits that “the possibility of unfavorable new preclinical, clinical or safety data and further analyses of existing preclinical, clinical or safety data or further information regarding the quality of preclinical, clinical or safety data, including by audit or inspection” could impact earnings.
They also note challenges related to public confidence, concerns about clinical data integrity, and prescriber and pharmacy education as potential risks, and that’s in addition to the possibility that COVID-19 might “diminish in severity or prevalence, or disappear entirely.”
All-Cause Deaths Soared in 2021
Collectively, patient neglect, mistreatment, overtreatment and the COVID jabs have resulted in massive disability and death. In early January 2022, OneAmerica, a national mutual life insurance company based in Indianapolis, reported deaths among working-age Americans (18 to 64) as of the third quarter of 2021 were 40% higher than prepandemic rates — and they’re not dying from COVID.
Compare that to the 15.4% increase seen between 2019 and 2020. In December 2021, Fortune magazine reported this as the highest life insurance payout increase in 100 years.33 Well, they ain’t seen nothing yet, as the saying goes. OneAmerica CEO Scott Davidson said:34
“We are seeing, right now, the highest death rates we have seen in the history of this business — not just at OneAmerica. The data is consistent across every player in that business.
And what we saw just in third quarter, we’re seeing it continue into fourth quarter, is that death rates are up 40% over what they were pre-pandemic. Just to give you an idea of how bad that is, a three-sigma or a one-in-200-year catastrophe would be 10% increase over pre-pandemic. So, 40% is just unheard of.”
At the same time, OneAmerica has also noticed an uptick in disability claims. Initially, there was a rise in short-term disability claims, but now most claims are for long-term disabilities. The company expects the rise in claims will cost them “well over $100 million,” an unexpected expense that will be passed on to employers buying group life insurance policies.
Globally, the life insurance industry was hit with claims amounting to $5.5 billion in the first nine months of 2021, which is when the COVID jabs were most aggressively rolled out. During all of 2020, the height of the pandemic, claims only reached $3.5 billion.35 According to one insurance broker cited by Reuters, the industry was caught off-guard, as they expected the mass vaccination campaign to result in lower payouts in 2021. Reuters also reports that:36
The Dutch insurer Aegon, which does two-thirds of its business in the U.S., saw U.S. claims rise from $31 million in 2020, to $111 million 2021
U.S. insurers MetLife and Prudential Financial also reported an increase in claims for 2021 compared to 2020 and prepandemic years
Reinsurer Munich Re raised its 2021 estimate of COVID-19 life and health claims from 400 million euros to 600 million euros
Treat COVID Symptoms Immediately and Aggressively
We live in heartbreaking times —so much unnecessary pain, suffering and death. The fact that so many of these atrocities are occurring in our hospitals make the situation all the more disconcerting. This, truly, is not the time to go to the hospital unless your life depends on it.
That’s the last place you want to be right now, for any reason. It’s beyond tragic, but you simply cannot count on hospitals to give unconflicted care like you could in the past, and that could lead to your premature demise.
Your best alternative is to be prepared. Create a “COVID survival kit,” much like you would a tornado or hurricane kit, so you can spring into action and treat yourself immediately at first symptoms. Perhaps it’s the common cold or regular influenza; maybe it’s the much milder Omicron, but since it’s hard to tell them apart, your best bet is to treat all cold/flu symptoms as you would treat earlier forms of COVID.
And, remember, this advice applies for those who have gotten the jab as well, since you’re just as likely to get infected — and perhaps even more so. Early treatment protocols with demonstrated effectiveness include:
A former Blackrock portfolio manager, Edward Dowd, has come forward to explain what’s really going on behind the pandemic shutdowns and mandates — and it’s all about money and a pending global collapse of the financial industry.
“We have a global debt problem,” Dowd says. “And it’s been since 2008 kind of a clarion call … they know you can’t keep it afloat forever.” With that in mind, he says when he saw the “COVID thing go down,” he immediately was suspicious that what was happening wasn’t about COVID at all.
“It was a perfect cover for central banks to print money for an emergency … and put in place medical tyranny systems as cover for a collapse of the financial system to prevent riots … All the pensions are broke, he says — and “it’s just a system of control.” Where Pfizer is concerned, he became suspicious when he was looking at clinical trial reports and FOIA-requested documents.
What he saw was that in the vaccine clinical trial groups, there were more deaths than in the placebo group. He also noticed that biotech industry executives who saw that were suddenly refusing the boosters and those who hadn’t yet been vaccinated were deciding not to get the shots.
Biophysics researcher Dr. Andreas Kalcker discussed the blood clotting that many vaccinees experience and how CDS helps degrade the micro clots responsible for this condition.
A testimony that has impacted Dr. Kalcker is that of Manu, a tattoo artist who has been tattooing people for 25 years and who claims that when he performs his art on people’s skin they no longer bleed. Dr. Kalcker pointed out that this is a sign of coagulation that can be solved thanks to chlorine dioxide.
Dr. Andreas Kalcker: I’m very happy because, right now, the question that a lot of people are asking is “What’s going on?” So, the things is… So, the thing is, of course, they’re saying, “What’s going on with me now?” Because of course, a lot of people —most people, in fact—, have been inoculated. And then, they’ve been told one thing and then another. Because, of course, they’re told that it’s a vaccine and, really, what they’ve really received is a genetic experiment. And those who have become aware of it are tired, without strength and defenses. In other words, people catch colds very easily and from anything.
And, of course, there’s a very obvious truth. It’s much easier to deceive than to wait for the deceived to realize the trap. And of course, people ask, “What now?” “What am I going to do? I’m already (inoculated).”
So, the fantastic thing that we have, and we already have a certainty, is that dioxide also works for precisely what we’re seeing. Because what we’re seeing is coagulation in the blood. What’s coagulation? It’s very simple. For example, you get bitten by a snake. And then you take, for example, a blood test, and you add the snake venom factor, the blood coagulates. So this is a well-known thing. There are many references. Many. And then, of course, blood coagulation is a factor that, from conventional medicine, what will be done? Well, prescribe an anticoagulant, such as warfarin, which is a substance equal to rat poison. And which, in the long term, will cause strokes, etc. It’s not a solution at all. However, chlorine dioxide is a solution because we have seen that it directly dissolves these mini clots before they get bigger. And this is what people are seeing all over the world.
Yesterday, I received a message from a tattoo artist telling me, “Andreas, I have been tattooing for 25 years, and something strange is going on.” And I asked him, “Well, what’s going on?” “Normally, when I’m tattooing, little drops of blood come out, but now, not anymore.” “Not anymore.” “The skin doesn’t react. It’s a very strange thing that I’m seeing.” And that’s, obviously, one of the first signs of micro-coagulation. That’s how it starts. Then, it gradually gets worse.
And then, well, people who are already taking the dioxide from the beginning, in this way, it dissolves these micro-clots because we have seen it under a microscope. And of course, people can see it on my website and other places, as well. It really is capable of doing this. So what are the COMUSAV doctors saying quite correctly? You have to take it. You have to take it for three to six months. Or longer in severe cases. And it’s okay because, really, even if you take it for a year or 15, like me, you’re not going to die. You’re not going to have serious side effects either.
So, it’s taking protocol C if I don’t know anything. And with this, I’m already getting rid of these clots. And if I can, if I’m more advanced in this, I can also do the AI (Anti Inoculation) protocol that’s on COMUSAV’s website. This is a fact, and we have a solution. That is, people many times, and on many, many websites, are complaining, complaining, complaining. And whether it’s this or that. Complaining isn’t a solution. Nobody gets cured. So we must know and let all the people around the world know that there’s a solution. And that solution exists, and it isn’t toxic. And it’s being taken by millions of people at this point.
Injected microtechnology stops working if graphene is removed from the body
Dr. Martín Monteverde reported for OMV (World Organization for Life) that although there isn’t yet a known way to remove the injected microcircuitry from the body, removal of the graphene oxide causes it to stop working.
Baicalin and baicalein are flavones under investigation for potential benefits to the nervous system & in rheumatoid arthritis. Learn more here.
What are Baicalin and Baicalein?
Baicalein is a flavone, a type of polyphenolic flavonoid, that is extracted from the roots of Scutellaria baicalensis and Scutellaria lateriflora that have a wide variety of health benefits.
Baicalin is a flavone glycoside, the glucuronide of baicalein, which is obtained through the binding of glucuronic acid to baicalein. It is primarily used in Asian countries as an herbal supplement.
Potential Health Benefits
Baicalin and baicalein supplements have not been approved by the FDA for medical use and generally, lack solid clinical research. Regulations set manufacturing standards for them but don’t guarantee that they’re safe or effective. Speak with your doctor before supplementing.
Possibly Effective For
1) Rheumatoid Arthritis & CAD
In one study of 374 patients with rheumatoid arthritis and coronary artery disease (which are frequently comorbid), 500 mg of baicalin per day significantly reduced blood lipids and markers of inflammation [1].
Animal Research (Lacking Evidence)
No clinical evidence supports the use of baicalin for any of the conditions listed in this section. Below is a summary of the existing animal and cell-based research, which should guide further investigational efforts. However, the studies listed below should not be interpreted as supportive of any health benefit.
2) Anxiety
Baicalein and baicalin inhibited the action potential of the neurons that raise anxiety [2].
In mice, baicalin produced anxiety-lowering effects without causing drowsiness or muscle relaxation [3].
3) Neuroprotection
Baicalin improved cognitive dysfunction in mice via its anti-neuroinflammatory activity, leading authors to suggest it as a potential candidate for the treatment of Alzheimer’s Disease (AD) [4].
It improved Amyloid beta-induced learning and memory deficit, hippocampus injury and neuron apoptosis (mice) [5].
Baicalin improved learning and memory impairment induced by brain injury in mammals [6].
Treatment with this flavonoid in animals, post-stroke, promoted neuron development in damaged sections of the brain, including the new formation of cells in the hippocampus [7].
4) Liver
Baicalin administered in rats reduced the effects of fatty liver disease (by increasing PPAR gamma and insulin receptors) [8].
It decreased cholesterol, alanine transaminase, low-density lipoproteins, and TNF levels.
Rats with alcohol-induced liver damage treated with this flavonoid before consuming alcohol had protective effects on the liver. It also decreased liver cell apoptosis [9].
5) Lung Function
Pure baicalin improved lung function in rats suffering from allergic diseases [10].
When administered to rats suffering from asthma as a pretreatment, baicalin stimulated a healthy remodeling of the airway [11].
Baicalein reduced lung inflammation by inhibiting Th17 cells in the lungs [12].
6) Eyes
Daily intake of baicalin or baicalein helped prevent eye diseases such as cataracts or age-related macular degeneration in animals [13].
Baicalin is found in traditional Japanese herbal medicines for eye health [14].
7) Fertility
In animals, baicalin significantly enhanced endometrial reproduction [15].
In mouse embryos, it increased the development and quality of blastocysts [16].
Cancer Research
Baicalin and baicalein are currently under investigation in the following types of cancers:
These experiments are currently limited to cell studies, however; such studies are often irrelevant for animal or human trials.
Baicalin ingested at a dose of 100 mg/kg for 28 days decreases tumor growth and replication in mice with colon cancer cells [21].
When taken orally in rats for 7 days it increases the activity of T helper cells and T regulatory cells to fight chemically-induced colon cancer [22].
Limitations
There are a variety of limitations that should be kept in mind when reading this research.
Almost all of the studies conducted with baicalin are in animals, and it’s not clear if any of these benefits would occur in humans.
Flavonoids usually have poor bioavailability, and baicalin is no exception [23]. It’s unclear if any of these benefits would be seen in humans given the bioavailability issues. When given to animals, it’s often injected, which bypasses the bioavailability problem that humans would have.
Dosage
There is no safe and effective dose of baicalin or baicalein because no sufficiently powered study has been conducted to find one.
Baicalein and baicalin supplements can be taken by healthy individuals. The healthy dose should be 200-800 mg in multiple doses, once in the morning and once again at night, without any side effects.
Between 2000 and 2016, the annual death toll from liver cancer in the U.S. rose by 43% for men and 40% for women. Globally, hepatocellular carcinoma is the third leading cause of cancer death
Other liver-related diseases such as cirrhosis and nonalcoholic fatty liver disease (NAFLD) are also becoming more prevalent, both of which raise your risk of liver cancer
Between 2001 and 2013, diagnosed cirrhosis cases nearly doubled; deaths from cirrhosis increased by 65% between 1999 and 2016. The greatest increase was among those between the ages of 25 and 34, where alcoholic cirrhosis has become rampant
Alcohol-induced cirrhosis and NAFLD can be reversed in their early stages by quitting drinking and cutting out processed fructose, respectively
Folate, milk thistle, NAC, coffee and broccoli all help promote healthy liver function
This article was previously published August 1, 2018, and has been updated with new information.
According to the American Cancer Society (ACS),1 liver cancer affects an estimated 41,260 Americans each year, and prevalence is rising.2 Between 2000 and 2016, the annual death toll from liver cancer rose by 43% for men and 40% for women,3 killing more than 11,000 people in 2016.4
In January 2022, the ACS estimates that 30,520 people will die from liver cancer in this year alone, adding, “Liver cancer incidence rates have more than tripled since 1980, while the death rates have more than doubled during this time.”
The five-year survival rate for localized liver cancer is 34 percent,5 while regional cancer that has spread to other organs and distant liver cancer have survival rates of just 12 percent and 3 percent respectively.
Globally, the liver cancer hepatocellular carcinoma (HCC) is the third leading cause of cancer death6 due to the high prevalence and difficulty of treatment. Researchers warn that by 2030, the global rate of liver cancer will double, affecting upward of 1.2 million.7
Other liver-related diseases such as cirrhosis, nonalcoholic fatty liver disease (NAFLD) and nonalcoholic steatohepatitis (NASH)8 are also becoming more prevalent. Between 2001 and 2013, the number of diagnosed cirrhosis cases nearly doubled,9 and deaths from cirrhosis increased by 65 percent between 1999 and 2016.10 The greatest increase (10.5 percent) was among those between the ages of 25 and 34, where alcoholic cirrhosis has become rampant.11,12
As a precursor for cancer, cirrhosis causes more than 1 million deaths a year worldwide,13 with the incidence of NASH more than doubling from 1990 to 2017.
Excess Alcohol Consumption Drives Risk of Liver Damage
According to researchers, the rise in cirrhosis mortality is entirely driven by excess alcohol consumption by young adults. While, historically, alcohol-related liver cirrhosis has been regarded as a condition that develops after two or three decades of heavy drinking, these newer statistics reveal it doesn’t have to take that long at all, as it’s now occurring in (and killing) 20- and 30-year-olds.
In the 25 to 34 age group, death from alcohol-related liver disease nearly tripled between 1999 and 2016. This increase parallels statistics14 showing a rise in binge drinking between 2002 and 2012. It also correlates with the global financial crisis in 2008, after which more people began dying from cirrhosis. Researchers believe financial worries and unemployment may be significant contributing factors, causing more people to drink more heavily.
Cirrhosis (irreversible scarring of your liver) can also be caused by obesity, NAFLD and hepatitis, and can in turn lead to fatal liver failure and/or liver cancer. Men are particularly at risk, in large part because they’re five times more likely to develop NAFLD than women.
Lifestyle factors such as diet, exercise, weight, smoking and alcohol consumption also play important roles in exacerbating (as well as reducing) your chances of developing some form of liver disease.
People at increased risk also include those who have an autoimmune disease, chronic liver inflammation and those whose livers have been damaged due to bouts of hepatitis B or C. The good news is that alcohol-related liver cirrhosis can be reversed if caught early enough — and provided you quit drinking.
While alcohol-related cirrhosis is driving up mortality rates, rising prevalence of NAFLD is contributing to the overall burden of liver-related diseases. In the case of NAFLD, the fatty liver occurs in the absence of significant alcohol consumption, and is driven instead by excess sugar, which is why this condition is now found even in young children.
NAFLD often has no symptoms, although it may cause fatigue, jaundice, swelling in the legs and abdomen, mental confusion and more. If left untreated, it can cause your liver to swell, called nonalcoholic steatohepatitis (NASH), and can lead to liver cancer or liver failure. As with alcohol-related cirrhosis, however, NAFLD can be reversed in its early stages by healthy eating and exercising.
Most importantly, you need to eliminate processed fructose and other added sugars from your diet. Fructose actually affects your liver in ways that are very similar to alcohol. Unlike glucose, which can be used by virtually every cell in your body, fructose can only be metabolized by your liver, as your liver is the only organ that has the transporter for it.
Since all fructose gets shuttled to your liver, if you consume high amounts of it, fructose ends up taxing and damaging your liver in the same way alcohol and other toxins do. The way your liver metabolizes fructose is also very similar to that of alcohol,15 as both serve as substrates for converting carbohydrates into fat, which promotes insulin resistance, dyslipidemia (abnormal fat levels in the bloodstream) and fatty liver.
Fructose also undergoes the Maillard reaction with proteins, leading to the formation of superoxide free radicals that can result in liver inflammation similar to acetaldehyde, an intermediary metabolite of ethanol. According to Dr. Robert Lustig, a neuroendocrinologist in the division of endocrinology at the University of California, fructose is a “chronic, dose-dependent liver toxin.”
Excess Glucose Converts to Fructose and Decimates Your NAD+
A few years ago I read an excellent review16 on NAD that helped me understand the basic biochemistry far better, and it makes perfect sense. I learned that excess fructose in processed foods isn’t the only problem, as excess glucose is ultimately converted to fructose by your body in an effort to metabolize glucose for energy. Let me explain it to you.
When your body is exposed to chronic glucose excess, the first enzyme in breaking down glucose is hexokinase, and this enzyme becomes saturated and can’t break down any more glucose. Once this occurs, glucose will then be metabolized through the polyol pathway, in which glucose is metabolized to sorbitol by aldose reductase, and sorbitol is subsequently metabolized to fructose by sorbitol dehydrogenase (see figure below).
It is estimated when you are healthy, only about 3% of glucose goes through the pathway below, but at least 30 percent of glucose flows through this pathway in chronic hyperglycemia,17 creating a vicious cycle of excess fructose.
This metabolic catastrophe is the net redox result of the trading of one molecule of NADPH for one molecule of NADH. This is precisely what you don’t want to happen, as NADPH is used as a reductive reservoir for your antioxidants and is necessary to make your steroid hormones and fats. When you have low levels you are in deep trouble.
Complicating it further, you increase NADH and worsen your NAD+/NADH ratio. As fuel supply outstrips metabolic demand, mitochondrial and cytoplasmic NAD/NADH ratios fall. The ensuing mitochondrial membrane hyperpolarization perpetuates electron leakage and excessive oxidative stress.
Fortunately, the good news is that there is a simple inexpensive solution that should radically improve this metabolic catastrophe. The first, of course, is to clean up your diet as we have previously discussed many times, so your body can burn fat for fuel. But you can also take NAD precursors like simple nontimed-release niacin.
That should help increase the NAD+/NADH ratio and NADPH levels. As noted in one recent paper,18 “Oral administration of nicotinamide riboside, a natural NAD+ precursor, completely corrected these NAFLD phenotypes induced by NAD+ deficiency.”
I would start non-timed release niacin at 25 to 50 milligrams a few times a day, as any dose higher will likely cause a harmless but relatively annoying flushing sensation. It would also be helpful to reduce your exposure to electromagnetic fields, as that also consumes NAD+ through PARP hyperactivation and will worsen the metabolic condition.
Low-Level Chemical Exposures Linked to Liver Damage
While there’s no data on this, it’s possible that alcohol-induced cirrhosis is now occurring sooner as a result of liver damage caused by chemical exposures. Researchers have shown that even small amounts of chemicals from food, pharmaceuticals and personal care products can in fact cause liver damage.
One such experiment19 was designed to evaluate the effects of chemical combinations at low doses from environmental sources such as food, pharmaceuticals and personal care products.20
Using four groups of Sprague-Dawley rats, the researchers administered a mix of chemicals found in everyday products in their drinking water at varying doses for a period of six months. The control group received chemical-free water.
Of the three treatment groups, the low-dose group received 25% of the European Union (EU) acceptable daily intake for the chemicals in question, the medium-dose group received exactly the acceptable daily intake defined by the EU, while the high-dose group received five times the acceptable daily intake.21
After six months, body weight and biochemistry markers were evaluated, revealing the animals’ weight increased more than 10% in all male groups, compared to controls.22 Modest increases were found in females given medium and high doses of the chemicals.
They also discovered adverse liver effects — especially at the low-dose level and primarily in the males. Overall, the results suggest exposure to low doses may induce liver damage as a result of the combination of different toxic mechanisms, and support previous research showing that chemical cocktails, even at low levels,23 can damage liver function24 and trigger cancer.25
Roundup Damages Liver at Ultralow Doses
Roundup, the most heavily-used weed killer in the world, has also been linked to liver damage. Disturbingly, urine levels of glyphosate have skyrocketed in the past couple of decades, suggesting widespread, chronic exposure, most likely from food. Between 1993 and 2016, levels of the chemical in human urine increased 1,200 percent.26 Food testing also reveals that many foods sold in the U.S. are contaminated with glyphosate.27
This is of significant concern, as research suggests Roundup can cause significant liver damage even at ultralow doses. The study,28 published in the journal Scientific Reports, looked at the effects of glyphosate exposures of 4 nanograms per kilogram of body weight per day, which is 75,000 and 437,500 times below EU and U.S. permitted levels, respectively.
After a two-year period, female rats showed signs of liver damage, specifically NAFLD and progression to nonalcoholic steatohepatosis (NASH). Study author Michael Antoniou, Ph.D., told Sustainable Pulse:29
“The findings of our study are very worrying as they demonstrate for the first time a causative link between an environmentally relevant level of Roundup consumption over the long-term and a serious disease — namely nonalcoholic fatty liver disease. Our results also suggest that regulators should reconsider the safety evaluation of glyphosate-based herbicides.”
Milk Thistle Helps Prevent Liver Damage
Milk thistle is an herb that has been used for thousands of years to support liver, kidney and gallbladder health. In modern times, silymarin has been used to treat alcoholic liver disease, acute and chronic viral hepatitis and toxin-induced liver diseases.
The active ingredient, a flavonoid called silymarin, is thought to be responsible for the beneficial effects attributed to milk thistle, including liver protection, antioxidant, antiviral and anti-inflammatory properties. In your liver, silymarin works as an antifibrotic, thereby preventing tissue scarring, and blocks toxins by inhibiting the binding of toxins to liver cell membrane receptors. Silymarin also protects your liver and promotes healthy liver function by:
Suppressing cellular inflammation30
Inhibiting the mammalian target of rapamycin (mTOR), a pathway that, when overactivated, increases your risk of cancer31
Activating AMPK (activated AMP-activated protein kinase),32 an enzyme inside your cells. AMPK is sometimes referred to as a “metabolic master switch,” as it plays an important role in regulating metabolism and energy homeostasis.33 AMPK produces many of the same benefits as you would get from exercise and weight loss, both of which benefit your liver health
Reducing liver injury caused by a number of drugs and environmental toxins, including acetaminophen, chemotherapy, psychotropic drugs and alcohol
Increasing glutathione, a powerful antioxidant that plays a role in the detoxification of heavy metals and other harmful substances
N-acetylcysteine Supplement Supports Your Liver Health
Another powerful liver protectant is N-acetylcysteine (NAC), a precursor needed for glutathione biosynthesis. In fact, research suggests NAC may be a better alternative for supporting liver health in those with hepatitis C and other chronic liver diseases than the antioxidant resveratrol.34
Alcohol and acetaminophen are two common compounds metabolized through the liver that are associated with liver damage. NAC supplementation has been effective in minimizing damage associated with alcohol consumption when taken prior to alcohol ingestion.35
NAC is also used as an antidote for acetaminophen toxicity, which causes liver damage by depleting glutathione.36 Research published in Hepatitis Monthly37 has also shown NAC supplementation helps improve liver function in patients with NASH.
Folate Deficiency Worsens Severity of NASH
Increasing your intake of folate can also help protect your liver function. In a study38 involving 83 patients with NASH, researchers found levels of folate and vitamin B12 were inversely related to the development of fibrosis or the formation of scar tissue. Past research has identified an association between low levels of vitamins and chronic liver disease, but this is the first to find an association between folate and vitamin B12 level to NASH severity.
Studies have also shown folate deficiency can increase your risk for liver cancer.39,40 In one, which involved hepatitis B-positive patients (who are at higher risk for liver damage), higher folate levels were associated with a 67 percent lower risk of liver cancer.41
According to the authors, increased folate in humans appear to be inversely associated with the development of liver damage and hepatocarcinoma, and that folate can offer the liver some degree of protection against damage. Folate may also mitigate against pesticide-related damage, including autism.
Your body stores approximately 10 to 30 milligrams of folate at a time, nearly 50 percent of which is in your liver. Folate is the natural form of vitamin B9 found in foods and once referred to as folacin. The word was derived from the Latin “folium,” meaning leaf. Green leafy vegetables such as spinach are abundant sources of folate, as are asparagus, broccoli, Brussels sprouts and spinach.42 Broccoli is perhaps ideal, as research43 has confirmed it helps protect against NAFLD.
Avoid folic acid supplements however. While readily absorbed, this synthetic form is not converted in the intestines like folate is. Instead, it is converted in your liver. This means folic acid can reach saturation quicker, which may result in overexposure if you’re taking supplements.
Coffee May Cut Risk of Liver Cancer
Last but not least, if you’re a coffee drinker, you may be relieved to find out that coffee appears to have a protective effect against HCC, a serious form of liver cancer and the third-most prevalent cause of death from cancer in the world. Drinking a single cup of coffee every day cuts your risk of HCC by one-fifth.44,45
If you drink more than that in a day, your risk for liver cancer is even lower. Two cups of coffee a day cut the risk by 35%, and five cups cut the risk in half. That said, excessive coffee consumption can have certain adverse effects. As noted by lead author Dr. Oliver Kennedy from the U.K.’s University of Southampton:46
“We’re not suggesting that everyone should start drinking five cups of coffee a day though. There needs to be more investigation into the potential harms of high coffee-caffeine intake, and there is evidence it should be avoided in certain groups, such as pregnant women.”
To optimize your health benefits from coffee, make sure it’s organic, and drink it black, without milk or sugar. A far better alternative would be “bulletproof coffee,” where you add butter or MCT oil to the coffee instead of sweeteners.
Researchers used computational analyses to evaluate the performance of 10 medications against the Omicron variant, finding that ivermectin outperformed all of them, including nirmatrelvir (Paxlovid) a new drug from Pfizer that has cost taxpayers $5.29 billion and costs $529 per course of treatment
Ivermectin lowers the viral load by inhibiting replication, reduces infection by 86% when used preventively, speeds recovery, protects against organ damage, lowers the risk of hospitalization and death and costs between $48 and $95 for a course of treatment depending on your location
Early treatment lowers your risk of long COVID, which includes physical and mental health conditions. According to cardiologist Dr. Peter McCullough, 50% of those sick enough to be hospitalized have symptoms of long COVID
Africa has a lower number of cases, severity of disease, hospitalizations and deaths than other areas of the world, which may be due to using prophylactic medications for endemic infections that have successfully treated COVID
At nearly no other time in history has there been this level of fear generated across the world as experienced thus far in 2020 and 2021. The depth and breadth of the strategies used to stoke those fears has been overwhelming.
Emergency use authorizations for drugs that have not proven to be effective in trials,1,2 public mask mandates for which there is no scientific evidence3,4,5 and the suppression and censorship of health information has boosted public fear over a viral illness with a survival rate of over 99%.6
Unfortunately, many of the early effective treatment strategies that can be used at home have also fallen victim to censorship. Ivermectin is one of those strategies. In a computational analysis of the Omicron variant against several therapeutic agents, data show that ivermectin had the best results.7
Yet, as you look objectively at what’s been happening across the world, the fear being generated is not one-sided. The suppression of information by corporations, government agencies and the pharmaceutical industry is one indication of their concern and how far they’re willing to go to ensure the level of fear remains high enough to manipulate behavior.
Consider the statistics from the U.S. Centers for Disease Control and Prevention. In 2019, 4.6% of the U.S. population was diagnosed with heart disease.8 The population at the end of 2019 was 328,239,523.9 This means there were 15,099,018 people with heart disease in the U.S. in 2019. There were 696,962 people who died that year from heart disease,10 which is a death rate of 4.6%.
This is 20 times greater than the death rate from COVID-19. Yet these same agencies were not lobbying for mandates against soda or sugar-laden foods; they weren’t banning smoking and they weren’t mandating exercise — all heart disease risk factors.11
The censorship and suppression of information has hobbled early treatment of COVID-19 in many western nations. Through 2020, public health experts12,13 and the mainstream media14,15 warned against the use of hydroxychloroquine and ivermectin. Both are on the World Health Organization’s list of essential drugs,16 but the benefits have been ignored by public health officials and buried by the media.
Newest Ivermectin Study Showed Best Results Against COVID
This study on Cornell University’s preprint website has not yet been peer-reviewed. Researchers used a computational analysis to look at the Omicron variant, which has demonstrated a lower clinical presentation and lower hospital admission rates.17
After having retrieved the complete genome sequence and collecting 30 variants from the database, the researchers analyzed 10 drugs against the virus, including:
Nirmatrelvir
Ritonvir
Ivermectin
Lopinavir
Boceprevir
MPro 13b
MPro N3
GC-373
GC376
PF-00835231
The researchers found that each of the drugs had some degree of effectiveness against the virus and most were currently in clinical trials. They used molecular docking to find that the mutations in the Omicron variant didn’t significantly affect the interaction between the drugs and the main protease.
An analysis of all 10 drugs found that ivermectin was the most effective drug candidate against the Omicron variant. The testing included Nirmatrelvir (Paxlovid), which is the new protease inhibitor for which the FDA provided an emergency use authorization against COVID in December 2021.18
In other words, Pfizer released a new drug which cost the U.S. taxpayers $5.29 billion or $529 per course of treatment19 and which received an EUA despite the availability of a similar drug that has proven to be more effective and is cheaper, priced between $4820 and $9521 for 20 pills depending on your location.
How Ivermectin Works
Ivermectin is best known for its antiparasitic properties.22 Yet, the drug also has antiviral and anti-inflammatory properties. Studies have shown that ivermectin helps to lower the viral load by inhibiting replication.23 A single dose of ivermectin can kill 99.8% of the virus within 48 hours.24
A meta-analysis in the American Journal of Therapeutics25 showed the drug reduced infection by an average of 86% when used preventively. An observational study26 in Bangladesh evaluated the effectiveness of ivermectin as a prophylaxis for COVID-19 in health care workers.
The data showed four of the 58 volunteers who took 12 mg of ivermectin once a month for four months developed mild COVID symptoms as compared to 44 of the 60 health care workers who declined the medication.
Ivermectin has also been shown to speed recovery, in part by inhibiting inflammation and protecting against organ damage.27 This pathway also lowers the risk of hospitalization and death. Meta analyses have shown an average reduction in mortality that ranges from 75%28 to 83%.29,30
Additionally, the drug also prevents transmission of SARS-CoV-2 when taken before or after exposure.31 Added together, these benefits make it clear that ivermectin could all but eliminate this pandemic.
Early Intervention Lowers Long COVID and Hospitalization
Some people who have had COVID-19 seem to be unable to fully recover and complain of lingering symptoms of chronic fatigue. Others struggle with mental health problems. One study,32,33 in November 2020, found 18.1% of people who had COVID-19 received their first psychiatric diagnosis in the 14 to 90 days after recovery. Most commonly diagnosed conditions were anxiety disorders, insomnia and dementia.
These symptoms have come to be called long COVID, long-haul COVID, post-COVID syndrome, chronic COVID or long-haul syndrome. They all refer to symptoms that persist for four more weeks after an initial COVID-19 infection. According to Dr. Peter McCullough, board-certified internist and cardiologist, 50% of those who have been sick enough to be hospitalized will have symptoms of long COVID:34
“So, the sicker someone is, and the longer the duration of COVID, the more likely they are to have long COVID syndrome. That’s the reason why we like early treatment. We shorten the duration of symptoms and there’s less of a chance for long COVID syndrome.”
Some of the common symptoms of long COVID include shortness of breath, joint pain, memory, concentration or sleeping problems, muscle pain or headache and loss of smell or taste. According to McCullough, a paper presented by Dr. Bruce Patterson at the International COVID Summit in Rome, September 11 to 14,35 2021:36
“… showed that in individuals who’ve had significant COVID illness, 15 months later the s1 segment of the spike protein is recoverable from human monocytes. That means the body literally has been sprayed with the virus and it spends 15 months, in a sense, trying to clean out the spike protein from our tissues. No wonder people have long COVID syndrome.”
It should come as no surprise that studies have also confirmed that early intervention improves mortality37 and reduces hospitalizations.38 Perhaps one of the greatest crimes in this whole pandemic is the refusal by reigning health authorities to issue early treatment guidance.
Instead, they’ve done everything possible to suppress remedies shown to work. Patients were simply told to stay home and do nothing. Once the infection had worsened to the point of near-death, patients were told to go to the hospital, where most were routinely placed on mechanical ventilation — a practice that was quickly discovered to be lethal.
However, as the featured study39 and others have demonstrated,40 ivermectin is one of the successful treatment protocols that can be used against SARS-CoV-2.
Africa Has Lowest Case and Death Rate, Likely From Ivermectin
Across the world, countries have taken different approaches to address the spread of the virus.41 The steps taken in Africa varied depending on the country, yet the infection and death rates were relatively stable and low across the continent.42
In the last year there have been reports of small areas in the world where the number of infections, deaths or case-fatality rates have been significantly lower than the rest of the world. For example, India’s Uttar Pradesh State43 reported a recovery rate of 98.6% and no further infections.
However, the entire continent of Africa appears to have sidestepped the massive number of infections and deaths predicted for these poorly funded countries with overcrowded cities. Early estimations were that millions would die, but that scenario has not materialized. The World Health Organization has called Africa “one of the least affected regions in the world.”44
There are several factors that may influence the infection rate in Africa. A study from Japan demonstrates that after just 12 days that doctors were allowed to legally prescribe Ivermectin to their patients, the cases dropped dramatically.45
The chairman of the Tokyo Medical Association46 had noticed the low number of infections and deaths in Africa, where many use ivermectin prophylactically and as the core strategy to treat onchocerciasis,47 a parasitic disease also known as river blindness. More than 99% of people infected with river blindness live in 31 African countries.
In addition to ivermectin use in Africa, other medications are also commonly available, such as hydroxychloroquine and chloroquine, which have long been used in the treatment and prevention of malaria,48 also endemic in Africa.49 In America, Dr. Vladimir Zelenko has published successful results using hydroxychloroquine and zinc against COVID-19.50,51,52
Finally, Artemisia annua, also known as sweet wormwood, is an herb used in combination therapies to treat malaria.53 It was used in traditional Chinese medicine for more than 2,000 years to treat fever. Today artemisinin, a metabolite of Artemisia, is the current therapeutic option for malaria. The plant has also been studied since the 2003 SARS outbreak for the treatment of coronaviruses, with good results.54,55
In other words, whether by design or default, the medications that have proven to be successful against the virus are commonly used in Africa for other health conditions. While Pfizer tests the short- and long-term effects of a genetic experiment on Israel’s population,56 it appears one continent has demonstrated administration of a 30-year-old, inexpensive drug with a known safety profile could reduce the cases, severity and mortality from this infection.
The question that must be asked and answered to get to the bottom of this plandemic is what is blinding mainstream media, government agencies, public health experts, medical associations, doctors, nurses, and your next-door neighbor from recognizing and speaking out in support of science?
Watch “Health Ranger Report with Mike Adams” on Brighteon.tv every weekday from 3:00 pm – 3:30 pm est
Visit The hhr Brighteon channel: https://www.brighteon.com/channels/hrreport
Sign up for free 100% real uncensored health email newsletters at: naturalnews.com
At Natural News listen to podcasts, audiobooks, read blog posts, current news reports, find out about events and more. Natural News is defending health, life, and liberty!
Join Brighteon Social, the pro-liberty social network: https://brighteon.social/about
Shop and visit – healthrangerstore.com & brighteonstore.com
Uncensored and Independent Media News – newstarget.com
All the news they don’t want you to see – censored.news
Audiobooks – https://audiobooks.naturalnews.com/
Thanks to our Friends and Visitors who stop by to watch our channel, and who like and subscribe. SecureLife is an outreach of Omega Fellowship, together walking and talking with Christ on the road and in our homes, the two main places where we spend our lives, where Christ spent most of His ministry! Strong Homes Build Strong Nations!
A decadent nation without repentance is a nation without hope. WE MUST HAVE REVIVAL!!
GeoEngineeringWatch.org – One hour weekly broadcast for Saturday February 12, 2022
Absolutely confirmed, graphene is an ingredient that [they] are spraying into our atmosphere on which all life depends. It’s in our rain and snow. It’s an ingredient in the clot-shots they’re desperately trying to jab into everyone. There’s a very bad reason for it.
Dark Journalist Daniel Liszt Interviews Catherine Austin Fitts
As She Reveals The Global Control Coup!
#Fitts #CBDC #CentralBank #BlackBudget
IT’S HAPPENING NOW!
Former Assistant HUD Secretary and Wall Street Dillon Read & Co. Partner Catherine Austin Fitts returns to the Dark Journalist show and reveals how the Central Bankers and the Deep State have implemented a worldwide surveillance and transaction tracking infrastructure to harvest humanity physically, financially and spiritually. Catherine sees this as a time to choose between freedom and tyranny and suggests we have a limited time to restore the Constitution and Rule of Law.
MORE…
CBDC
Bitcoin
UFOs
Black Budget
Digital Tyranny
Support Dark Journalist Now!
We are 100 Percent Independent and Supported by Viewers like YOU! You can make sure this important work continues by subscribing to Dark Journalist here: https://darkjournalist.com/s-subscribe.php
Scott Schara is sharing the heartbreaking details of how hospital staff mistreated his daughter with Downs Syndrome and ultimately left her to die while he cried out for them to step in. You won’t believe all of the rules, regulations, and laws the hospital broke with seemingly impunity because of CARES ACT dictates that give the doctors immunity from liability. Don’t miss his warning to others so that no family has to go through what his has.
ABOUT US
We take long interviews, lectures and documentaries and break them into smaller segments, highlighting the best and most logical points. The result is a compilation of the greatest video clips from alternative media sources. We believe this service is indispensable in the emotionally-charged and polarized society in which we live, because it creates more concise and relevant content that can be found and shared faster and, hopefully, understood more easily. Please support our efforts by making a donation and by sharing our website with others.
I was surfing @gettr today (great content on there by the way) and I came acroos a poster named kim Neville and I want to give her a big shoutout for posting all great content today and I used her protest content in this video. All I can say is that if I lived in France I would be livid at the heavy handedness of Macron’s thug cops in dealing with their protesters. I can guarantee you that if it gets like that here in Canada when they go to removing the protesters Canada will erupt like it will be a bench clearing brawl in hockey. These Davos Table of Rome, New World Order Dictatators days are numbered Netherlands Mark Rutte, France’s Emmanuel Macron, Trudeau here in Canada, and Australia’s Scott Morrison.
Across the world, from Asia, the Middle East, Europe, and North America, globalists are forced to back down after facing massive public pressure and raw facts of science! Alex Jones is taking calls & laying out all the incredible developments on the NEW giant trucker convoy’s journey to DC! The chain reaction for liberty has begun as people are waking up and discovering the horrible truths of what REALLY happened over the last two years!
Found this Fantastic Music Video on Telegram. Not sure who put this together, so sorry cannot give credit to the contributor. It was to awesome not to share!
Stew Peters Show
Mother of three, co-founder of the Health Freedom Summit, and a fierce fighter against the oppressive and unjust mandates, Alanah Newman joined the Stew Peters Show on Friday to discuss the rising infertility rate, the mRNA shot, and her focus to break through the mass formation that plagues our society.
STORY AT-A-GLANCE
Podcaster and certified industrial hygienist, Stephen Petty, is encouraged by statements recently made by former commissioner of the FDA, Dr. Scott Gottlieb, in which he said that masks don’t provide a lot of protection
National data from 2016 to 2019 show that relational and social risks increase the likelihood of mental, emotional and behavioral health issues in children. Children have experienced a rise in both factors throughout 2020 and 2021
A Canadian public school teacher wrote about her high school students’ behavior in the past two years, citing disengagement, shame, a fundamental alteration in their understanding of themselves, learning loss and an unwillingness to continue “living like this”
Not all educators are interested in protecting the mental health of their charges, as demonstrated by one principal at Garrison Elementary School in Washington, D.C., who is proud of the shaming he does as a vaccine “advocate” for his school, which boasts an 80% shot rate
One U.K. Freedom of Information Act request showed there were three deaths caused solely by COVID-19 since the start of the pandemic in children under 17, as compared to the 38,966 injuries and 79 deaths in the same age group reported in VAERS
As Stephen Petty, certified professional engineer, industrial hygienist and safety professional, points out in this short 11-minute podcast, the truth about masks and the Plandemic is slowly leaking out. However, since mainstream media are not universally covering these stories, it is incumbent on us to ensure that our friends and family are informed.
January 2, 2022, Dr. Scott Gottlieb, who had served as the commissioner of the Food and Drug Administration until 2019 and is now a special partner at Pfizer, was interviewed on Face the Nation. When asked about cloth masks, Gottlieb said they “aren’t going to provide a lot of protection, that’s the bottom line. This is an airborne illness. It could protect better through droplet transmission … but not something like this coronavirus.”1
Despite documentation from the Centers for Disease Control and Prevention as of January 26, 20222 that just 770 children aged 17 and under had died in two years, between 2020 and 2022, from COVID-19 — 0.00023369% of the U.S. population — Gottlieb continues to promote the idea that COVID-19 may be a serious threat to young children.
Yet, the atrocities being perpetrated on children in the name of public health is not warranted based on the number of children affected. Collette Martin, a practicing nurse, testified before a Louisiana Health and Welfare Committee hearing December 6, 2021.3
She claimed she and her colleagues have witnessed “terrifying” reactions to the COVID shots among children — including blood clots, heart attacks, encephalopathy and arrhythmias — yet their concerns are simply dismissed.
Each of these issues present short-term and long-term challenges for children’s physical, mental and emotional health. Essentially, how society has treated the children during the last two years amounts to child abuse.
Children Demonstrating Harm From Mandatory Mask Policies
National data4 from 2016 to 2019 revealed children who experienced relational and social risks had a four times higher likelihood of having mental, emotional or behavioral problems. The researchers also found that children who experienced only relational risks were more likely to have mental, emotional and behavioral health concerns than children who experienced social risks.
Relational risks are concerned with opportunistic behavior that occur within a cooperative effort, such as a family,5 for example, substance abuse within the family. Social risk factors are a significant influence over morbidity and mortality through behavioral pathways.6 These can include socioeconomic status, social network and social support.
Children have experienced a rise in both these risk factors throughout 2020 and 2021 and the evidence of damage can be found all around you. For example, ZeroHedge reported that one speech therapist said the number of children being treated in their clinic has soared by 364% during the pandemic as compared to before the pandemic.
ZeroHedge reports, “Parents are describing their children’s speech problems as “COVID delayed,” with face coverings the primary cause of their speaking skills being seriously impaired.”7 In an article published in The Washington Post,8 three experienced infectious disease physicians and parents of school-age children, noted a pattern of behavior from children in what they call a “punitive mask culture.”9
A journalist at the San Francisco Chronicle recalls that a self-portrait her 8-year-old son drew at school had no nose or mouth.10 According to data that viral immunologist Dr. Scott Balsitis11 pulled from the CDC, children have died from flu each winter, ranging in number from 200 to over 1,000.
So,12 the 770 deaths in children from birth to 17 years since the start of the pandemic have not been greater than what has been experienced in the past from flu.
While any death is tragic, masking until all children are “safe” means ineffective and damaging masks will become a permanent part of society and will continue to drive up the number of children and students who suffer from depression,13 anxiety,14 speech problems15 and who get behind in their schoolwork.16
School Teacher Identifies More Issues
Stacey Lance is a Canadian public school teacher. She has 15 years of experience at the high school level and writes about what she has seen in the last two years during lockdowns, mandatory masking and fearmongering. In an essay called, “The Kids Aren’t Alright,” she writes:17
“It also became increasingly clear that the response to the pandemic would have immense consequences for students who were already on the path to long-term disengagement, potentially altering their lives permanently.”
She believes research data has overlooked the shame that she has watched her students suffer. Throughout the pandemic, children have been made to think their schools are “hubs for infection and themselves as vectors of disease. This has fundamentally altered their understanding of themselves.”18
She describes the times when students were physically in school during the pandemic as feeling “cold and soulless.” The learning loss was noticeable, and the students had trouble concentrating. The older students weren’t allowed a lunch break and the freshmen and sophomores had to eat while facing the front of the classroom.
Lance compares that to the kids outside of school who are “going to restaurants with their families and to each other’s houses, making the rules at school feel punitive and nonsensical.”19 Lance shared the experience of one student that appeared to echo the experience of the rest of the class, writing:20
“I try to take time at the beginning of class to ask my kids how they’re doing. Recently, one of my 11th grade students raised his hand and said that he wasn’t doing well, that he doesn’t want to keep living like this, but that he knows that no one is coming to save them. The other kids all nodded in agreement. They feel lied to — and I can’t blame them.”
Lance writes that she is more worried about the shame and worry students are feeling over breaking the rules, and how that may impact their community and families. She cites information as of the time of her writing:21
“What am I supposed to say? That 23 children22 have died from Covid in Canada during the whole of the pandemic and she is much more likely to kill someone driving a car? That kids in Scandinavia, Sweden, and the Netherlands largely haven’t had to wear masks at school and haven’t seen outbreaks because of it?
That masks are not a magic shield against the virus, and that even if she were to pass it along to a classmate, the risk of them getting seriously sick is minuscule?
I want to tell her that she can remove her mask and socialize with her friends without being worried. But I am expected to enforce the rules … It’s true that humans, by nature, are very resilient. But they also break. And my students are breaking. Some have already broken.
When we look at the COVID-19 pandemic through the lens of history, I believe it will be clear that we betrayed our children. The risks of this pandemic were never to them, but they were forced to carry the burden of it.”
‘Experts’ Use Fear to Drive Vaccine Programs
But not all educators feel the same way about protecting your children. In fact, some are at the forefront of nagging and shaming parents and students into taking a shot that has not demonstrated any effectiveness and, as you’ll read below, it has caused more injury and death than the illness.
Brigham Kiplinger, the principal at Garrison Elementary School in Washington D.C., is one such educator who spends his day combing through a call list of parents who have not vaccinated their children.23 He is described by The New York Times as a “vaccine advocate,” a job that the reporter admits is usually handled by public health officials or medical professionals.
However, he is being applauded for taking this as his central role. The reporter writes, “Largely through Mr. Kiplinger’s skill as a parent-vax whisperer, Garrison Elementary has turned into a public health anomaly: 80% of the 250 Garrison Wildcats in grades kindergarten through fifth grade now have at least one shot …”24
Kiplinger uses common shaming techniques. For example, at lunch he gets the children who have been vaccinated to raise their hand and then applauds them for their actions and urges them to keep prodding others to do the same.25
The reporter believes the genetic therapy experiment is “crucial not only to sustaining in-person education but also to containing the pandemic overall.”26 Interestingly, the reporter mentions the only reason many working parents have not vaccinated their children is logistical rather than philosophical, without mentioning parents may also be fearful of the medical challenges and risks to their child.
Organizations that have been relied on for medical education and information in the past are now putting out talking points for pediatricians and parents to encourage them to vaccinate their children.27,28 Johns Hopkins School of Public Health29 has gone as far as to post a free online training course to give parents the language needed to approach friends who are resistant to injecting their children with an experiment.
The Times reports that tips offered in the Johns Hopkins training course include sharing personal stories and to “normalize Covid vaccination by proudly telling friends and family when children get COVID shots.”30 Yet, sharing personal stories is exactly what social media platforms is censoring when it comes to COVID shot injuries.
More Children Are Dying From the Shot Than the Illness
Judging from the COVID numbers in children I discussed earlier, it is apparent that school educators and many public health and medical experts have completely ignored the data from the Vaccine Adverse Events Reporting System (VAERS) demonstrating children are being harmed by the shot in large numbers.
In fact, if you give any credence at all to VAERS, they are being injured by the vaccine in larger numbers than by the disease itself. It’s important to note the CDC makes the distinction that these deaths involved COVID-19 and were not necessarily the direct result of COVID-19.
In the U.K., a Freedom of Information Act request asked for “deaths caused solely by COVID-19, where COVID is the only cause of death listed on the death certificate, broken down by age group and gender between February 2020 up to and including December 2021.”31 The data show that in children from birth to age 19, there were three deaths in the U.K. from February 2020 to December 31, 2021.
Based on the U.K. and CDC data, it makes no sense that policymakers want to mandate a vaccine for children. According to Steve Kirsch, founder of the COVID-19 Early Treatment Fund,32 the FDA justified the vaccine based on assumptions made for a statistical model.33 Kirsch also points out the U.K. has now stopped any mask mandates, social distancing and lockdowns.
However, in Santa Clara County, California, where Kirsch lives, the mask mandate, vaccines and distancing rules remain. As he writes, “Same virus, different policymakers.”34 Kirsch was part of a team that used an engineering estimate to find the underreporting factor in VAERS was likely near 41.35 This means the number of reports in VAERS can be multiplied by 41 to reach the number likely injured by the vaccine.
When VAERS is filtered to find children from birth to 17 years, it reveals 38,966 reports and 79 deaths.36 If you extrapolate those numbers using the underreporting factor, you discover there could be roughly 1.6 million injuries and 3,239 deaths.
Underreporting to the system can happen for several reasons. Martin and others have explained that most doctors are not familiar with the system37 and filling out the VAERS report is time-consuming. As Debra Conrad found out, many hospitals do not want to report all the injuries to the system, and as Brittney Galvin revealed in a recorded conversation with a VAERS investigator,38 they are as much as one year behind in publishing reports.
A search on OpenVAERS for records of vaccine adverse events from 1990 to 202039 reveals 821,470 total reports of injuries to children in 30 years. However, since the rollout of the emergency use vaccine, the system has received a total of 1,071,854 reports in adults and children in 13 months.40
The Shot Increases Risk of Lifelong Damage
British data also show deaths among teenagers have spiked since that age group became eligible for the COVID shots,41 by an increase of 47%. Children are also at risk for potentially lifelong health problems from the experimental shot, as there are absolutely no long-term safety data on this. One of the most common problems that has emerged so far in children is myocarditis.42
This is an inflammation of the heart muscle that can cause ongoing heart problems and may even require a heart transplant. In October 2021, cardiologist Dr. Peter McCullough and Jessica Rose, Ph.D., research fellow at the Institute for Pure and Applied Knowledge in Israel, submitted a paper on myocarditis cases to the journal Current Problems in Cardiology.
The paper was ready to be published when the journal suddenly took it down. You can find the preprint on Rose’s website,43 which clearly shows that myocarditis is inversely correlated to age. This means that the risk is higher in younger individuals. The risk is also dose-dependent. The data showed boys had a six times greater risk of myocarditis after the second dose of the vaccine.
Damage to the heart muscle is often permanent and, historically, the three- to five-year survival rate has ranged from 56% to 83%.44 The data do not support the push to vaccinate children who are not experiencing severity of disease and death.
Additionally, research does not support the use of masks to filter viruses45,46,47 and even the boxes are labeled: “will not provide any protection against COVID … or any viruses or contaminants.”48 Fact checkers get around this statement by acknowledging that the box is labeled as such, but that “does not mean masks should not be worn.”49
Politifact goes one step further to extrapolate a whole new meaning, writing, “Such disclaimers don’t mean that the masks are ineffective at slowing the spread of the disease, but that they don’t protect the wearer as well as medical respirators such as the N95 recommended for use by health care professionals.”50 When:
Masks don’t work
The shot increases the risk of death and long-term health damage in children
Educators take on the role of “parent-vaccine whisperer”
There is a rising number of children and teens suffering from depression and anxiety
Children have fallen behind in their studies
You must ask yourself, ultimately, what is the goal here? Why are agencies pushing for behavior and choices that have demonstrably damaged children and may result in life-long physical and emotional disability?
STORY AT-A-GLANCE
October 4, 2020, three public health scientists launched The Great Barrington Declaration — a public health proposal that calls for focused protection of the most vulnerable while letting the rest of the world resume normal life
The Great Barrington Declaration has been signed by more than 920,000 individuals, including 46,412 medical practitioners and 15,707 scientists
It was recently revealed that Dr. Anthony Fauci, director of the National Institutes of Allergy and Infectious Diseases, and his former boss, now retired National Institutes of Health director Francis Collins, colluded behind the scenes to quash the declaration from Day 1
Focused protection is based on longstanding basic principles of public health that we have followed for decades, while lockdowns are novel, experimental strategies with no history of usefulness
Fauci and Collins had nothing in terms of actual science. They could not defend lockdowns or anything else based on science alone. So, they turned to propaganda, PR and smear tactics
October 4, 2020, three public health scientists launched The Great Barrington Declaration1 — a public health proposal that calls for focused protection of the most vulnerable while letting the rest of the world resume normal life. The declaration has since garnered more than 920,000 signatures by doctors, scientists and other health professionals who agree with its premises. The founding trio include:
Martin Kulldorf, Ph.D., a biostatistician, epidemiologist with expertise in detecting and monitoring infectious disease outbreaks and vaccine safety evaluations, and a professor of medicine at Harvard University
Sunetra Gupta, Ph.D., professor at Oxford University, an epidemiologist with expertise in immunology, vaccine development, and mathematical modeling of infectious diseases
Jay Bhattacharya, MD, Ph.D., professor at Stanford University Medical School, a physician, epidemiologist, health economist, and public health policy expert focusing on infectious diseases and vulnerable populations
In the video above, Jimmy Dore interviews Kulldorf and Bhattacharya about the declaration, and the recent revelation that Dr. Anthony Fauci, director of the National Institutes of Allergy and Infectious Diseases (NIAID) and his former boss, now retired National Institutes of Health (NIH) director Francis Collins, colluded behind the scenes to quash the declaration from day one.2
Focused Protection
The Great Barrington Declaration points out some key basic facts. First of all, it stresses that pandemic measures such as lockdowns “cause irreparable damage, with the underprivileged disproportionately harmed.” Second, it highlights the fact that the risk of death from COVID is not equal to all.
“We know that vulnerability to death from COVID-19 is more than a thousand-fold higher in the old and infirm than the young. Indeed, for children, COVID-19 is less dangerous than many other harms, including influenza.”3
Furthermore, as natural immunity within a population grows, the overall risk of infection declines. So, allowing those at low risk for complications and death to live normally, and potentially get sick but recover, actually helps protect those at greatest risk.
By having everyone isolate at home and avoid contact with others, herd immunity is postponed and the pandemic prolonged. “Our goal should … be to minimize mortality and social harm until we reach herd immunity,” the declaration explains, adding:4
“The most compassionate approach that balances the risks and benefits of reaching herd immunity, is to allow those who are at minimal risk of death to live their lives normally to build up immunity to the virus through natural infection, while better protecting those who are at highest risk. We call this Focused Protection.
Adopting measures to protect the vulnerable should be the central aim of public health responses to COVID-19. By way of example, nursing homes should use staff with acquired immunity and perform frequent testing of other staff and all visitors. Staff rotation should be minimized.
Retired people living at home should have groceries and other essentials delivered to their home. When possible, they should meet family members outside rather than inside. A comprehensive and detailed list of measures, including approaches to multi-generational households, can be implemented, and is well within the scope and capability of public health professionals.
Those who are not vulnerable should immediately be allowed to resume life as normal. Simple hygiene measures, such as hand washing and staying home when sick should be practiced by everyone to reduce the herd immunity threshold. Schools and universities should be open for in-person teaching.
Extracurricular activities, such as sports, should be resumed. Young low-risk adults should work normally, rather than from home. Restaurants and other businesses should open.
Arts, music, sport and other cultural activities should resume. People who are more at risk may participate if they wish, while society as a whole enjoys the protection conferred upon the vulnerable by those who have built up herd immunity.”
Fauci’s False Consensus
As noted by Bhattacharya in the interview above, while Fauci tried his best to create the illusion of scientific consensus — that most all scientists agreed with lockdowns, masking, social distancing and so on — there were and are just as many if not more who disagree.
The Great Barrington Declaration has been signed by more than 920,000, including 46,412 medical practitioners and 15,707 scientists. “We posed a significant problem for them,” Bhattacharya says, “because they couldn’t dismiss us as fringe.” Well, Collins certainly tried. In fact, in an October 8, 2020, email to Fauci, Collins wrote:5,6,7,8
“The proposal from the three fringe epidemiologists who met with the Secretary seems to be getting a lot of attention … There needs to be a quick and devastating published take down of its premises …”
“Don’t worry, I got this,” Fauci replied. Later, Fauci sent Collins links to newly published articles refuting the focused protection solution, including an op-ed in Wired magazine, and an article in The Nation, titled “Focused Protection, Herd Immunity and Other Deadly Delusions.”
When They Can’t Win an Argument, They Slander
As noted by Bhattacharya, Fauci and Collins had nothing in terms of actual science. They could not defend lockdowns or anything else based on science alone. So, they turned to propaganda, PR and smear tactics.
“Focused protection is based on longstanding basic principles of public health that we have followed for decades,” Kulldorf says. “Lockdowns is a new experimental thing. So, the problem for Dr. Fauci and Collins is that they don’t really have any good public health arguments. Collins is a geneticist and Fauci is an immunologist, so their experience with epidemiology and public health is limited.
You can see that in this email where Fauci was quoting Wired magazine as a take-down of The Great Barrington Declaration. They didn’t really have any good public health arguments. There were no arguments to keep the schools closed.
So, the only thing that remains then is to use slander, or smearing, or mischaracterizing your opponents, and that’s what they did. They called focused protection a ‘let it rip strategy,’ even though it’s the very opposite [of that].”
The very same tactic has been used to shut down all other counternarratives as well, be it evidence showing that masks don’t work, that the COVID shots cause harm, or that vaccine passports are moot since the shots don’t prevent you from getting infected or transmitting the virus and therefore cannot protect others, cannot confer vaccine-induced “herd immunity” and cannot end the pandemic.
COVID Jab Risk-Benefit Analysis
Unfortunately, Dore, Kulldorf and Bhattacharya all claim that the COVID shot is beneficial, or at least can be for some, and is saving lives. Kulldorf goes so far as to say that “older people who have not had COVID should certainly — a no-brainer — take this vaccine.”
While I respect their expertise, I strongly disagree with such statements. Importantly, they are not comparing the effectiveness of and protection you get from the shot, to the protection and effectiveness of preventive measures and aggressive early treatment.
I have never seen any professional make this recommendation and compare it to the alternative of optimizing vitamin D levels and providing early treatment, ideally on the first day. They are comparing it to doing nothing, which makes no sense as it should be compared to another intervention.
If you don’t take the shot, your risk of getting COVID is not 100%. If you take the shot, however, you’re 100% exposed to its risks, which are significant. Seeing how we have several different early treatment protocols with demonstrable effectiveness, reducing the risk of death even among the seriously ill by 80%, why take an experimental shot that can devastate your health, if not acutely, then over the long term?
Now, I’m not indifferent to the clearly delicate position they’re in. It’s at least possible (although far from certain) that their enthusiastic pro-jab stance is a concession to avoid the anti-vax label in order to be able to engage in the larger conversation about other pandemic measures. If they failed to take this position they would likely be even more censored.
It’s easy for the establishment to attack and smear those who express concerns about the COVID jab. It’s more difficult to sink the reputations of those who agree that the jab is “fantastic” but have concerns about other measures.
That said, Bhattacharya does point out some basic data — published by the World Health Organization — to clarify for whom the benefit of the jab might outweigh its unknown risks:
A 53-year-old has a 0.2% mortality rate from COVID, i.e., they have a 99.8% chance of surviving the infection
For every seven years of age above 53, the mortality rate doubles, so a 60-year-old has a 0.4% risk of dying from COVID, a 67-year-old risk’s is 0.8% and for a 74-year-old, it’s 1.6%
For every seven years of age below 53, the mortality rate is halved, so a 46-year-old has a 0.1% risk of dying from COVID and it dwindles into statistical zero for teens and children
80% of COVID deaths in the U.S. occur in people over 65
The average age of COVID death is above the national life expectancy
Why Vaccine Mandates Make No Sense
As Dore points out, the facts simply don’t support vaccine mandates. “I don’t see how you can be for mandates after you have this information,” he says.
The COVID jabs do not prevent transmission, and vaccinated people have just as high or higher viral load as the unvaccinated, making them just as contagious, or more so
Even if the jab reduces symptoms, they do not prevent you from contracting the virus
With Omicron being so highly contagious, the consensus seems to be that just about everyone will be exposed and contract it, thereby producing herd immunity
“If everyone’s going to get it, what does it matter who you get it from, a vaccinated or an unvaccinated person?” Dore asks. “So, how can they justify a mandate?”
COVID Jab Mandates Are Cruel and Unethical
According to Kulldorf, the establishment pushing for vaccine mandates are ignoring basic public health science. They’re also acting unethically. Demanding that a 25-year-old who already had COVID take the experimental jab that won’t provide them with a clear benefit is medically unethical.
Meanwhile, elderly people in underdeveloped countries that might benefit aren’t able to get it and that, too, Kulldorf says, is unethical. Bhattacharya agrees, saying “it’s a cruel thing we’ve done with the mandates.” People who risked their lives during the first year of the pandemic, when little was known about the infection, are now being fired because they don’t want a shot they don’t need.
The vaccine does not stop transmission. Given that, what logic is there for a mandate? There isn’t any. It’s just cruel and unethical. ~ Dr. Jay Bhattacharia
Doctors, nurses, first responders, truckers, grocery store clerks — they all worked through 2020 and were exposed on the frontlines. Those who recovered and have natural immunity are now being discarded like yesterday’s trash for no good reason.
Naturally immune health care workers, for example, would normally be invaluable. Now they’re being fired and replaced with workers who have fragile and temporary protection at best, which is beyond irrational if you’re trying to prevent outbreaks.
“The vaccine does not stop transmission,” Bhattacharya says. “Given that, what logic is there for a mandate? There isn’t any. It’s just cruel and unethical.”
The Bizarre Disappearance of Natural Immunity
Kulldorf points out that we’ve known about natural immunity for 2,500 years, and there’s absolutely no reason to assume that this virus would be completely different from any other virus and fail to confer robust immunity after you’ve recovered.
But even if you were unsure, real-world data confirm that it does confer immunity. He cites data from Israel, showing people who have received the jab are 27 times more likely to come down with symptomatic infection compared to those who had prior COVID infection. So, we know that natural immunity is far better than the jab.
It’s a very curious phenomenon that has occurred, and Bhattacharya and Kulldorf both admit being very confused by it, and that is that seemingly hundreds of scientists have sided with narratives that everyone knows to be false — such as the denial of natural immunity.
Bhattacharya describes being utterly shocked reading a statement signed by 100 scientists declaring that natural immunity did not occur after COVID infection. He believes the scientific community was so caught up in the fear of being “canceled” that they either silenced themselves or went along with things they knew were untrue.
He also points out that the World Health Organization went so far as to change the definition of herd immunity after The Great Barrington Declaration was published. The new definition basically denies the existence of natural herd immunity and pretends that it can only be achieved through mass vaccination, which has never been the case.
“It’s a weird power we have,” Bhattacharya says, tongue-in-cheek. “We released [The Great Barrington Declaration] and we made the World Health Organization stupider.”
Blatant Lies Being Told About Children’s Risk of COVID
Dore also highlights other blatant lies. Two-thirds of parents are very reluctant to give their children the COVID jab, so the propaganda machine is in full swing trying to make parents more afraid of COVID than they are of the shot. He plays a news clip in which it’s claimed that:
Since the beginning of the pandemic, more than 8,000 children have been hospitalized with COVID, a third of those ending up in the ICU
146,000 children have died from COVID since the beginning of the pandemic
COVID is now in the Top 10 causes of death among children
“That’s just false,” Bhattachary says. The news clip goes on to claim that:
The shot has been proven safe for children
That there are “no side effects” in children
Side effects only occur within the first couple of months after the jab, and
“Long-term concerns are very theoretical” and would be “rare at the most” whereas the effects of COVID itself “could be devastating”
“He just said there are NO side effects from the vaccine,” Dore says. “[That’s] also a lie!” Bhattacharya commented on the clip calling it “absolutely shocking, filled with absolute lies.” Aside from the lack of proven safety, they also lied about COVID causing long-term problems in children. Bhattacharya cites a recent large-scale study that concluded “long-COVID in children were of short duration.”
“They’re creating this sense of panic in parents, and it’s just evil,” Bhattacharya says. “What happens is the parents then end up making decisions for their kids that end up harming them, on the basis of this false information.”
Aggressive Early Treatment Is Key
I hope you take the time to listen to the full interview, as they cover far more than I’ve reviewed here. It’s an interesting conversation and Jimmy is profoundly entertaining as he educates us on the facts. In the latter half of the interview, they also discuss the issue of treatment, and the irrational stance that discussing and using effective treatment will result in people not getting the COVID jab.
Bhattacharya expresses exasperation at this, noting that when a patient is ill, you have to do everything in your power to treat them. You can’t ignore treatment for fear they might not want a vaccine later. And you can’t not treat people simply because others might decide they don’t want the vaccine because they know they can get treated if they get sick.
Indeed, the suppression and denial of early treatment is perhaps the most egregious and deadly lie of all. At first signs of symptoms, you need to begin treatment. We now know that treating early and aggressively will prevent the vast majority from needing hospital care or dying. Early treatment also radically lowers your risk of long-COVID. At this point, we have several early treatment protocols with demonstrated effectiveness, including:
The Front Line COVID-19 Critical Care Alliance’s (FLCCC’s) prevention and early at-home treatment protocol. They also have an in-hospital protocol and long-term management guidance for long-haul COVID-19 syndrome. You can find a listing of doctors who can prescribe ivermectin and other necessary medicines on the FLCCC website
The AAPS protocol
Tess Laurie’s World Council for Health protocol
America’s Frontline Doctors
Based on my review of these protocols, I’ve developed the following summary of the treatment specifics I believe are the easiest and most effective.
While influenza can indeed be deadly in rare cases, these deaths are typically the result of secondary infections, not the flu virus itself
Research has highlighted the link between influenza and severe sepsis (blood poisoning). Symptoms of sepsis can mimic flu, and are often overlooked. Without prompt treatment, the condition can be deadly
Use of intravenous vitamin C, hydrocortisone and thiamine has been shown to reduce sepsis mortality nearly fivefold, from 40 to 8.5 percent
Optimizing your vitamin D level is a far more potent preventive strategy than getting a seasonal flu vaccine. People with significant vitamin D levels may reduce their risk of respiratory infections such as influenza by 50%
People with higher vitamin D levels may also benefit from additional vitamin D, reducing their risk of flu by 10%, which equals the effectiveness of the seasonal flu vaccine, including this year’s vaccine
This article was previously published February 1, 2018, and has been updated with new information.
As the COVID pandemic enters its second year, the U.S. Centers for Disease Control and Prevention is ramping back up on its influenza recommendations, and stressing that it’s important to get a flu vaccine along with your COVID shots and boosters.1 The CDC is urging everyone aged 6 months and older to get a flu shot, with rare exceptions.2
During the height of the pandemic, influenza cases appeared to drop or nearly disappear, but with the 2021-2022 flu season, more flu cases are being reported. By the end of December 2021, the CDC reported that two children had already died of flu, and that flu hospitalizations were rising quickly.3 But how many deaths and hospitalizations are actually due to flu?
Many Flu ‘Deaths’ Are Actually From Secondary Infections
While influenza can indeed be deadly in rare cases, what most health experts fail to tell you is that these deaths are typically the result of secondary infections, not the flu virus itself. Importantly, research has highlighted the link between influenza and severe sepsis — a progressive disease process initiated by an aggressive, dysfunctional immune response to an infection in the bloodstream (which is why it’s sometimes referred to as blood poisoning).
Symptoms of sepsis are often overlooked, even by health professionals, and without prompt treatment, the condition can be deadly. Not only that, sepsis also goes hand in hand with COVID-19 infection, particularly in patients in intensive care with COVID.4
Unfortunately, conventional treatments often fail, and most hospitals have yet to embrace the use of intravenous (IV) vitamin C, hydrocortisone and thiamine,5 which has been shown to reduce sepsis mortality from 40% to a mere 8.5%.6,7
How Influenza May Cause Lethal Sepsis
A decade and more ago, severe sepsis was generally associated with bacterial infections, but by 2013, viral infections like flu, and now COVID, had become a prominent cause of sepsis.8 To complicate matter even more, as noted in the video above, some sepsis symptoms also resemble influenza, which can lead to tragedy. The video offers guidelines on how to tell the difference between the two.
Sepsis, without doubt, requires immediate medical attention, whereas most people will successfully recover from the flu with a few days to a week of bedrest and fluids. Just how influenza can lead to sepsis is a somewhat complex affair, described as follows:9
“Regardless of the etiologic agent, the inflammatory response is highly interconnected with infection. In the initial response to an infection, severe sepsis is characterized by a pro-inflammatory state, while a progression to an anti-inflammatory state develops and favors secondary infections …
In the predominant pro-inflammatory state, Th1 cells activated by microorganisms increase transcription of pro-inflammatory cytokines such as tumor necrosis factor (TNF-α), interferon-γ (INF-γ), and interleukin-2 (IL-2).
[C]ytokines … released from endothelial cells and subsequently from macrophages can induce lymphocyte activation and infiltration at the sites of infection and will exert direct antiviral effects. Subsequently, with the shift toward an anti-inflammatory state, activated Th2 cells secrete interleukin-4 (IL-4) and interleukin-10 (IL-10).
In certain situations, T cells can become anergic, failing to proliferate and produce cytokines. Type I IFN has a potent anti-influenza virus activity; it induces transcription of several interferon stimulated genes, which in turn restrict viral replication. However, influenza virus developed several mechanisms to evade IFN response …
Viral infections such as the influenza virus can also trigger deregulation of the innate immune system with excessive cytokines release and potential harmful consequences. An abnormal immune response to influenza can lead to endothelial damage … deregulation of coagulation, and the consequent alteration of microvascular permeability, tissue edema, and shock.”
Signs and Symptoms of Sepsis
Common signs and symptoms of sepsis to watch out for include:10
A high fever
Inability to keep fluids down
Rapid heartbeat; rapid, shallow breathing and/or shortness of breath
Lethargy and/or confusion
Slurred speech, often resembling intoxication
Should a few or all of these be present, seek immediate medical attention to rule out sepsis. Also inform the medical staff that you suspect sepsis, as time is of the essence when it comes to treatment. As noted in the featured video, hydration is of utmost importance, as much of the damage caused by sepsis begins with fluid loss.
Preventive Strategies to Reduce Your Chances of Infections
Your immune system is your first-line defense against all types of infections, be they bacterial or viral, so the most effective way to avoid coming down with flu is to bolster your immune function. While health officials claim getting an annual flu shot is the best way to ward off influenza, the medical literature actually suggests vitamin D optimization may be a far more effective strategy, and the evidence for this goes back at least a decade.
Dr. John Cannell, founder of the Vitamin D Council, was one of the first to introduce the idea that vitamin D deficiency may actually be a causative factor in influenza. His hypothesis11 was initially published in the journal Epidemiology and Infection in 2006.12 It was subsequently followed up with another study published in the Virology Journal in 2008.13
The following year, a large, nationally representative study14 confirmed that people with the lowest vitamin D levels indeed reported having significantly more colds or cases of the flu. Similar findings have been reported with vitamin D status and COVID, with several studies showing that persons with low vitamin D levels not only are more likely to be susceptible to the infection, but have a higher risk of hospitalization and death.15,16,17
With flu, a number of studies confirm the importance of your vitamin D status in fighting this viral infection. In 2017, for example, a scientific review18,19 concluded that vitamin D supplementation boosts immunity and cuts rates of both cold and flu.
In all, 25 randomized controlled trials were included in the review, involving nearly 11,000 individuals from more than a dozen countries. People with significant vitamin D deficiency (blood levels below 10 ng/mL), taking a vitamin D supplement reduced their risk of respiratory infections such as influenza by 50%.
People with higher vitamin D levels also benefited, although not as greatly. Overall, they reduced their risk by about 10%, which the researchers stated was about equal to the effect of flu vaccines. Coincidentally, 10% was the effectiveness rate of the 2017-2018 flu vaccine.20
The take-home message here is that vitamin D supplementation far exceeds the flu vaccine in terms of effectiveness, and the more deficient you are, the greater its protective effects when you supplement.
Aside from vitamin D, loading up on vitamins B1 and C may go a long way toward keeping you healthy through the flu season and beyond. Influenza has been successfully treated with high-dose vitamin C.21 Taking zinc lozenges at the first sign of a cold or flu can also be helpful.
Zinc boosts immune function and plays a vital role in activating your body’s T cells (white blood cells tasked with destroying infected cells). If you fall victim to frequent bacterial infections or colds, your body might be trying to tell you it needs more zinc.
Be Aware of This Lifesaving IV Protocol
If you or a loved one contracts sepsis, whether caused by influenza or some other infection, please remember that a protocol of IV vitamin C with hydrocortisone and thiamine (vitamin B1) can be lifesaving.22 So, urge your doctor to use it. Chances are, they might not even be aware of it.
This sepsis treatment protocol was developed Dr. Paul Marik23,24 when he was a critical care doctor at Sentara Norfolk General Hospital in East Virginia, and clinical use has proven it to be remarkably effective for the treatment of sepsis, reducing mortality nearly fivefold.
Marik’s retrospective before-after clinical study showed that giving patients IV vitamin C with hydrocortisone and vitamin B1 for two days reduced mortality from 40% to 8.5%. Of the 50 patients treated, only four died, and all of them died from their underlying disease, not sepsis. Importantly, the treatment has no side effects and is inexpensive, readily available and simple to administer, so you really have nothing to lose by trying it.
The only contraindication is if you are glucose-6-phosphate dehydrogenase (G6PD) deficient (a genetic disorder).25 G6PD is an enzyme your red blood cells need to maintain membrane integrity.
High-dose IV vitamin C is a strong pro-oxidant, and giving a pro-oxidant to a G6PD-deficient individual can cause their red blood cells to rupture, which could have disastrous consequences. Fortunately, G6PC deficiency is relatively uncommon, and can be tested for.
People of Mediterranean and African decent are at greater risk of being G6PC deficient. Worldwide, G6PD deficiency is thought to affect 400 million individuals, and in the U.S., an estimated 1 in 10 African-American males have it.26
Flu Vaccines Don’t Usually Live Up to Their Hype
Sadly, flu deaths are inevitably used to incite fear, and the recommended remedy is annual flu vaccination, even when statistics show the vaccines don’t perform the way they’re hyped.
For example, in January 2015, U.S. government officials admitted that, in most years, flu shots are — at best — 50 to 60% effective at preventing lab confirmed type A or B influenza requiring medical care.27 And, as mentioned, the 2017-2018 flu vaccine had an effectiveness rating of just 10%, due to it being poorly matched, yet the call for flu vaccination remained.
Many also gloss over the fact that flu deaths also occur in those who have been vaccinated. Such was the case with this 8-year-old boy in Arkansas, featured in this CNN report.
Yet, despite year after year of dismal efficacy numbers, the CDC continues to push the flu vaccine. In December 2021, they said that, despite indications that the H3N2 protection for this season’s vaccine may not live up to expectations, they still recommend getting the shot, as flu could be more serious in the 2021-2022 season:28
“Flu vaccination has many benefits yet early data suggest the number of people who have been vaccinated so far this season is down, especially among certain higher risk groups such as pregnant people and children.
Lower vaccination rates and reduced population immunity resulting from historic low flu activity since March 2020 could lead to widespread flu, with more serious illnesses. With ongoing COVID-19 activity, hospitals could be further stressed this winter.”
But, considering the many studies showing flu vaccines have a dismal success rate even when well-matched to circulating viral strains, the fact that vaccination continues to be touted as your first line of defense against influenza suggests this annual campaign is more about generating conformity for profit, opposed to actually improving and protecting public health.
Flu Vaccine Likely Raises Your Risk of Illness
The fact that flu vaccines offer negligible protection against flu is bad enough, but evidence suggests the vaccine may even make you more susceptible to the disease. For example, Canadian researchers found that annual flu vaccination appears to increase your risk of pandemic illness, and cause more serious bouts of illness.
Data collected from Canada and Hong Kong during 2009 to 2010 showed that people who received the seasonal flu vaccine in 2008 had twice the risk of getting the H1N1 “swine flu,” compared to those who had not received a flu shot.29
A well-publicized ferret study30 confirmed these results. Research31 published more than a decade ago, in 2011, also warned that the seasonal flu vaccine appears to weaken children’s immune systems and increases their chances of getting sick from influenza viruses not included in the vaccine.
Some health experts claim flu vaccination will help you develop resistance against strains that are not included in the vaccine, but research has actually shown the complete opposite to be true.
When blood samples from healthy, unvaccinated children and children who had received an annual flu shot were compared, the unvaccinated group had naturally built up more antibodies across a wider variety of influenza strains compared to the vaccinated group.32 Flu vaccines are also associated with debilitating and potentially lifelong side effects such as Guillain–Barré syndrome and chronic shoulder injury related to vaccine administration (SIRVA).33
But what about the claim that you might contract influenza from your flu shot? There are many anecdotal reports of people developing the worst bout of influenza they’ve ever had following a routine flu vaccination and, indeed, a Chinese study34 published in 2012 appears to support such claims, finding that children had a 4.4 higher chance of contracting a viral upper respiratory infection following seasonal flu vaccine administration.
Researchers have also highlighted the influence of bias in studies looking at influenza vaccine effectiveness. As noted in one 2010 study,35 ”Forgoing vaccination predicted death in those who had received vaccinations in the previous five years, but it predicted survival in patients who had never before received a vaccination. We conclude that bias is inherent in studies of influenza vaccination and death among elderly patients.”
Beware: Tamiflu Can Trigger Psychosis
Should you or your child come down with the flu and your doctor or pediatrician recommends Tamiflu,0 you should know this antiviral drug has been shown to shorten the duration of flu symptoms by less than 17 hours36,37 It also does not reduce viral transmission and does not lower your risk of complications from the flu, such as pneumonia.38,39 Scientist have also warned that the risks far outweigh the benefits.40
These risks include convulsions, brain infections, psychosis and other neuropsychiatric problems. Tamiflu made recent headlines after a 6-year-old girl started hallucinating and attempted to jump out a second story window.41 “I don’t think the 16 hours of symptom relief from the flu is worth the possible side effects that we went through,” the girl’s father told ABC7 News.42
Indeed, a number of studies have observed that Tamiflu may cause psychiatric symptoms. Research43 published in 2015 reported the case of a 22-year-old man who “complained of mood swings, suicidal feelings, auditory hallucinations, memory deterioration and insomnia” after taking the drug. Other studies44 have found more than half of all children taking Tamiflu suffer side effects from the drug.45
Dangerous Lies Told by the CDC
Prior to the global H1N1 scare, the U.S. government stockpiled $1.5 billion of this basically useless antiviral — money that could have been spent in far better ways than merely enriching Roche’s company pockets. As noted in an article about Tamiflu by The Atlantic, “The only people helped by the proven-to-be-ineffective drug are its manufacturers.”46
A 2013 Forbes article47 also spelled out a number of flaws in the science behind Tamiflu, and how benefits were overstated. Despite all of this overwhelming evidence, the CDC to this day continues to recommend both flu vaccines and antiviral drugs like Tamiflu.48,49 They even continue to claim antiviral drugs “may prevent serious flu complications” — though the evidence clearly shows Tamiflu does no such thing.
The take-home message here is to do your homework, and not blindly follow public health recommendations. Also avoid falling prey to unreasonable fears. All deaths are tragic, but people die from influenza with and without flu vaccines. People also die without certain drugs, and from drugs.
Remember, optimizing your vitamin D to a level of 60 to 80 ng/mL may be one of the most effective flu prevention strategies out there. Also familiarize yourself with the signs and symptoms of sepsis, and urge your doctor to administer Marik’s IV vitamin C protocol should you or a loved one be diagnosed with sepsis. It just might save your life.
People with natural COVID-19 immunity continue to be discriminated against and are still expected to get double- or triple-jabbed in order to comply with vaccine mandates — an unprecedented move in history
New data from the U.S. Centers for Disease Control and Prevention show that prior COVID-19 infection, i.e., natural immunity, is more protective than COVID-19 injections
The U.S. Supreme Court recently upheld a vaccine mandate at the Centers for Medicare & Medicaid Service (CMS), which affects 10.4 million health care workers employed at 76,000 medical facilities, making no exceptions for those who have natural immunity to COVID-19 due to prior infection
One study found that the risk of reinfection with SARS-CoV-2 decreased by 80.5% to 100% among people who had previously had COVID-19
In Switzerland, residents who have had COVID-19 in the past 12 months are considered to be equally as protected as those who’ve been injected
COVID-19 injection mandates raise glaring questions, with a key one revolving around natural immunity. Your immune system is designed to work in response to exposure to an infectious agent. Your adaptive immune system, specifically, generates antibodies that are used to fight pathogens that your body has previously encountered.1
If you’ve had COVID-19, the research is strong that you’re well protected against reinfection. New data from the U.S. Centers for Disease Control and Prevention even show that prior COVID-19 infection, i.e., natural immunity, is more protective than COVID-19 injections.2
However, people with natural immunity continue to be discriminated against and are still expected to get double- or triple-jabbed in order to comply with vaccine mandates — an unprecedented move in history.
‘Unprecedented’ Denial of Natural Immunity
The U.S. Supreme Court recently upheld a vaccine mandate at the Centers for Medicare & Medicaid Service (CMS), which is part of the U.S. Department of Health and Human Services. The mandate affects 10.4 million health care workers employed at 76,000 medical facilities,3 making no exceptions for those who have natural immunity to COVID-19 due to prior infection.
Speaking with The Epoch Times, Dr. Scott Atlas, a former White House COVID-19 Task Force adviser, called the SCOTUS ruling “another denial of scientific fact,” adding:4
“Our continued denial of superior protection in recovered individuals, with or without vaccination, compared to vaccinated individuals who’ve never had the infection … the denial of that is simply unprecedented in modern history. Proven fact and decades of fundamental immunology are somehow denied. If we are a society where the leaders repeatedly deny the fact, I’m very concerned about the future of such a society.”
While upholding the vaccine mandate for medical facilities that accept Medicare or Medicaid payments, SCOTUS blocked a White House mandate that would have required private companies with 100 or more employees to ensure staff have gotten a COVID-19 injection or were tested regularly for COVID-19 — or face steep fines.
The Labor Department’s Occupational Safety and Health Administration (OSHA) was supposed to be in charge of enforcing the rule, which would have affected more than 80 million U.S. workers.5 Of their decision, the court noted:6
“Although Congress has indisputably given OSHA the power to regulate occupational dangers, it has not given that agency the power to regulate public health more broadly. Requiring the vaccination of 84 million Americans, selected simply because they work for employers with more than 100 employees, certainly falls in the latter category.”
Despite the private business vaccine mandate being struck down, the White House urged states and businesses to voluntarily enact sweeping vaccine mandates,7 again ignoring the fact that many people are already naturally immune.
World No. 1 tennis player Novak Djokovic is a prime example — despite previously having COVID-19, and therefore having acquired natural immunity, he was barred from playing at the Australian Open because he didn’t get the COVID-19 injection.8
Natural COVID-19 Immunity Superior to Shot-Derived Immunity
Data from New York and California health officials, published in the CDC’s Morbidity and Mortality Weekly Report, show that people who had previously had COVID-19 were far better protected against COVID-19 infection with the Delta variant than people who had been jabbed. The report states:9
“By the week beginning October 3, compared with COVID-19 cases rates among unvaccinated persons without a previous COVID-19 diagnosis, case rates among vaccinated persons without a previous COVID-19 diagnosis were 6.2-fold (California) and 4.5-fold (New York) lower; rates were substantially lower among both groups with previous COVID-19 diagnoses, including 29.0-fold (California) and 14.7-fold lower (New York) among unvaccinated persons with a previous diagnosis, and 32.5-fold (California) and 19.8-fold lower (New York) among vaccinated persons with a previous diagnosis of COVID-19.
During the same period, compared with hospitalization rates among unvaccinated persons without a previous COVID-19 diagnosis, hospitalization rates in California followed a similar pattern. These results demonstrate that vaccination protects against COVID-19 and related hospitalization, and that surviving a previous infection protects against a reinfection and related hospitalization.
Importantly, infection-derived protection was higher after the Delta variant became predominant, a time when vaccine-induced immunity for many persons declined because of immune evasion and immunologic waning.”
In another study,10 researchers reviewed studies published in PubMed and found that the risk of reinfection with SARS-CoV-2 decreased by 80.5% to 100% among people who had previously had COVID-19. Additional research cited in their review found:11
Among 9,119 people who had previously had COVID-19, only 0.7% became reinfected.
At the Cleveland Clinic in Cleveland, Ohio, the incidence rate of COVID-19 among those who had not previously been infected was 4.3 per 100 people; the COVID-19 incidence rate among those who had previously been infected was zero per 100 people.
The frequency of hospitalization due to a repeated COVID-19 infection was five per14,840 people, or .03%, according to an Austrian study; the frequency of death due to a repeated infection was one per 14,840 people, or .01%.
Given these findings, the researchers concluded that previous infection status should be documented and recovered patients counseled on their risk for reinfection. They stated:12
“Given the evidence of immunity from previous SARS-CoV-2 infection, however, policy makers should consider recovery from previous SARS-CoV-2 infection equal to immunity from vaccination for purposes related to entry to public events, businesses, and the workplace, or travel requirements.”
It’s Rare to Get Reinfected by SARS-CoV-2
In a letter to the editor of The New England Journal of Medicine, Dr. Roberto Bertollini of the Ministry of Public Health in Doha, Qatar, and colleagues estimated the efficacy of natural immunity against reinfection by comparing data in the national cohort.
They found that immunity acquired from previous infection was 92.3% effective against reinfection with the beta variant and 97.6% effective against reinfection with the alpha variant.13 Protection persisted even one year after the primary infection.
Researchers from Ireland14 also conducted a systematic review including 615,777 people who had recovered from COVID-19, with a maximum duration of follow-up of more than 10 months. “Reinfection was an uncommon event,” they noted, “… with no study reporting an increase in the risk of reinfection over time.” The absolute reinfection rate ranged from zero percent to 1.1%, while the median reinfection rate was just 0.27%.15,16,17
Another study revealed similarly reassuring results. It followed 43,044 SARS-CoV-2 antibody-positive people for up to 35 weeks, and only 0.7% were reinfected. When genome sequencing was applied to estimate population-level risk of reinfection, the risk was estimated at 0.1%.18
Again, there was no indication of waning immunity over seven months of follow-up, with the researchers concluding, “Reinfection is rare. Natural infection appears to elicit strong protection against reinfection with an efficacy >90% for at least seven months.”19
Another study from Israel also had researchers questioning “the need to vaccinate previously-infected individuals,” after their analysis showed similar risks of reinfection among those with vaccine-induced or natural immunity. Specifically, vaccination had an overall estimated efficacy of preventing reinfection of 92.8%, compared to 94.8% for natural immunity acquired via prior infection.20
Evidence from Washington University School of Medicine also shows long-lasting immunity to COVID-19 exists in those who’ve recovered from the natural infection.21 At both seven months and 11 months after infection, most of the participants had bone marrow plasma cells (BMPCs) that secreted antibodies specific for the spike protein encoded by SARS-CoV-2.
The BMPCs were found in amounts similar to those found in people who had been vaccinated against tetanus or diphtheria, which are considered to provide long-lasting immunity. “Overall, our data provide strong evidence that SARS-CoV-2 infection in humans robustly establishes the two arms of humoral immune memory: long-lived BMPCs and memory B cells,” the researchers noted.22
This is among the best available evidence of long-lasting immunity, because this immunological memory is a distinct part of the immune system that’s essential to long-term protection, beyond the initial immune response to the virus.23
Getting the Shot May Be Worse After Prior Infection
If you’ve had COVID-19, getting injected may pose an even greater risk, to the extent that Dr. Hooman Noorchashm, Ph.D., a cardiac surgeon and patient advocate, has repeatedly warned the FDA that “clear and present danger” exists for those who have had COVID-19 and subsequently get the injection.24
At issue are viral antigens that remain in your body after you are naturally infected. The immune response reactivated by the COVID-19 injection can trigger inflammation in tissues where the viral antigens are present. The inner lining of blood vessels, the lungs and the brain may be particularly at risk of such inflammation and damage.25 Writing in Lancet Infectious Diseases, researchers also explained:26
“Some people who have recovered from COVID-19 might not benefit from COVID-19 vaccination. In fact, one study found that previous COVID-19 was associated with increased adverse events following vaccination with the Comirnaty BNT162b2 mRNA vaccine (Pfizer–BioNTech). In addition, there are rare reports of serious adverse events following COVID-19 vaccination.”
As it stands, the U.S. CDC continues to push universal injections, despite past infection status, and natural immunity is not considered adequate to enter the growing number of venues requiring vaccine passports. This isn’t the case in Switzerland, where residents who have had COVID-19 in the past 12 months are considered to be equally as protected as those who’ve been injected.27
The end-goal of vaccine passports, though, isn’t to simply track one shot. Your entire identity, including your medical history, finances, sexual orientation and much more, could soon be stored in a mobile app that’s increasingly required to partake in society. While some might call this convenience, others would call it oppression.
You can fight back against vaccine mandates and their related vaccine passports by not supporting establishments that require proof of a shot or a negative test, and avoiding all digital identities and vaccine ID passports offered as a means of increasing “access” or “convenience.”28
The Canadian “Freedom Convoy” started pulling into Ottawa January 29, 2022, gathering in front of the Parliament building. They have vowed to stay put until the Canadian government agrees to roll back all federal mandates, including the vaccine mandate and the vaccine passport
Canadian Prime Minister Justin Trudeau has tried to downplay the protest, referring to it as a “small fringe minority” of people “who hold unacceptable views” and don’t represent the views of Canadians
As the convoy descended on Ottawa, Trudeau moved out of his residence and then claimed to have contracted COVID and that he would remain in isolation for a week
Inspired and encouraged by the Canadian trucker movement, truckers in other countries are now organizing their own Freedom Convoys. In Europe, a European Freedom Convoy will meet up in Brussels, February 14, 2022, and remain there “until vaccination passports and associated restrictions are abolished” across the European Union
Australia also organized a Freedom Convoy to gather outside the Parliament House in Canberra, starting January 31, 2022, and in the U.S., American truckers are planning a DC Freedom Convoy
Did you know there’s a massive trucker convoy protesting COVID jab mandates in Ottawa, Canada? You’re forgiven if you missed it, because this gigantic movement received very minimal coverage in the conventional press for the first week or so. Ditto for similar trucker protests forming in other countries, such as Australia and Germany.
The Canadian Freedom Convoy
The Canadian “Freedom Convoy” started pulling into Ottawa January 29, 2022, gathering in front of the Parliament building. According to The New York Times:1
“The convoy was organized in response to a regulation, implemented this month, that requires truckers returning from the United States to show proof of vaccination. But in recent days, it has broadened to include Canadians critical of pandemic restrictions in general, and of Prime Minister Justin Trudeau …
Private cars and pickup trucks greatly outnumbered the heavy trucks that made up the convoy in its first days. Throughout Saturday, the vehicles clogged the streets in and around Parliament, most of them bearing flags or signs denouncing public health measures related to the pandemic.
Thousands of protesters on foot, many carrying handmade signs on hockey sticks, wandered through the parked vehicles and the slow-moving traffic or gathered on the lawn in front of Parliament … Few people appeared to be following Ontario’s rules requiring social distancing and masks at crowded, outdoor gatherings …
Several Canadian news outlets reported that Mr. Trudeau and his family had been moved out of their official residence by the Royal Canadian Mounted Police as a precaution.”
Trudeau Shows His True Colors
Canadian Prime Minister Justin Trudeau initially tried to downplay the protest, referring to it as a “small fringe minority” of people “who hold unacceptable views” and don’t represent the views of Canadians. It boggles the mind to think how rapidly our countries have spiraled into authoritarianism where the very idea of freedom is now “unacceptable.”
We can’t be surprised, however. It’s no secret that the World Economic Forum, which is leading the technocratic takeover of the whole world, has penetrated the cabinet of Trudeau and many other countries. WEF head and founder Klaus Schwab admitted it in 2017.2
Once this “fringe minority” descended on Ottawa, however, Trudeau ran. Not only was he escorted out of his official residence, as reported by The New York Times, he’s also said to have tested positive for COVID and will be in isolation for a week.3
Countless videos illustrate just how out of touch Trudeau’s comments are, and that’s putting it kindly. Along highways and overpasses, in the city and outside of it, Canadians have gathered in astounding numbers to cheer the truckers on, everywhere thanking them for taking up this peaceful fight for freedom.
While the actual number of trucks involved is still unknown, it seems reasonable to assume it’s in the thousands. According to Local 12 News,4 the convoy could be a “world-record setter” in terms of its size — an estimated 70 kilometers or some 43.5 miles.
The truckers have vowed to stay put until the Canadian government agrees to roll back all federal mandates, including the vaccine mandate and the vaccine passport.5
Covert Surveillance Is Here
In the video above, Jimmy Dore plays an interview with Benjamin Dichter, one of the organizers of the Freedom Convoy, who describes how Canada has already rolled out previously unknown technology that scans and reads a trucker’s passport and vaccine status on approach, without them actually having to show any papers or display their vaccine QR code on their phone.
Their cell phones pop up automatically on the border agent’s screen as they approach the station, and the cell phone is automatically linked to the driver’s passport and vaccine card, which are also displayed automatically.
So much for right to medical privacy! The secret surveillance and tracking we’ve been warning about is here, or at the least at the Canadian border. The question is, where else it might be deployed without our knowledge?
Google Runs Is Part and Parcel of the Surveillance State
For years, I’ve warned people about the creeping surveillance state, of which Google is a significant part. If you still haven’t ditched Google products from your life (which include Android), now’s a good time to start. In early 2020, I interviewed Robert Epstein, Ph.D., who for the last decade has helped expose Google’s manipulative and deceptive practices. As noted by Epstein, Google’s powers pose three very specific threats to society:
1. They’re a surveillance agency with significant yet hidden surveillance powers — The Google search engine, Google Wallet, Google Docs, Google Drive, Gmail, Google Chrome browser, YouTube, Android phones, Google home devices like Nest and Google wearables like Fitbit are all surveillance platforms that work together.
Android cell phones, for example, which are a Google-owned operating system, can track you even when you’re not connected to the internet, whether you have geo tracking enabled or not, and even if your phone is turned off.
As soon as you reconnect to the internet, all that information stored in your phone is sent to Google. So, even though you may think you’ve just spent the day incognito, the moment you reconnect, every step you’ve made is shared (provided you had your phone with you).
Google is also tracking your movements online even if you’re not using their products, because most websites use Google Analytics, which tracks everything you do on a website. And, you have no way of knowing whether a website uses Google Analytics or not. The only way to protect yourself against this would be to use a VPN.
2. They’re a censoring agency — Google has a unique ability to restrict or block access to websites across the internet, thus deciding what people can and cannot see. They even have the ability to block access to entire countries and the internet as a whole.
The most crushing problem with this kind of internet censorship is that you don’t know what you don’t know. If a certain type of information is removed from your search, and you don’t know it should exist somewhere, you’ll never go looking for it. And, when searching for information online, how would you know that certain websites or pages have been removed from the search results in the first place? The answer is, you don’t.
For example, Google has been investing in DNA repositories for quite a long time, and are adding DNA information to our profiles. According to Epstein, Google has taken over the national DNA repository, but articles about that — which he has cited in his own writings — have all vanished.
3. They have the power to manipulate public opinion through search rankings and other means — In so doing, they have the ability to shape the opinions, beliefs, thoughts, attitudes, purchases, behavior and votes of billions of people, all without anyone realizing they’re being manipulated. They don’t even leave a paper trail for authorities to trace. As noted by Epstein:
“They’re using new techniques of manipulation that have never existed before in human history and they are for the most part, subliminal … but they don’t produce tiny shifts. They produce enormous shifts in people’s thinking, very rapidly. Some of the techniques I’ve discovered are among the largest behavioral effects ever discovered in the behavioral sciences.”
In his article6 “Seven Simple Steps Toward Online Privacy,” Epstein outlines his recommendations for protecting your privacy while surfing the web, most of which don’t cost anything.
Vaxxed or Unvaxxed — People Want Freedom
Now, don’t get me wrong, I love Jimmy Dore as we both grew up in a poor neighborhood in Chicago and I love his humor. But for the record, while Dore tells his audience that the COVID jab will protect you from severe illness and death, I disagree. Mounting evidence suggests it might actually destroy your natural immune function, especially after the third dose.
Be that as it may, Dore rightfully states that being against mandates and vaccine passports isn’t a cause restricted to the unvaccinated. He, Dichter and countless others who have received the jab did so because they wanted to protect themselves, but they’re not willing to give up their freedoms and live in a totalitarian state.
A Political Tsunami
The good news is that, for whatever reason, the Canadian Freedom Convoy has captured the attention and hearts of the global population — even with mainstream media ignoring and/or minimizing it for days. As noted by Ron Paul in the Liberty Report above, it’s turning into “a political tsunami.”
Truck driver is one of the most common jobs in North America, and perhaps around the world, which might explain the wide appeal of this movement, and how news of it spread so rapidly and organically despite media blackouts and social media censorship. Another reason is probably because people recognize the leverage truckers as a group have.
For example, nearly 70% of all goods freight transported annually in the U.S. are delivered by truck.7In Canada, that percentage is closer to 90%.8 When thousands of truck drivers stop delivering goods and instead honk their air horns outside a government building, the effects are bound to rapidly become noticeable in the form of empty shelves.
Anyone tired of living in Orwellian dystopia recognizes that this kind of leverage over the political class is far more significant than people marching in the streets with signs — which is what Europeans have been doing every weekend for months on end, to no avail.
The Rise of Global Freedom Convoys
Inspired and encouraged by the Canadian trucker movement, truckers in other countries are now organizing their own Freedom Convoys.9 In Europe, a European Freedom Convoy will meet up in Brussels, February 14, 2022, and remain there “until vaccination passports and associated restrictions are abolished” across the European Union.10,11
Australia also rapidly started organizing a Freedom Convoy to gather outside the Parliament House in Canberra, starting January 31, 2022.12,13 Within days, the Official Convoy to Canberra Facebook page had gathered 170,400 members.14 Facebook has now removed the group.
In the U.S., American truckers are planning a DC Freedom Convoy. Facebook was quick in deleting their page, though — a move its organizers blasted as “Censorship at its finest.” As reported by Fox News:15
“The group, titled ‘Convoy to D.C. 2022,’ acted as a place for truckers to plan and coordinate their trek from California to Washington, D.C. Jeremy Johnson, who set up the Facebook group, said his personal account was also removed, prompting him to contact a civil rights attorney to discuss the next steps …
[Mike] Landis, a trucker involved in the freedom convoy, told host Carley Shimkus that this movement is ‘a long time coming.’ He said Americans are tired of the ‘government overreach’ and criticized politicians for, as he believes, not following the Constitution.
‘The presence of that amount of people that show that they are unhappy with what’s going on is a good way to hopefully get their attention,’ he said. Johnson and Brase anticipate a wide range of Americans, not only truckers, will come out to support their cause.
‘This crosses all genders, all races, all sexual orientations, all occupations,’ Brase said. ‘Truckers might be standing up, but it’s not about the truckers. It’s about America.’ The group’s goal is to end vaccine mandates through peaceful protests. ‘The government needs to really take a look at what the American people want,’ Johnson said. ‘And they don’t want mandates.'”
(Natural News) The Canadian truckers and freedom protesters deserve huge credit for bringing humanity to a tipping point against tyranny. Thanks to the courage, determination and dedication to peace that’s demonstrated by Canada’s protesters, humanity is withdrawing its consent from government tyrants all over the world.
Globalism is crashing, and centralization of power is being ripped to shreds. The entire model of globalism is dead, and no human being that’s aware and alive right now wants to return to a society structured as a top-down, totalitarian, centralized control system of global enslavement run by a few hundred hyper-wealthy freakazoids like Zuckerberg and Gates.
What I’m trying to explain here is that this is about much more than covid vaccines or lockdowns. This is about humanity rising up against the very idea of centralized government, corporations, media and tech giants. The era of centralization has come to an end, and the free people of the world have begun the process of dismantling it by simply withdrawing their consent.
Consider the impact of the realizations now spreading across the world:
Government failed the people.
Corporations murdered people for profit.
Doctors, hospitals and the medical system betrayed the people.
Big Tech platforms silenced the truth, costing millions of lives.
Big Media was complicit in the plandemic and the vaccine biowar against humanity.
The institution of science deceived the people and proved it is hopelessly corrupt and evil.
What we’ve all lived through over the last two years is corrupt, deceptive, anti-human institutions waging war against truth and humanity, showing their true cards and exposing the depth of their evil.
And that’s why the people of the world are now peacefully rising up and demanding an end to the entire centralization structure of globalism. It is the centralized control over media, information, government and “science” that brought us all to the brink of destruction. Absolute power corrupts absolutely, and for the past several generations, the people have handed over far too much power to governments, science journals, media giants and tech platforms.
Now, the people are taking their power back.
And they’re doing it, ironically, by mimicking the mRNA spike protein blood clots in the real world: Clogging bridges, roadways and cities, bringing society to a standstill with nothing but trucks, horns and raw courage.
The message is clear: You try to put clots into our blood and we’ll put traffic clots across your cities.
The evil governments, predictably, call these peaceful protesters “terrorists” — even as the governments themselves are carrying out acts of terrorism and mass murder against their own people. So let’s take a look at some of the very real people behind the Ottawa protests. The masterful portrait photos shown here are from Dan Aponte, a Canadian photographer who brilliantly captures the humanity of the freedom protesters in Ottawa. This is flat-out the most impactful photography I’ve seen in years. Read more details about these truckers and peaceful protesters at:
Brock Hobb:
Katie Hepburn:
Nabil Yaghi:
Odia Jean Pierre:
Randy:
Sebastian Fortin:
From Bari Weiss at Substack.com:
The solidarity was infectious. There were copycat protests popping up in Helsinki, Finland, and Wellington, New Zealand and Nice, France (they planned to hit Paris and Brussels). There were truckers organizing in the Netherlands, Australia and the United States. Among the Americans who had driven up to Ottawa there was talk that soon the big rigs would descend on Washington, D.C.
“Seeing the country fall apart like this is heartbreaking,” Sim said. “For me, this is the line in the sand. If we lose this battle, I’d like to move out of Canada.” He said that he was thinking of maybe heading to Florida. A lot of the truckers were thinking about the States. But not yet. “I feel that I owe it to me and others that share my values to, at least, fight for this.”
Learn more about how humanity defeats globalism and centralization, dismantling the whole damned system
Today’s Situation Update podcast covers all this in more detail. Definitely hear the last 30 minutes of the podcast for an inspiring analysis of why we’re all here right now in this pivotal time of human history:
Find more information-packaged podcasts each day, along with special reports and emergency updates, at:
Johnson & Johnson temporarily halted production of its COVID-19 vaccine in The Netherlands, the only manufacturing hub making usable doses for the pharmaceutical company, according to a New York Times report on Tuesday.
The company stopped production of the vaccine at its facility in the Dutch city of Leiden at the end of 2021 and has instead turned its attention to making another vaccine for an unrelated virus, The Times reported. The pause is temporary and expected to last just a month — but it could reduce Johnson and Johnson’s vaccine supply by a few hundred million doses.
While the Johnson & Johnson vaccine from Janssen Pharmaceuticals has been linked to rare blood clots and is considered less effective than Pfizer and Moderna‘s shots by the Centers for Disease Control and Prevention, the vaccines are extremely important in Africa and other low-income countries, which rely on the simpler one-dose shot.
Novavax Inc (NVAX.O) said on Monday U.S. government funding for its COVID-19 vaccine had been expanded to cover a late-stage study in adolescents with a booster component.
Novavax in July 2020 had received $1.6 billion in funding to develop its protein-based vaccine under a government program aimed at accelerating access to coronavirus vaccines and treatments, formerly called Operation Warp Speed.
Novavax’s two-dose shot has received authorizations from the European Union and the World Health Organization and was recently cleared for use in adults in Britain and New Zealand. Novavax last year started testing its vaccine in adolescents aged 12 to 17.
A group of young children in Ireland experienced no major reactions after mistakenly being given adult-sized shots of Pfizer‘s COVID-19 vaccine.
The mistake was noticed by staff at a mass vaccination center where the children came for the second dose of Pfizer‘s two-shot vaccine, the Irish Examiner reported Monday. Only one of the seven children had a mild adverse effect, the paper reports, citing regulators.
Children are supposed to be given a 10-milligram dose of Pfizer’s vaccine, known as Comirnaty, according to Health Service Executive’s National Immunization Office. For adults, the dose is 30 milligrams.
It’s not the first time health workers have confused doses. Kaiser Permanente warned in January that nearly 4,000 patients had received an insufficient dose of the vaccine.
Pfizer made nearly $37 billion (£27bn) in sales from its COVID-19 vaccine last year — making it one of the most lucrative products in history — and has forecast another bumper year in 2022, with a big boost coming from its COVID-19 pill Paxlovid.
The U.S. drugmaker’s overall revenues in 2021 doubled to $81.3 billion, and it expects to make record revenues of $98 billion to $102 billion this year.
The bumper sales prompted accusations from campaigners of “pandemic profiteering”. The group Global Justice Now said the annual revenue of $81 billion was more than the GDP of most countries and accused Pfizer of “ripping off public health systems”.
The European Union’s drug regulator launched a review to evaluate whether the Pfizer/BioNTech (PFE.N), (22UAy.DE) COVID-19 vaccine can be used as a third booster shot in adolescents aged 12 to 15, even after several countries in the region have already started such a campaign.
In its statement on Tuesday, the European Medicines Agency added that a review of booster shots given to 16- and 17-year-old teenagers was ongoing.
Germany’s vaccine committee last month recommended that all children between the ages of 12 and 17 receive a booster, following the initial two-shot course, as infection rates continue to soar among youngsters in particular. Other states in the region followed suit.
Pediatric mental health visits to physicians increased during the first year of the COVID-19 pandemic in Ontario, Canada, according to a population-wide study.
Starting in July 2020, rates of visits to mental health services were consistently 6% to 15% above expected levels — based on prior years — and were sustained as of February 2021 (adjusted relative rate [aRR] 1.15, 95% CI 1.13-1.17), reported Natasha Ruth Saunders, MD, MSc, of the Hospital for Sick Children in Toronto, and colleagues.
The largest increase in physician-based mental health visits was recorded for adolescent girls (aRR 1.26, 95% CI 1.25-1.28), they noted in JAMA Pediatrics.
Just 10% of Americans now expect that COVID-19 will be eradicated by this time next year, according to a new poll released Tuesday by Axios-Ipsos.
One in 3 survey takers said they expect to catch COVID-19 within the next month as the results show an American public that is starting to process the concept of living with the coronavirus. The poll does show that Americans are divided on how to live with COVID-19.
Axios reports that there are four fairly evenly split groups on how to go forward with the virus: open up and end all restrictions, open up with precautions, keep precautions and requirements in place, and increase mask and vaccine requirements.
A sub-variant of the Omicron variant of COVID is spreading rapidly in Europe and Asia and could become the dominant variant of the virus. The so-called “stealth” Omicron COVID sub-variant BA.2 has now been found in 67 countries.
Speaking to The Jerusalem Post, Dr. Dorit Nitzan, regional director for the World Health Organization (WHO), said that the expected trajectory of BA.2 will see the sub-variant become the new dominant variant of COVID once it passes a certain threshold as is being seen in Denmark and the U.K.
Research Director, Co-Director of the MPH Global Health Epidemiology Program CE, and an epidemiologist in Copenhagen, Lone Simonsen, told Newsweek: “BA.2 is already dominant in Denmark, but we see no rise in severe illness and ICU admissions are dropping. My take is BA.2 is a faster but not more deadly variant.”
Pet hamsters can transmit COVID to humans and are the likely source of a recent outbreak of the Delta variant in Hong Kong, data suggests.
The research confirms fears that a pet shop was the source of a recent COVID outbreak in the city, which has seen at least 50 people infected and led to the culling of more than 2,200 hamsters.
However, virologists emphasized that, although the pet trade could provide a route for viral spread, existing pet hamsters are unlikely to pose a threat to their owners and should not be harmed.
In the wake of the FDA being forced to release massive amounts of data on Pfizer’s mRNA COVID shot clinical trials, the drug company has revised its fourth quarter investors report to reflect concerns about that data.
Quite noticeably, Pfizer’s now tempering their previously glowing predictions of $54 billion in sales in 2022 with new disclosures of unfavorable safety data that may come to light under audits or inspections. As noted by Twitter posts and ZeroHedge, some of the notations are buried “deep in its business risk disclosures.”
At the same time, Pfizer is also acknowledging to investors that the pandemic may “diminish in severity or prevalence, or disappear entirely.”
More than 10,000 Americans have reported tinnitus as a possible side effect of the COVID-19 jab, and some are now questioning why the FDA and CDC are not taking a deeper look into their claims about hearing problems.
The problem is, no matter how many people report the side effects — which one man said rendered him nearly deaf — they are being told this is not a side effect of the shots. The victims, however, just want answers.
In a ground-breaking story for mainstream media, Minnesota’s StarTribune suggests that the state’s political leaders “could — and should — join the call” to reevaluate the value of using convalescent plasma to treat COVID patients.
The plasma, donated by persons who have recovered from a COVID-19 infection, is a therapy that not only is natural, but could be given promptly to patients to lower the possibility of a hospital admission, the paper said:
“Convalescent plasma has a long history helping combat disease. Before there were antibiotics and antivirals, physicians recognized that recovering patients could help others from becoming seriously ill. The reason: the antibodies they naturally manufactured.
Blood donated by these patients can be ‘processed to remove blood cells, leaving behind liquid (plasma) and antibodies,’ according to the Mayo Clinic. The antibodies can then be infused into the newly ill. It’s like having a seasoned platoon show up to assist immune system soldiers.”
Mass formation involves the formation of a hypnotic state around a shared consensus
Those under its spell obsessively focus on a failure of the normal world or a particular event or person, who becomes the focus of the attention and can effectively control the masses
Mass formation can occur in a society with feelings of social isolation and free-floating anxiety among a large number of people; it leads to totalitarian thinking and, eventually, to totalitarian states
After Dr. Robert Malone mentioned mass formation on an episode of The Joe Rogan Experience, the term went viral
The technocrats quickly took action, manipulating search results and populating Google with propaganda to discredit Malone and the mass formation psychosis theory
At the end of 2021, the term “mass formation psychosis” had a value of 0 on Google Trends, meaning there’s not enough data for the term to even make it on the charts. Then, on December 31, Dr. Robert Malone, the inventor of the mRNA and DNA vaccine core platform technology,1 mentioned it on an episode of The Joe Rogan Experience viewed by more than 50 million people.2
The term, which provides a coherent explanation of why so many people have fallen victim to the unbelievable lies and propaganda of the mainstream COVID-19 narrative, went viral. On January 2, 2022, mass formation psychosis reached a value of 100 on Google Trends,3 which means it had reached peak popularity.
Google Manipulates Reality Around ‘Mass Formation Psychosis’
The technocrats quickly took action, adding a rarely seen warning that popped up for those searching the suddenly popular phrase in the early days of 2022. It read, “It looks like these results are changing quickly. If this topic is new, it can sometimes take time for results to be added by reliable sources.”4
In reality, the topic is not new. Mattias Desmet, professor of clinical psychology at the University of Ghent in Belgium, who has 126 publications to his name,5 has been studying it for many years, and the phenomenon actually dates back over a hundred years. One of the earliest works on the subject, according to Malone, is an 1841 book titled, “Extraordinary Popular Delusions and The Madness of Crowds,” which details “the irrational behaviors of crowds.”6
You won’t find any of this — at least not easily — if you search on Google for “mass formation psychosis” today, however, as it’s all been effectively buried by Big Tech. What you will find is the results of an orchestrated and carefully vetted links to sites that help control the mainstream narrative around the topic. This not only serves to twist the meaning of the term but also to discredit Malone, a classic Orwellian Doublespeak move.
The top search results include headlines like “An anti-vaxx scientist said ‘mass formation psychosis’ caused people to follow COVID-19 measures. Psychologists say there’s no such thing,” (Business Insider7) and “Fact Check-No evidence of pandemic ‘mass formation psychosis’, say experts speaking to Reuters” (Reuters8). Rogan’s interview with Malone was also taken down by YouTube.
Outrageously, one of the “expert fact checkers” used by the AP to discredit Malone and mass formation psychosis is Jay Van Bavel, a New York University assistant professor of psychology and neural science who not only stated he had never heard of the phrase and could not find it in peer-reviewed literature, but also has encouraged the use of “behavioral science” to “nudge” and “motivate” people to obey the official COVID-19 narrative.9 On January 10, Malone wrote:10
“[T]here has been an amazingly coordinated effort to shoot the messenger and actively character assassinate (or “defenstrate”) me as a surrogate while avoiding any reference to the highly credentialed academic Professor Dr. Mattias Desmet who actually developed the theory and has documented the extensive evidence in an upcoming academic book.
… In this coordinated propaganda and censorship response, we can clearly see the hands of the BBC-led Trusted News Initiative, the Scientific Technological Elite, the transnational investment funds and their World Economic Forum allies which control Pfizer and most of Big Pharma, Legacy Media and Big Tech (and many national governments) acting in real time to suppress a growing awareness by the general public of having been actively manipulated using crowd psychology tools to generate clinically significant fear and anxiety of COVID-19 (otherwise known as “Coronaphobia”) to advance their agendas on a global scale.”
What Is Mass Formation Psychosis?
In the video above, you can see Thomas Patrick Carrigan interview Malone, Desmet and board-certified internist and cardiologist Dr. Peter McCullough about mass formation psychosis. Don’t be confused by the term mass, it is just psychological speak for crowd. Crowd formation is the same as mass formation.
Formation is the sudden cohesion of the group (the crowd) around a shared consensus. Desmet says he prefers the term mass formation — not mass formation psychosis — because he doesn’t want to use a diagnostic term and the word “psychosis” has a stigma and medical meaning attached to it. Either way, both terms have the same meaning, which involves the formation of a hypnotic state.
Desmet’s upcoming book, “The Psychology of Totalitarianism,” explains that mass formation has grown over the last 200 years. On a grand scale, mass formation leads to totalitarian thinking and, eventually, to totalitarian states. He details the four conditions needed to achieve mass formation on a large scale, which include cognitive dissonance and psychological pain — factors that often leave people desperate for change and a way to escape:11
Feelings of social isolation and being alone among a large number of people
Feelings that your life is pointless and meaningless
High levels of free-floating anxiety
High levels of free-floating frustration and aggression
According to an abridged excerpt from Desmet’s book:12
“If under these conditions a narrative is distributed through the mass media which indicates an object of anxiety and provides a strategy to deal with this object of anxiety, then all the free floating anxiety might be associated to this object and a huge willingness might be observed to participate in the strategy to deal with the object of anxiety.
At the same time, the field of attention gets narrower until it only contains the part of reality that is indicated by the narrative and people lose their capacity to take into account the other aspects of reality (what makes them often utterly irrational).”
The More Absurd It Gets, the More Successful It Will Be
People want to remove their feelings of social isolation and anxiety. Toward that end, mass formation involves obsessive focusing on a failure of the normal world or a particular event or person, who becomes the focus of the attention — and the more absurd the narrative becomes, the better. Desmet says in the video above:13
“The narrative that leads to the mass formation typically becomes more and more absurd, and the strange thing is that people don’t seem to notice this … The reason why people buy into the narrative is not, in the first place, because the narrative is correct or scientific or accurate.
The reason why people buy into the narrative is because it creates this new social bond. That’s why typically during mass formation, the people who don’t want to conform to the masses, who don’t go along with the narrative, are typically [accused of] lacking citizenship and solidarity.”
Desmet says that the more absurd the narrative and its surrounding measures become, the more successful they will be for a certain part of the population, usually about 30%, because the measures function as rituals, through which an individual shows that they are less important than the collective masses:14
“A ritual is a kind of behavior that is without pragmatic meaning or sense, which is a symbolic kind of behavior through which an individual shows that it belongs to a collective and that it wants to sacrifice something of itself, which is important, in favor of the collective.”
Another irony is that the higher the level of education, the more susceptible people usually are to mass formation, Desmet says. “The people who try to get advanced degrees are usually people who think that social status is very important. And that could be the reason they are inclined to conform with the mainstream narrative.”15 It may also explain why so many physicians and academics have bought into the propaganda, ignoring science in favor of the collective narrative.
Fanaticism Allows for Lies, Manipulation
Those who are under the spell of mass formation psychosis are so convinced that their narrative will save the world that they feel justified in using manipulative tactics and lies to protect it, Desmet explains, exemplifying Plato’s noble lie — the notion that, in the case of high-status individuals or designated public leaders, it’s acceptable to lie if the lie is made in the interest of the common good. According to Desmet:16
“Once you understand the nature of mass formation, you also understand what you can do about it. But that doesn’t mean that it is easy to do something about it. The process of mass formation is a kind of hypnosis. Most scholars agree that it is very hard to wake people up from such a state of mass formation. Mass formation is a phenomenon that’s provoked by a voice.
It’s the voice of a leader, the voice that is distributed time and time again through the mass media, that keeps people in the grasp of mass formation, and the leader himself is also grasped in this process of mass formation … both the hypnotist and the hypnotized are into the process.”
Who’s the leader today? “The experts. The authority and the technocrats you could say,” Desmet says. The way out involves having the courage to speak the truth, even though doing so is typically extremely dangerous.
The ancient Greeks had a word for this — parrhesia, which is having the courage to speak the truth in spite of danger. But as Desmet explains, while those who try to reveal knowledge that is in conflict with the narrative put themselves at risk, if no one speaks the truth, society cannot continue to function.
Four Steps to End Mass Formation Psychosis
The first step to ending mass formation, which is also the most important, is speaking out against the official narrative if things seem off to you. “If you want to make the mass formation less deep, then it is quintessential that there are people who continue to speak out and [are a] dissonant voice in society, because this will disrupt the process of mass formation,” says Desmet.17
The second step involves connecting with other people in the real world who have a similar viewpoint as you or a feeling that something is wrong. Forming small networks in your community will help you break the mass formation cycle. It’s important, however that when you speak to people about the truth that you don’t try to take them back to the “old normal,” because, remember, this is what drove them to mass formation in the first place. According to Desmet:18
“If we try to convince people or bring a different narrative, [it’s important] that we do not try to convince people to go back to the old normal, because the old normal, that’s what people tried to escape through the process of mass formation. It was exactly because the old normal was unbearable that people were sensitive to the process of mass formation.
What we should try to construct together is a new normal, which is not a technocratic or transhumanist new normal. We should show people that there are other options. There are other options to escape the old normal.”
In short, Desmet recommends the following four steps to break free from mass formation psychosis and enact favorable change one social circle at a time:
Continue to speak out
Seek to connect with others of like mind
Construct a narrative together of a new normal — not to be confused with the “new normal” the transhumanist, technocratic movements are trying to advance — showing people that there are other options to escape the old normal
Always stick to the principles of nonviolent resistance
The last step is an important one, because if you use aggression of any form, even in the way you speak, it will only be used as justification by the masses that they were right to oppose you. Nonviolent resistant is the most efficient strategy as you try to resist and defy the mass formation psychosis around you.
How to Reverse Mass Formation Psychosis
While I deeply appreciate Desmet’s and Malone’s description of how the cabal has been able to fool most of the population, this is the best description of how they pulled all the brainwashing and the solution of how to avoid it right out of the matrix.
We all have the capacity to generate reality with our minds and this is what the cabal has hijacked so effectively. Why? Because never in the history of mankind have the tools existed to pull it off. First radio and then TV spread the message, but then social media leveraged the effectiveness of the brainwashing exponentially.
I would recommend watching this video a few times and sharing it with your friends, as it will help them understand — how we can repair the damage. We need to free our mind from their hijacking and use it for constructive purposes — not destructive ones.
Probiotics reduced muscle fatigue and brain fog, two symptoms of long COVID, after only 14 days; this may have a significant impact on the nearly 12 million people who experience long COVID symptoms
Poor gut microbiome diversity also predicts greater severity of COVID-19; some health experts recommend postbiotics in the prevention and treatment of COVID
Your gut health affects your neurological health; a poor gut microbiome can increase the risk of gut permeability, Alzheimer’s and other dementias
Factors that affect the health of your gut microbiome include artificial sweeteners, sleep, exposure to sunlight and the types of foods you eat
As reported in this short news clip, research evidence1 shows that probiotics may help reduce long-haul symptoms after COVID-19. Some people experience symptoms for weeks or months after a COVID-19 infection has resolved. When these symptoms persist for four weeks or more, they are known as long COVID, long-haul COVID, chronic COVID or long-haul syndrome.
Many of the symptoms of long COVID can also mirror those that are caused by the COVID-19 genetic therapy injections. Although anyone can experience symptoms of long COVID, it is more frequently seen in people who have been sick enough to be hospitalized or in the ICU.
According to Dr. Peter McCullough, board-certified internist and cardiologist, 50% of those who have been sick enough to be hospitalized will have symptoms of long COVID:2
“So, the sicker someone is, and the longer the duration of COVID, the more likely they are to have long COVID syndrome. That’s the reason why we like early treatment. We shorten the duration of symptoms and there’s less of a chance for long COVID syndrome.”
Symptoms of long COVID include fatigue, shortness of breath, coughing, chest pain, joint pain, memory problems, loss of taste or smell and muscle pain or headache.3 The symptoms are the result of damage to the lungs, immune system, mitochondria, heart and nervous system. McCullough goes on to explain that after a severe case of COVID-19, blood clots and heart problems can happen for up to 90 days or more.
Inflammation to the lining of the heart — pericarditis — and around the lining of the lungs — pleuritis — can also occur in long COVID. Data from a study4 published in November 2021 show the administration of probiotics can affect the gut microbiome, and subsequently help your body heal from the symptoms of long COVID.
Data Show Probiotics Help Long-Haul COVID Symptoms
Roughly 12 million people may suffer from long COVID symptoms, which a Swedish study found could potentially be alleviated after 14 days of probiotics.5 The study was published September 2021 in the journal Medicines.6 The researchers wanted to evaluate how effective probiotics might be in alleviating two of the symptoms of long COVID — muscle soreness and brain fog.
They enrolled 200 patients who had complaints of muscle fatigue after COVID. One hundred participants received a placebo and 100 received a combination of ImmunoSEB (systemic enzyme complex) and ProbioSEB CSC3 (probiotic complex). The participants were tested at different time points from Day 1 to Day 14.
The data showed that those treated with the supplements had 91% resolution of muscle fatigue by Day 14. There was also a greater reduction in mental fatigue scores as compared to those receiving the placebo. The researchers concluded:7
“This study demonstrates that a 14 days supplementation of ImmunoSEB + ProbioSEB CSC3 resolves post-COVID-19 fatigue and can improve patients’ functional status and quality of life.”
ABC News interviewed public health medical educator Dr. Shad Marvasti, who recommends using probiotic supplements with at least 10 strains of active cultures to help support the immune system.8 He noted fermented foods such as sauerkraut, miso, kimchi and tempeh would help populate your gut microbiome.
He also mentions yogurt. However, I recommend that if you do use yogurt, it’s homemade since the products sold in the grocery store are high in sugar, which is a nutrient that feeds harmful bacteria in the gut. Also, if you decide to eat fermented soy, to be sure it’s grown organically, as most soy in the U.S. is a GMO food that is contaminated with pesticides and herbicides.
During data-gathering for the research, the scientists found other coronavirus infections, such as SARS, also triggered long-term symptoms. During follow-up, data showed 64% reported muscle fatigue at three months, 54% at six months and muscle fatigue at 12 months in 60% of those surveyed.9 Likewise, after the Middle East Respiratory Syndrome (MERS), 48% reported fatigue after 12 months.
The researchers believe that the supplement regimen used on the participants reduced physical and mental fatigue and would be an effective early intervention. They suggest that while scientists continue to characterize long haul syndrome, these dietary supplements are added to clinical recommendations to help improve functional status and quality of life.10
Poor Gut Health May Predict Severe COVID
In an unrelated study published in 2018, researchers performed a systematic review of 70 randomized placebo-controlled trials11 to evaluate how specific probiotics may benefit individuals who had irritable bowel syndrome or other gastrointestinal (GI) disturbances. The data from the review indicated that there were specific probiotics with beneficial effects on lower GI health conditions, such as irritable bowel syndrome.
Knowledge that probiotics offer a distinct advantage to the immune system has prompted study into the relationship between gut health and COVID outcomes. The featured study was published in the same month and year as another paper12 that proposed the use of postbiotics in the treatment of post-COVID long-haul symptoms.
The writers advocate postbiotics that may help alleviate the burden on the body from viral infections and they postulate there may be a role for “precision postbiotics” in preventive interventions. Postbiotic is an umbrella term for components of microbial fermentation.13 This can include short-chain fatty acids, functional proteins, metabolites and extracellular polysaccharides.
Since the start of the pandemic, several studies have shown that patients with GI symptoms often have more severe disease. One review of more than 1,000 patient records was presented to the American College of Gastroenterology.14 The data showed those who presented at admission with GI symptoms and suspected COVID-19 infection had worse outcomes than those who did not have GI symptoms.
After adjusting for comorbidities, demographics and other clinical symptoms, of 1,000 patients, 22.4% had at least one GI symptom, the most common of which was nausea and vomiting. Researchers also found those who had GI symptoms had a higher body mass index, a higher prevalence of diabetes and high blood pressure, and were older.
While this group had a higher rate of ICU admission and intubation, the study did not include mortality rates in the analysis. However, SciTech Daily15 reported that autopsy results and studies have suggested a sizable number of people with severe COVID-19 also have GI problems. A significant number of people with respiratory problems also had GI symptoms, suggesting that when the virus affects the GI tract, it can increase the severity of the illness.
Another paper16 published in January 2021 suggested the GI symptoms that predict severe COVID-19 are triggered by poor gut health. The writer, Heenam Stanley Kim, Ph.D., from Korea University, proposes that gut dysbiosis can exacerbate the severity of the infection.
This hypothesis is supported by a review of several studies since the start of the pandemic, which also demonstrated an association between severe disease and a lack of microbial diversity.17 An early study of patients admitted from March 4, 2020, to March 24, 2020, showed 31.9% had GI symptoms on admission.18
Your Gut Affects Brain Health and Immunity
Your gut health plays an important role in your neurological health and with your immune system. A very large part of your immune system sits in your gut microbiome and GI tract. Researchers estimate that up to 80% of your immune cells can be found in the gut.19
The complex interaction between your gut microbiome, pathogens and your immune system is affected by several factors, including your nutrition. One review of the research20 published in 2021 identified the significance that nutrition plays in both prevention and treatment of infectious disease.
There are also deep connections that exist between your gut and your brain. Harvard Health21 explains that these two structures are linked through biochemical signaling. The primary connection is the vagus nerve, which is the longest nerve in the body.
For example, when the fight-or-flight response is triggered, warning signals are sent to the gut. This is why digestive problems can be triggered by a stressful event. On the other hand, digestive issues like irritable bowel syndrome or chronic constipation can trigger anxiety or depression.
Alzheimer’s disease continues to be a leading cause of death in the U.S., with 1 in 3 seniors dying with Alzheimer’s or dementia — more than the number killed by breast and prostate cancers combined.22
One team of Swiss and Italian researchers found a connection between imbalanced gut microbiota and the development of amyloid plaques in the brain, associated with Alzheimer’s disease.23 In a prior study24 the team had found that the gut microbiota in people with Alzheimer’s disease is different from those without the condition; microbial diversity is reduced, and certain bacteria are overrepresented.
In their current study, the researchers engaged 89 people aged 65 to 85 years. Some were diagnosed with Alzheimer’s disease or other neurodegenerative diseases and the others were healthy with no memory problems. The researchers used PET imaging to measure amyloid deposits in the brain and measure the serum markers of inflammation and proteins produced by intestinal bacteria.
“Our results are indisputable: Certain bacterial products of the intestinal microbiota are correlated with the quantity of amyloid plaques in the brain,” explained Moira Marizzoni, one study author with the Fatebenefratelli Center in Brescia, Italy.25
The Effects of Artificial Sweeteners, Sleep and Sunlight
Several factors influence your gut microbiome. One factor found in many processed foods that has a devastating effect on your gut microbiome is artificial sweeteners. As early as 2008,26 scientists had discovered that sucralose lowered your gut bacteria count by 47.4% to 79.7% and increased the pH level of your intestines.
More recently, scientists found that three of the most popular artificial sweeteners — sucralose (Splenda), aspartame (NutraSweet, Equal and Sugar Twin) and saccharin (Sweet’n Low, Necta Sweet and Sweet Twin) — have a pathogenic effect on two types of gut bacteria.27
Lab data demonstrated the products can trigger beneficial bacteria to become pathogenic and potentially increase your risk of serious health conditions. This was the first study to demonstrate how two types of beneficial bacteria can become diseased and invade the gut wall. The bacteria studied were Escherichia coli (E. coli) and Enterococcus faecalis (E. faecalis).
This research supports past evidence that noncaloric artificial sweeteners induced “compositional and functional alterations” in the gut microbiome.28 Data have also shown that artificial sweeteners can increase the permeability of the intestinal epithelial barrier, which leads to systemic inflammatory diseases. In the lab,29 high concentrations of aspartame and saccharin induced cell death and at low concentrations, it increased the epithelial permeability.
Two strategies that also play a role in your gut microbiome are getting more sleep and sunshine. Researchers have found a curious bidirectional link between your gut health and sleep. One study published in the Frontiers of Psychiatry noted:30
“There is considerable evidence showing that the gut microbiome not only affects the digestive, metabolic, and immune functions of the host but also regulates host sleep and mental states through the microbiome-gut-brain axis.
Preliminary evidence indicates that microorganisms and circadian genes can interact with each other. The characteristics of the gastrointestinal microbiome and metabolism are related to the host’s sleep and circadian rhythm.”
As noted in the Frontiers in Psychiatry study,31 mounting research suggests your gut microbiome helps regulate not only your mood but also your sleep cycle through what’s known as the gut-brain axis — a bidirectional communication “highway” that links your central and enteric nervous systems.32
During the past pandemic months, it has become increasingly obvious that maintaining optimal levels of vitamin D could help reduce your risk of infectious disease.33 A research team from the University of British Columbia was also interested in how exposure to UVB light may affect the human gut microbiome.34
Past studies had suggested vitamin D could alter the gut microbiome35 and since there are few natural foods that contain vitamin D,36 a vast majority of your body’s requirement is usually met through skin exposure to UVB light.37
The researchers from British Columbia noted that past research has shown sunlight has a positive effect on those with inflammatory bowel disease and multiple sclerosis, both of which are exacerbated by inflammation.38 In this clinical pilot study the researchers found the fecal microbiota were positively altered after exposure to sunshine. They wrote:39
“This is the first study to show that humans with low 25(OH)D serum levels display overt changes in their intestinal microbiome in response to NB-UVB skin exposure and increases in 25(OH)D levels, suggesting the existence of a novel skin-gut axis that could be used to promote intestinal homeostasis and health.”
Optimize Your Gut Microbiome
The choices you make every day have an impact on your gut microbiome. Optimizing your gut flora and vitamin D level is crucial to good health. Regularly eating traditionally fermented and cultured foods is the easiest, most effective and least expensive way to make a significant impact on your gut microbiome.
Healthy choices include lassi (an Indian yogurt drink), cultured grass-fed organic milk products such as kefir and yogurt, natto (fermented soy) and fermented vegetables of all kinds. Generally, I believe the majority of your nutrients need to come from food. However, supplemental probiotics are an exception if you don’t eat fermented food on a regular basis. Spore-based probiotics, or sporebiotics, can be helpful if antibiotics are necessary.
In addition to getting enough quality sleep and maintaining optimal levels of vitamin D, it is also important to feed your beneficial bacteria the nutrients they need to thrive. While harmful bacteria thrive on sugar and carbohydrates, beneficial bacteria thrive on fiber.
According to a study published in 2019 in The Lancet40 people eating 25 to 29 grams of fiber each day had a reduced risk of a range of critical outcomes, such as stroke, coronary heart disease, Type 2 diabetes and all-cause mortality. However, they found eating 29 grams a day was merely adequate, writing:41
“Dose-response curves suggested that higher intakes of dietary fiber could confer even greater benefit to protect against cardiovascular diseases, Type 2 diabetes, and colorectal and breast cancer.”
Many health officials and world leaders are finally acknowledging that the COVID shots cannot end the pandemic and that we must learn to live with the virus. Some have even started speaking out against repeated boosters
A major driver for this U-turn in the pandemic narrative is the emergence of the Omicron variant. While incredibly infectious, it causes only mild cold symptoms in the vast majority of people; it’s ripping through populations, leaving natural herd immunity in its wake. As a result, many are now claiming the end of the pandemic is in sight
Nearly 100% of COVID cases in the Boston area are now Omicron. In New England, the current outbreak is predicted to rapidly wane and disappear during the month of February 2022. As of early January 2022, Omicron was responsible for about 73% of all COVID cases in the U.S.
After two years of repetitive fearmongering, most people have had enough. The general consensus appears to be that people are ready to brave life even if the threat of COVID remains
With that baseline of natural immunity that Omicron provides, populations will, going forward, be far better equipped to handle any new strains that emerge, without a significant increase in mortality
For nearly a year, experts have noted that the COVID shots cannot establish herd immunity to end the pandemic, as the gene transfer injections do not prevent infection or transmission.
It’s not rocket science, yet health officials and government leaders around the world have irrationally claimed otherwise, and censored any and all — regardless of credentials — who dared to suggest alternative approaches.
Now, all of a sudden, the narrative is rapidly changing, with loads of these same individuals — truthfully, if you can believe that — acknowledging that the COVID “vaccines” cannot end the pandemic and that we need to learn to live with the virus. Some have even started speaking out against repeated boosters, at least at intervals of three to four months.
It seems a major driver for this U-turn in the pandemic narrative is the emergence of the Omicron variant. While incredibly infectious, it causes only mild cold symptoms in the vast majority of people, so it’s essentially ripping through populations, leaving natural herd immunity in its wake. As a result, many are now claiming the end of the pandemic is in sight.1
Moving on From COVID
In a January 15, 2022, Trial Site News article, Mary Beth Pfeiffer reported:2
“The director of global infectious diseases at Massachusetts General Hospital is predicting what was unthinkable less than a month ago: The end of the pandemic. Dr. Edward Ryan made stunning and encouraging comments on the Omicron variant that give hope for a return to normalcy.
Among these: Omicron will make boosters unnecessary. The COVID virus will join the ranks of the ‘common cold.’ And the latest wave will enter ‘clean up mode’ shortly. ‘We are fighting the last war with COVID and should be pivoting back to normal life,’ the summary of Dr. Ryan’s comments states. ‘Spring/Summer will be really nice!'”
According to Ryan, nearly 100% of COVID cases in the Boston area are now Omicron, which is good news, considering it doesn’t appear to bring with it any of the more severe side effects seen with previous strains, including Delta. In New England, the current outbreak is predicted to rapidly wane and disappear during the month of February 2022. Nationwide, Omicron was reportedly responsible for about 73% of all cases as of early January 2022.3
Pfeiffer also reports that, according to Ryan, booster shots will not be needed for Omicron, as by the time a dedicated injection is released, the wave will already be over and done with. Ryan is reported to have stated that “we’re all going to get it, which will give us the immunity we need to get through it,” referring to the Omicron infection.
Ryan’s comments fly in the face of mainstream medical recommendations, which near-universally call for boosters for everyone, including children. Clearly, however, Ryan makes a lot of sense. The boosters, while seemingly able to temporarily raise a double-jabbed person’s resistance against Omicron, it’s designed to protect against the original SARS-CoV-2 strain that no longer exists.
Overall, it appears the only reason a double-jabbed person would need a booster against Omicron is because the first two doses impaired their immune system such that they’re now more vulnerable, even to a milder strain. This downward spiral of negative immunity can only continue if people continue to take boosters, especially mismatched ones.
Vaccine-Induced Herd Immunity Called Out as ‘Myth’
In early August 2021, the director of the Oxford Vaccine Group, professor Sir Andrew Pollard, actually spoke out against the idea that the COVID shots were the answer everyone was looking for. At the time, he referred to the idea that vaccine-induced herd immunity against COVID was “mythical.” As reported by Yahoo! News, August 10, 2021:4
“… Pollard … said … that herd immunity is ‘not a possibility’ with the current Delta variant. He called the idea ‘mythical,’ warning that vaccine programs should not be developed around it.
‘We know very clearly with coronavirus that this current variant, the Delta variant, will still infect people who have been vaccinated and that does mean that anyone who’s still unvaccinated, at some point, will meet the virus,’ Pollard told a session of the All-Party Parliamentary Group (APPG) on coronavirus.
He said that while vaccines might ‘slow the process’ of transmission down, they cannot currently stop the spread completely.
‘I think we are in a situation here with this current variant where herd immunity is not a possibility because it still infects vaccinated individuals,’ he said, predicting the next thing may be ‘a variant which is perhaps even better at transmitting in vaccinated populations.’ He added: ‘So that’s even more of a reason not to be making a vaccine program around herd immunity.'”
During that same APPG meeting, professor Paul Hunter from the University of East Anglia stressed that variants capable of evading the COVID shots were “an absolute inevitability.” Pollard and Hunter both turned out to be correct, as Omicron’s vaccine-evading capacity has now been documented.
Most People Are ‘Done’ With COVID
The reprieve Omicron provides could not have come at a better time. At this point, after two years of repetitive fearmongering, most people have simply had enough. It’s not often you put a hold on life for this long, and the general consensus appears to be that people are ready to brave life even if the threat of COVID remains.
In a December 22, 2021, Atlantic opinion piece, Yascha Mounk, associate professor at Johns Hopkins University and a senior fellow at the Council on Foreign Relations, noted that “No matter the severity of the variant, the appetite for shutdowns or other large-scale social interventions simply isn’t there.” He goes on:5
“It feels like everyone I know has COVID … The pattern among my circle of friends fits with what’s unfolding in South Africa, where the coronavirus’s new Omicron variant was first identified.
The number of cases in the country shot up quickly, but the number of deaths has so far increased much, much more gradually — possibly indicating that Omicron is more contagious but causes less severe disease than previous variants …
I wager that, whatever course Omicron — or future strains of the disease — might take, we are about to experience the end of the pandemic as a social phenomenon …
Despite skyrocketing caseloads, few pundits or politicians are proposing strict measures to slow the virus’s spread. The appetite for shutdowns or other large-scale social interventions simply isn’t there …
Scientists have their own way of deciding that a pandemic is over. But one useful social-scientific marker is when people have gotten used to living with the ongoing presence of a particular pathogen.
By that definition, the massive surge of Omicron infections that is currently coursing through scores of developed countries without eliciting more than a half-hearted response marks the end of the pandemic.”
Mounk, like others, pointed out that if Omicron turned out to be as mild as it initially appeared — which has been borne out since then — then natural herd immunity would develop as the highly infectious virus spread like wildfire. With that baseline of natural immunity, populations would, in the future, be far better equipped to handle any new strains that emerge, “without a significant increase in mortality.”
Living With Risk
Mounk goes on to discuss how, over time, people get used to and learn to live with all sorts of risks, including direct threats to life and limb, and that’s exactly the kind of resiliency we see building and spreading now:6
“When I was growing up in Germany, I was fascinated by news reports about life in very dangerous places. Residents of Baghdad or Tel Aviv seemed to put themselves in danger simply by going shopping or meeting friends for a cup of coffee.
How, I wondered with a mixture of horror and admiration, could anybody be willing to accept such an existential risk for such a trivial pleasure?
But the truth of the matter is that virtually all humans have, for virtually all of recorded history, faced daily risks of disease or violent death that are far greater than those that the residents of developed countries currently face.
And despite the genuine horrors of the past 24 months, that holds true even now … The determination to get on with our lives is deeply and perhaps unchangeably human.
In that sense, the spring of 2020 will be remembered as one of the most extraordinary periods in history — a time when people completely withdrew from social life to slow the spread of a dangerous pathogen. But what was possible for a few months has turned out to be unsustainable for years, let alone decades.
Whatever damage Omicron might wreak in the immediate future, we will, most likely, soon lead lives that look a lot more like they did in the spring of 2019 than in the spring of 2020.”
Do You Have a Cold, Flu or COVID?
Based on what I’m seeing around me, it seems the prediction that Omicron will “get” just about everyone is likely to be true. People are sick in droves. The good news is that there’s little panic surrounding these cases. Most people are now realizing that there’s no need.
That said, I still recommend treating any COVID symptoms early and aggressively, just in case. As mentioned, the vast majority of SARS-CoV-2 infections are now related to Omicron, and the core symptoms are near-indistinguishable from the common cold and/or influenza. The most commonly reported symptoms of Omicron infection are:7
Fatigue
Cough
Congestion, sneezing and runny nose
Sore throat
Headache
Fever
In addition to these, other symptoms commonly reported with SARS-CoV-2 infection, up to and including Delta, include:
Loss of taste or smell
Stomach/gastrointestinal pain (which in some cases could be a sign of microclots in the intestines8)
Nausea or vomiting
Diarrhea
A key difference in symptomology between Delta and Omicron is that Omicron does not appear to cause the loss of taste and smell, which often occurs with Delta infection (as with previous strains). Fortunately, Omicron also does not seem to be associated with blood clots, like previous strains (especially the initial ones), and it’s also far less likely to cause severe lung infection and damage.9,10
Treat Symptoms Early
Considering the uncertainties around diagnosis, it’s best to treat any cold or flu-like symptoms early. At first signs of symptoms, start treatment. Perhaps it’s the common cold or a regular influenza, maybe it’s the much milder Omicron, but since it’s hard to tell, your best bet is to treat symptoms as you would treat earlier forms of COVID.
Considering how contagious Omicron is, chances are you’re going to get it, so buy what you’ll need now, so you have it on hand if/when symptoms arise. And, remember, this applies for those who have gotten the jab as well, since you’re just as likely to get infected — and perhaps even more so. Early treatment protocols with demonstrated effectiveness include:
A doctor who has been offering free telehealth services to COVID-19 patients during the pandemic says that early treatment for COVID-19 works, claiming that he has a 99.99 percent survival rate.
“We have a team of volunteer free doctors that donate their time to help treat these patients that come to us,” Dr. Ben Marble, the founder of myfreedoctor.com, an online medical consultation service, said at a roundtable discussion hosted by Sen. Ron Johnson (R-Wis.) on Jan. 24.
He added, “We deliver the early treatment protocols to them as early as we can, and we have a 99.99 percent survival rate. So, I believe myfreedoctor.com, the free volunteered doctors have settled the science on this—early treatment works, period!”
Marble was answering Johnson’s question about what people can do if they or their loved ones have COVID-19.
People can visit the website myfreedoctor.com, create an account, and fill out a patient intake form if the doctors are accepting new patients for that day. One of the doctors will then reach out in less than 24 hours. With a huge demand for their services, the physicians say they can only “accept a certain number of patients each day.”
Marble says that he and his small team of volunteer doctors prescribe Dr. Peter McCullough’s treatment protocol, which consists of hydroxychloroquine, ivermectin, monoclonal antibodies, prednisone, and other low-cost generic drugs. They also prescribe vitamins D and C, and zinc.
Vitamin C bottles were on display in Miami, Florida on June 15, 2001. (Joe Raedle/Getty Images)
McCullough, a cardiologist, and epidemiologist, along with several physicians put together an early treatment protocol to provide outpatient care for COVID-19 patients. Their paper was published in The American Journal of Medicine in August 2020.
Dr. Pierre Kory, a pulmonologist and the President at the Frontline COVID-19 Critical Care (FLCCC) Alliance, says that the public is not aware that there are doctors across the country who will provide telehealth and early treatment for COVID-19.
“On our website, we have a button, which says find a provider. We’ve tried to collect as many telehealth providers that treat all states in the country,” Kory said.
“We are trying to let that message be known because that message is being suppressed that this disease is treatable,” he added.
Kory also claims that there is corruption at the federal level in suppressing early treatment with repurposed cheap drugs and their availability and that the Centers for Disease Control and Prevention (CDC) has been “captured by the pharmaceutical industry.”
“The corruption is because they don’t want you to use off-label, repurposed generic medicines. It does not provide profit to the system,” Kory said, adding that, “you know what’s going on in this country right now, is that the CDC has been captured by the pharmaceutical industry.”
“They sent out a memo in August of 2021, they sent out a similar memo back in the spring 2020, telling the nation’s physicians and pharmacists not to use generic medicines.”
The Epoch Times has reached out to the CDC for comment.
Early treatments were and continue to be discouraged by the CDC, whose guidance since the beginning of the pandemic up until January 2022, only focused on people self-quarantining for 14 days, keeping hydrated, taking analgesics, and only seeking hospital care when they can’t breathe or turn blue. They also warned people to not take any medications not approved for COVID-19.
“People have been seriously harmed and even died after taking products not approved for use to treat or prevent COVID-19, even products approved or prescribed for other uses,” the CDC wrote on its potential treatments webpage.
The weblink provided for the alleged harmful product was related to a March 2020 health alert warning of a serious health effect from ingesting non-pharmaceutical chloroquine phosphate used to clean fish tanks. This alert came after an Arizona man and his wife took the non-pharmaceutical drug in an attempt to self-medicate for COVID-19.
For the past two years, the U.S. Food and Drug Administration (FDA) has only authorized limited early outpatient treatments for COVID-19 that include monoclonal antibodies for high-risk patients and antiviral pills from Merck and Pfizer. However, the FDA on Jan. 24 announced it was limiting the use of Eli Lilly and Regeneron monoclonal antibodies only to patients “likely to have been infected with or exposed to a variant that is susceptible to these treatments.”
Johnson held the roundtable discussion to offer a different perspective on the response to the pandemic, including on “the current state of knowledge of early and hospital treatment, vaccine efficacy and safety, what went right, what went wrong, what should be done now, and what needs to be addressed long term.”
The discussion panel consisted of health experts and scientists that included McCullough, Dr. Robert Malone, and Dr. Paul Marik.
According to a press release, Johnson also invited over a dozen prominent figures involved in developing, promoting, and leading the pandemic response, including the CDC Director Dr. Rochelle Walensky and White House Coronavirus Response Coordinator Jeffrey Zients. All of the individuals declined to attend the forum.
Hospitalist can go to this website to review all the studies demonstrating ivermectin’s excellent results in the treatment of covid.
Indian Bar Association sues WHO scientist over ivermectin WHO gets sued over IVM
Step 4 – CAUTION if they want to give Remdesivir which has been taken off the WHO recommendation for covid treatment.
Dexamethasone – Dexamethasone, a corticosteroid, is similar to a natural hormone produced by your adrenal glands. It often is used to replace this chemical when your body does not make enough of it. It relieves inflammation (swelling, heat, redness, and pain) and is used to treat certain forms of arthritis; skin, blood, kidney, eye, thyroid, and intestinal disorders (e.g., colitis); severe allergies; and asthma. Dexamethasone is also used to treat certain types of cancer.
Vancomycin – Vancomycin is used to treat an infection of the intestines caused by Clostridium difficile, which can cause watery or bloody diarrhea.
Remdesivir Fraud, Failure, and Harm
Ohl, Michael E., Donald R. Miller, Brian C. Lund, Takaaki Kobayashi, Kelly Richardson Miell, Brice F. Beck, Bruce Alexander, Kristina Crothers, and Mary S. Vaughan Sarrazin. 2021. “Association of Remdesivir Treatment With Survival and Length of Hospital Stay Among US Veterans Hospitalized With COVID-19.” JAMA Network Open 4 (7): e2114741.
Yan, Victoria C., and Florian L. Muller. 2021. “Why Remdesivir Failed: Preclinical Assumptions Overestimate the Clinical Efficacy of Remdesivir for COVID-19 and Ebola.” Antimicrobial Agents and Chemotherapy, July, AAC0111721.
Step 6 – Use your judgement if you need to THREATEN with LEGAL ACTION if the hospital does not follow the patient’s requested protocol. Contact an attorney for legal assistance. Ralph C Lorigo has a lot of experience in this particular area.
Dexamethasone – Dexamethasone, a corticosteroid, is similar to a natural hormone produced by your adrenal glands. It often is used to replace this chemical when your body does not make enough of it. It relieves inflammation (swelling, heat, redness, and pain) and is used to treat certain forms of arthritis; skin, blood, kidney, eye, thyroid, and intestinal disorders (e.g., colitis); severe allergies; and asthma. Dexamethasone is also used to treat certain types of cancer.
Vancomycin – Vancomycin is used to treat an infection of the intestines caused by
Clostridium difficile, which can cause watery or bloody diarrhea.
How to Get the Hospitals to Administer the Proven Treatments:
12 And Jesus went into the temple of God, and cast out all them that sold and bought in the temple, and overthrew the tables of the moneychangers, and the seats of them that sold doves, 13 And said unto them, It is written, My house shall be called the house of prayer; but ye have made it a den of thieves.
Revelation 18:23 – “And the light of a candle shall shine no more at all in thee; and the voice of the bridegroom and of the bride shall be heard no more at all in thee: for thy merchants were the great men of the earth; for by thy sorceries were all nations deceived.”
There’s an even worse offender than sugar for your immune system and overall health: industrially processed seed oils, often referred to as “vegetable oils”
At the root of the harmful biochemical reactions triggered by seed oils is linoleic acid, the primary fatty acid found in polyunsaturated fatty acids (PUFAs)
The dramatic increase in seed oil intake in recent decades is a key culprit behind the soaring rates of heart disease, cancer, age-related macular degeneration, diabetes, obesity and dementia
Unsaturated fat intake is associated with increased mortality from COVID-19, while saturated fat intake lowers your risk of death
Linoleic acid is found in most processed foods, including sauces and salad dressings, along with “healthy” foods like chicken, pork and olive oil
What you eat plays a significant role in how well your immune system functions. As a result, you can actively support your body’s ability to ward off acute and chronic conditions with each food you put into your mouth. However, depending on your food choices, you can also hinder it.
What’s the worst ingredient for your immune system? If you guessed sugar, nice try, but there’s an even worse offender that’s just as prevalent but not as widely recognized for its pernicious influence on health: industrially processed seed oils, often referred to as “vegetable oils.”
At the root of the harmful biochemical reactions triggered by seed oils is linoleic acid, which is an 18-carbon omega-6 fat. Linoleic acid is the primary fatty acid found in polyunsaturated fatty acids (PUFAs) and accounts for about 80% of the fatty acid composition of vegetable oils. Omega-6 fats must be balanced with omega-3 fats in order to not be harmful, but this isn’t the case for most Americans.
Why Seed Oils Are Even Worse Than Sugar
An immunologist with CNBC News recently named sugar the “worst food ingredient for your immune system,”1 in large part because consuming too much of it can contribute to insulin resistance and obesity, which increases inflammation in your body and causes damage to blood vessels.
While your immune system is busy tending to these areas, CNBC notes, “This creates a major distraction for the immune system and paves the way for dangerous bacteria and viruses to slip through our body’s defenses.”2 In fact, it’s been known since at least the 1970s that sugar weakens the immune system (while fasting strengthens it),3 and I recommend limiting added sugars to a maximum of 25 grams per day or 15 grams a day if you’re insulin resistant or diabetic.
But most health “experts” simply do not understand that seed oils are even worse than sugar. These fats become embedded in your cell membranes and stay there for about seven years, wreaking havoc on your health.
Not only are most of the omega-6s you eat, including seed oils, damaged and oxidized through processing, but even if they are unheated and pristine when consumed in any but small amounts, your body degrades them into free radicals that damage virtually every tissue in your body.
“Most of this linoleic acid, when it oxidizes, it develops lipid hydroperoxides and then these rapidly degenerate into … oxidized linoleic acid metabolites,” says Dr. Chris Knobbe, an ophthalmologist and the founder and president of the Cure AMD Foundation.4
OXLAMs (oxidized linoleic acid metabolites) create a perfect storm, as they are cytotoxic, genotoxic, mutagenic, carcinogenic, atherogenic and thrombogenic, according to Knobbe. Their atherosclerosis and thrombogenic actions are especially concerning because they can produce strokes and clots, however metabolic dysfunction can also occur.
During the lipid peroxidation cascade caused by the excess consumption of omega-6 seed oils, PUFAs accumulate in your cell membranes, leading to a peroxidation reaction. Because there are so many reactive oxygen species it leads to the development of insulin resistance at the cellular level. OXLAMs are also toxic to the liver and are associated with inflammation, fibrosis and fatty liver disease in humans.5
Dr. Paul Saladino, a physician journalist, also explained in a podcast that linoleic acid “breaks the sensitivity for insulin at the level of your fat cells,”6 essentially making them more insulin sensitive — and, since your fat cells control the insulin sensitivity of the rest of your body by releasing free fatty acids, you end up with insulin resistance.
There’s virtually nothing more destructive to your body than seed oils in producing heart disease, cancer, age-related macular degeneration, diabetes, obesity and dementia.7 When I interviewed Tucker Goodrich, who developed an IT risk management system used by two of the largest hedge funds in the world, then transitioned into medical research, he explained that animals typically develop cancer once the linoleic acid in their diet reaches 4% to 10% of their energy intake.
Yet, most Americans get approximately 8% of their calories from seed oils. “So, we’re way over what these thresholds in the lab would suggest is a safe level of these fats based on the laboratory work in animals,” Goodrich said, adding:
“We’ve got this huge disconnect between what the lab science tells us we should be doing and what our dietary guidelines tell us we should be doing. The scientists are saying, ‘Oh, look, it’s poison. It causes all the chronic diseases,’ and the government’s saying, ‘Eat lots of it.’ That’s not a good thing.”
Data also indicate that COVID-19 mortality rates are heavily influenced by the amount of unsaturated fats you eat. Simply put, unsaturated fat intake is associated with increased mortality from COVID-19, while saturated fat intake lowers your risk of death.8 The authors noted that unsaturated fats “cause injury [and] organ failure resembling COVID-19.”
More specifically, unsaturated fats are known to trigger lipotoxic acute pancreatitis, and the sepsis and multisystem organ failure seen in severe cases of COVID-19 greatly resembles this condition. In short, linoleic acid contributes to the inflammatory domino effect that eventually kills some people with COVID-19. Goodrich explained:
“I did an enormous post on this, looking at the effects of LA [linoleic acid] in SARS COV-2 and SARS in general. SARS is a severe acute respiratory syndrome. SARS kills you by giving you acute respiratory distress syndrome (ARDS).
ARDS can be caused by lots of different things, not just these viruses. You can get it from influenza. You can get it from inhaling acid into your lungs. What’s fascinating is the human literature is quite clear that you can induce ARDS through feeding seed oils.
Very sick people who can’t eat are fed intravenously. It’s called total parenteral nutrition (TPN). Generally, this is used through a product called Intralipid, which is made out of soybean oil and sugar. When you start to understand all this stuff, it’s just mind boggling. Doctors did an experiment after they noticed that a lot of their patients who came into the ICU and got TPN then subsequently got ARDS.
So, they started playing with what they were feeding them, and what they discovered was this soybean oil formula increased the patient’s rate of getting ARDS. The fatality rate from ARDS is 30% to 60%. Feeding seed oils increased the rate of ARDS by seven times.”
It’s Hidden in ‘Healthy’ Foods, Like Chicken and Olive Oil
Another reason why linoleic acid is so harmful is because it’s found in virtually every processed food, including restaurant foods, sauces and salad dressings. Many processed foods high in sugar also contain seed oils, which is why eliminating them from your diet is essential for improving and maintaining your health.
However, even if you cut out processed foods and skip sauces and salad dressings when you eat out, you may still be consuming too much seed oil because it’s hidden in “healthy” foods like chicken and pork. The problem is that these animals are fed grains that are high in linoleic acid,9 which makes the meat a major source as well. So if you’re eating chicken and pork, believing it to be good for you, you’re being misled.
Olive oil is another health food that’s a hidden source of linoleic acid; however, there are caveats. As Goodrich explained, the linoleic acid content of olive oil can vary significantly. “The percentages that I’ve seen quoted in literature range from 2%, which is awesome, to 22%, which is not good,” he said.
Olive oil also has the benefit of containing beneficial oleic acid, which is protective against both cardiolipin oxidation and LDL oxidation. Cardiolipin is a type of fat located in your mitochondria, and oxidation of cardiolipin is one of the things that controls autophagy.
By altering the composition of cardiolipin in your mitochondria to one that’s richer in omega-6 fats, you make it far more susceptible to oxidative damage. Goodrich cites research showing that when the linoleic acid in cardiolipin is replaced with oleic acid like that found in olive oil, the cardiolipin molecules become highly resistant to oxidative damage.
The other variable, however, is that olive oil is often cut with cheaper seed oils, which raises the linoleic acid content. So if you consume olive oil, I strongly recommend keeping close track of your total linoleic acid intake.
How Much Linoleic Acid Is Too Much?
Many now understand that your omega-6 to omega-3 ratio is very important, and should be about 1-to-1 or possibly up to 4-to-1, but simply increasing your omega-3 intake won’t counteract the damage done by excessive linoleic acid. You really need to minimize the omega-6 to prevent damage from taking place.
Ideally, consider cutting linoleic acid down to 2 or 3 grams per day, which is close to what our ancestors used to get before all of these chronic health conditions, including obesity, diabetes, heart disease and cancer, became widespread. If olive oil puts you over the limit, consider cooking with tallow or lard instead. Beef tallow is 46% oleic acid and lard is 36% oleic acid.
Remember, linoleic acid is considered an essential fat, so you don’t want to eliminate it entirely. It’s only when consumed in excessive amounts that linoleic acid acts as a metabolic poison — but virtually everyone is consuming excessive amounts.
What amount is “excessive”? Anything over 10 grams a day is likely to be problematic, although the exact cutoff is still unknown. In 1909, Americans ate 2 grams a day of vegetable oil, according to Knobbe, but by 2010 this had increased to 80 grams a day.10
If you’re not sure how much you’re eating, enter your food intake into Cronometer — a free online nutrition tracker — and it will provide you with your total linoleic acid intake. The key to accurate entry is to carefully weigh your food with a digital kitchen scale so you can enter the weight of your food to the nearest gram.
Cronometer will tell you how much omega-6 you’re getting from your food down to the 10th of a gram, and you can assume 90% of that is linoleic acid. Again, anything over 10 grams is likely to cause problems. Since there’s no downside to limiting your linoleic acid, you’ll want to keep it as low as possible, which you do by avoiding high-LA foods. This means eliminating all of the following oils:
Soy
Corn
Canola
Safflower
Sunflower
Peanut
Other high-LA foods include chips fried in vegetable oil, commercial salad dressings and sauces, virtually all processed foods and any fried fast food, such as french fries. I’m currently writing a book on this topic as well, so stay tuned for more information about what I believe is likely the leading contributing cause of virtually all chronic diseases we’ve encountered over the last century.
Welcome to FlashPoint! Featuring Gene Bailey, Hank Kunneman, Lance Wallnau and Mario Murillo. Join in as they recap recent developments in the nation and discuss deep spiritual and political developments.
Continue to watch FlashPoint exclusively on VICTORY via DIRECTV Channel 366, DISH Channel 265, YouTube®, Roku®, Apple TV®, Amazon Fire TV, Glorystar, FaithNOW App, and https://www.govictory.com.
As of January 7, 2022, the U.S. Vaccine Adverse Events Reporting System (VAERS) has received 9,936 reports of death following the COVID jab in the U.S. When you include foreign reports received by VAERS, the death toll stands at 21,745
A total of 1,541 miscarriages have also been reported post-jab in the U.S., or 3,594 if you include foreign reports. Despite these shocking statistics, U.S. health officials and “fact checkers” insist not a single death can be attributed to the shots
According to OneAmerica, a national life insurance company, in the third quarter of 2021, working age Americans (aged 18 to 64) died at a rate that is 40% higher than the prepandemic rate, and they didn’t die from COVID
The Insurance Regulatory and Development Authority of India also reports a 41% rise in death claims in 2021, and teens’ mortality in the U.K. shot up 47% in the three months after they became eligible for COVID shots
A recent histopathologic analysis of the organs from 15 patients who died within seven days to six months’ post-jab, ages 28 to 95, found 14 of the deaths — 93% — were caused by the jab
As of January 7, 2022, just over a year into the campaign to inject every human being with a gene transfer product to protect against COVID, the U.S. Vaccine Adverse Events Reporting System (VAERS) has received 9,936 reports of death following the COVID jab in the United States’ territories alone.1 When you include foreign reports received by VAERS, the death toll stands at 21,745.
A total of 1,541 miscarriages have also been reported post-jab in the U.S., or 3,594 if you include foreign reports. Despite these shocking statistics, U.S. health officials and “fact checkers” insist not a single death can be attributed to the shots.
During an early January 2022 Senate committee hearing on the nation’s Omicron response (see video above), Centers for Disease Control and Prevention director Dr. Rochelle Walensky, and director for the National Institutes of Allergy and Infectious Diseases, Dr. Anthony Fauci, testified — under oath — that they “did not know” how many deaths had been reported to VAERS following COVID “vaccination.”2,3
Walensky referred to the shots as “incredibly safe,” claiming — against all science — that they “protect us against Omicron, they protect us against Delta, they protect us against COVID.” She also falsely claimed that all reported COVID-19 vaccine deaths have been “adjudicated.”
No, VAERS Is Not a Repository of Fake Reports
Worse yet, both Walensky and Fauci claim any and all adverse events following vaccination get reported to VAERS, including accidental deaths and car accidents. They both actually claim that if a person gets the COVID shot and gets hit by a car afterward, that is reported as an adverse reaction.
Nothing could be further from the truth. First of all, adverse events are not automatically reported and, certainly, obvious accidents are not entered into the system as a suspected vaccine side effect.
As reported by Health Impact News,4 there are about 18 reports in VAERS that include “road traffic accident,” but most if not all relate to an adverse event, such as a heart attack, occurring while driving. They were not hit by someone else and entered into the system. As noted by Pam Long in a January 12, 2022, Twitter thread:5
“If anyone in public health utters ‘a person can get hit by a car & report their death to VAERS’ you need stop them, in any public meeting, and demand they explain what motive would a physician have to inflate VAERS reports with car accidents or any unrelated mortality?
Despite Walensky’s & Fauci’s cliché testimony to Congress. Not one person ‘got hit by a car’ & reported their own death to VAERS as a vaccine injury. Most reports are filed by medical professionals, using diagnostic language about drug reactions.”
VAERS was designed and created as an early warning system. It’s true that anyone can file a report, but it’s time-consuming, requires the knowledge of medical details a patient oftentimes won’t have, and carries penalties for filing a false report. There’s absolutely no reason to suspect, let alone assume, that people are filing false reports just to make the shots look bad.
Fact Checker Outs Himself as a Pharma Propagandist
Walensky and Fauci aren’t the only ones lying about the lethality of the COVID jab. Mainstream media are all-in as well. In a USA Today fact check,6 Daniel Funke claims that “COVID-19 vaccines [are] safe for children” and “not linked to deaths.”
“… online, some claim children face more risk from the vaccine than COVID-19 itself,” Funke writes. “USA TODAY previously rated False a claim that children are 50 times more likely to die from the COVID-19 vaccine than the virus. This claim is similarly wrong.
Public health officials say the vaccine from Pfizer-BioNTech is safe and effective at preventing COVID-19 in children ages 5-11. As other independent fact-checking organizations have reported, the benefits of the vaccine outweigh its known and potential risks.
‘Over 700 children have died due to COVID-19 in the United States,’ Dr. Sonja Rasmussen, a professor in the departments of pediatrics and epidemiology at the University of Florida, said in an email.
‘I am not aware of any deaths in children that have been attributed to the COVID-19 vaccine’ … The benefits of the COVID-19 vaccine for children outweigh its known and potential risks, according to the CDC. The shot does not cause death.”
Funke cites data from Pfizer’s clinical trials, “which found the vaccine was safe” for children, as “no deaths were reported” in Pfizer’s trials for 12- to 25-year-olds, and those for 12- to 17-year-olds. Funke dismisses the rationale for looking at VAERS data on the basis that anyone can file a report and that reports are unverified, and therefore cannot be used to determine causation.
All Opinion and No Data
There are so many issues with this “fact-check,” no wonder Facebook attorneys are using the legal defense that fact checks are “opinion” only and not actual assertions of fact.7,8 There’s nothing but opinions in this piece. As “evidence” that the COVID shots are safe and have caused no deaths, Funke presents:
Another opinion piece by USA Today
The supposed opinion of unnamed “public health officials”
Biased opinion assertions by other pharma-funded propaganda organizations (aka, “fact checking organizations”)
The opinion of a single professor who admits she is unaware of publicly available data
The unsupported opinion of the Centers for Disease Control and Prevention, a captured agency that has repeatedly been caught manipulating data and changing definitions to fit the pandemic narrative
Pfizer’s preliminary trial data, which whistleblowers warn may have integrity issues9
The unsupported claim that VAERS data are unreliable because anyone can file, the implication being that people can file fake reports
The debatable claim that VAERS data cannot tell us anything about causation, hence it’s useless looking at it
It’s hard to come up with a less compelling list of evidences for safety, but then again, propagandists have to work with what they have, and in this case, they have nothing. Funke presents zero actual data to support his opinion.
Explain the Rise in Mortality if You Can
There are many data-driven reasons to suspect, predict and even assume that the COVID shots are killing more people than they’re saving — regardless of the age group in question. It would take an entire book to cover it all, so I will only review a few of those reasons here.
One very telling clue that recently came to light is life insurance data. According to OneAmerica, a national life insurance company based in Indianapolis, in the third quarter of 2021, working-age Americans (aged 18 to 64) died at a rate that is 40% higher than the prepandemic rate, and they didn’t die from COVID.10
And, according to CEO Scott Davidson, this catastrophic abnormality is consistently seen “across every player” in the life insurance industry.11 A 40% increase in mortality is simply unheard of, and as of yet, they claim to have no clue as to what’s causing young and middle-aged people to die prematurely at such an astounding rate.
Looking at it from a sleuth’s point of view, one might ask, “What environmental factor with unknown safety was introduced in 2021 to people in this age group?” Sure, pandemic restrictions have led to spikes in drug overdoses and suicides, which affects this cohort in particular. But “deaths of desperation” cannot account for all of it.
The one wild card is the COVID jab. More than 173 million working-age Americans (18 to 64) got these experimental gene transfer injections,12 and doctors and scientists have elucidated several mechanisms by which they might injure or kill.
What’s more, the rise in deaths began AFTER the rollout of the shots, and whatever the causative factor, it is not only national but likely international in scope. The Insurance Regulatory and Development Authority of India, for example, also reports a 41% rise in death claims in 2021.13
Excess deaths (exceeding prepandemic norms) are also reported in the U.K.14 Among teens (aged 15 to 19), mortality spiked right after teens became eligible for the COVID shot.15 Between the week ending June 26 and the week ending September 18, 2020, and that same period of time in 2021, teenage deaths rose by 47%.16
A rise in disability claims17 also suggests that many who aren’t killed by this novel lethal threat are seriously injured, often long-term. For all of these reasons, the COVID jabs cannot be taken off the table. Logic demands that they be looked into as a potential causative factor.
Can VAERS Data Demonstrate Causality?
One person who has taken a strong stance against the claim that VAERS data cannot tell us anything about causation is Steve Kirsch, executive director of the COVID-19 Early Treatment Fund. In the video “Vaccine Secrets: COVID Crisis,”18 he argues that VAERS can indeed be used to determine causality.
It’s important to realize that the idea that VAERS cannot show causality is part of how and why the CDC can claim none of the deaths is attributable to the COVID shot. Kirsch argues that this premise is in fact false, and that causation can be determined using VAERS’ data.
To prove his point, Kirsch gives the following analogy: Suppose you give a two-dose vaccine. After the first dose, nothing happens, but after the second dose, people die within 24 hours of a deep vein thrombosis (DVT).
When you look at the VAERS data, what you would find is no reports associated with the first dose, and a rash of deaths after the second dose, all within the same timeframe and with the same cause of death.
According to the CDC, you cannot ascribe any causality at all from that. To them, it’s just random chance that everyone died after the second dose, and from the same condition, and not the first dose or from another condition.
Kirsch argues that causality can indeed be identified from this kind of data. It’s very difficult to come up with another explanation for why people — many who are young, in perfect health with no predisposing conditions — die exactly 24 hours after their second dose. It’s even difficult to come up with another explanation for people who do have underlying conditions.
For example, is it reasonable to assume that people with, say, undiagnosed heart conditions, would die from DVT exactly 24 hours after getting a second dose of vaccine? Or that people with undiagnosed diabetes would die from DVT exactly 24 hours after their second dose?
Why not after the first dose, or two months after the second dose, or any other random number of hours or days, or for other random cause of death? Why would people randomly die of the same condition at the exact same time, over and over again?
At bare minimum, as an early warning system, VAERS is designed to flag potential causation. It’s by looking for repeated patterns of side effects that you would begin to identify a potentially problematic vaccine. Once a pattern is identified — and there’s no denying death within 24 hours to one week is a pattern seen for the COVID shots — an investigation should be launched.
But no such investigation has been launched for the COVID jabs. Clear-cut patterns are simply ignored. As an early warning system, VAERS is performing as intended, despite severe underreporting (the CDC recently published a paper in which they admit COVID jab adverse effects in children are underreported by a factor of 6.519). It’s the follow-up that’s lacking. But lack of investigation and follow-up is not evidence that the shots can’t cause death.
‘Bad Batches’ Are Another Clue
Another clue that hints at SOME of the shots being able to cause rapid death is the “bad batch” phenomenon. Independent investigations have revealed that some lots of the shots are associated with very severe side effects and death, whereas other lots have no adverse events associated with their use.
According to howbadismybatch.com, a site that matches up vaccine lot codes with reports in the VAERS system, approximately 5% of the lots are responsible for 90% of all adverse reactions. Some of these batches have 50 times the number of deaths and disabilities associated with them, compared to other lots.20
Another website that basically does the same thing is TheEagle’s VAERS Dashboard. (A video explaining how to use the dashboard can be found on Bitchute.21)
Dr. Reiner Fuellmich, cofounder of the German Corona Investigative Committee, and Dr. Wolfgang Wodarg, a former member of the German parliament, discuss this “smoking gun” evidence in the video above. According to Fuellmich and Wodarg, this lot-dependent data shows vaccine makers are conducting secret experiments within the larger public trial.
They appear to actually be doing lethal-dose testing on the public. Wodarg argues that the evidence for this is very clear from the data. They also appear to be coordinating these lethal-dose experiments, so that they’re not all releasing their most toxic lots at the same time, or in the same areas, so as to avoid detection through clustering.
More Data Showing COVID Jabs Can Kill
In closing, I will raise just two more pieces of evidence that speaks to COVID jabs having the ability to kill large numbers of people:
•A recent histopathologic analysis of the organs from 15 patients who died within seven days to six months’ post-jab, ages 28 to 95, found 14 of the deaths — 93% — were caused by the jab.22,23 None of the original coroners’ reports implicated the shots, however.
The association was only established through autopsy, which revealed a “process of immunological self-attack” that is “without precedent.” “Because vaccination was the single common denominator between all cases, there can be no doubt that it was the trigger of self-destruction in these deceased individuals,” Drs. Sucharit Bhakdi and Arne Burkhardt wrote.
•According to researchers at Columbia University, the real number of people killed by the COVID jabs is about 20 times the reported rate, based on their analysis of two publicly available databases (VAERS in the U.S., and another in Europe).24,25,26 That analysis was published in October 2021, but few ever heard a peep about it. According to the authors:
“Comparing our age-stratified VFRs [vaccine-induced fatality rates] with published age-stratified coronavirus infection fatality rates (IFR) suggests the risks of COVID vaccines and boosters outweigh the benefits in children, young adults and older adults with low occupational risk or previous coronavirus exposure.
We discuss implications for public health policies related to boosters, school and workplace mandates, and the urgent need to identify, develop and disseminate diagnostics and treatments for life-altering vaccine injuries.”
Based on the ever-mounting data, the claim that COVID shots have not, cannot, and/or will not cause death simply isn’t credible. And the longer these shots continue to be used, the greater the likelihood that they will indeed kill far more than the actual virus ever did. We also need to remember that the disabilities and long-term chronic ill health these shots are causing will prematurely kill many more, even if it takes 10 or 15 years, and we have no data on any of that yet.
The end-goal of vaccine passports is to surveil and collect not only medical information but also financial transactions, political affiliations, religious and philosophical beliefs and more
Disguised as a tool for convenience and safety, digitized IDs, such as mobile driver’s licenses, will be embedded into everyday life and used to control everything from food and sustainability to travel and mobility
There’s still time, however, to stop the imposition of totalitarian control worldwide, and a key way to do so is to fight back against vaccine passports
Investigative journalist Corey Lynn shared 22 ways to stop vaccine passports, from not complying and leaving your cellphone at home to using cash as much as possible and not supporting establishments that require vaccine passports
Vaccine passports are poised to change the world as you know it, creating a digital trail of your every move. Right now, it’s injection status that’s being highlighted, but the end goal is to surveil and collect not only medical information but financial transactions, political affiliations, religious and philosophical beliefs and more.
Some have speculated that the introduction of digital IDs and vaccine passports in the U.S. is laying the infrastructure for a social credit system. China’s social credit system, a massive undertaking of government surveillance that aims to combine 600 million surveillance cameras — about one for every two citizens — with facial recognition technology, has the reported goal of being able to identify anyone, anywhere, within three seconds.1
It’s difficult to imagine this type of tyranny transpiring in the U.S. — until you look back over the last two years. In 2019, it may also have seemed farfetched that you’d have to receive an injection of an experimental gene therapy in order to enter certain restaurants, gyms, entertainment venues and workplaces, yet, here we are.
As investigative journalist Corey Lynn, who recently detailed not only why it’s so important to stop vaccine passports but also 22 practical ways to do so, put it:2
“Simply put: the pandemic is to mandate an experimental gene therapy that the CDC likes to refer to as a ‘vaccine.’ That ‘vaccine’ is for purposes of getting everyone onto a vaccine ID passport. The passport is to force everyone into the new global social credit system.
That system is to bring the global population to full obedience, as the globalists control everyone’s access and spending to anything and everything in life, through the use of the new CBDC (central bank digital currency) system they are building toward.”
Are We Being Trained Like Dogs?
Lynn compared the vaccine ID passport system being rolled out to mandatory rabies vaccines for dogs. It might seem like a stretch, but there are many similarities between the rabies vaccine system and what could soon happen on a global scale, but this time to people, not dogs. Lynn writes:3
“Let’s put aside ‘rabies’ for one moment and look at the system that billionaire funders of big pharma and policymakers quickly put into place.
They made the vaccine mandatory, assigned an ID tag that dogs must wear, stored the information and address of the dog and its owner in a database, informed healthcare, retail, park services, and businesses that they should not provide services to those without this ID. If one doesn’t abide by this law, the owner can be fined, dog quarantined and force-vaccinated.”
Your dog can’t visit doggy day cares, dog parks or grooming centers unless he’s received the rabies shot. Failure to comply leaves your dog ostracized and you, as its owner, vulnerable to fines.
Lynn argues that, much like COVID-19, millions of pet owners have blindly gone along with the required rabies vaccines for their pets, despite questions over its safety and necessity on an annual basis, as studies suggest the shots may provide protection for more than six years.4
“They have tested this system on pet owners for years, and half the U.S. population willingly went along with this without even questioning it. Sound familiar?” Lynn asks. “… They are treating you like a dog, and they didn’t even show dogs the respect they deserve. You are nothing more than livestock to them.”5
How Digital Identities Threaten Your Freedom
Disguised as a tool for convenience and safety, digitized IDs, such as mobile driver’s licenses, “go way beyond what a driver’s license is about.”6 The World Economic Forum’s (WEF) Annual Meeting 2018 in Davos was focused on “advancing good, user-centric digital identities.”7 This isn’t simply a matter of maintaining your name, address and birthdate, or proof that you’ve passed your state’s driving exam.
Digital identities are described by WEF as “complex webs, crossing the internet, of … personal data, digital history and the inferences that algorithms can draw from this.”8 These identities, they say, “are increasingly embedded in everything we do in our daily lives.” In a figure that describes digital identity systems in our everyday lives, WEF envisions that digital IDs, i.e., vaccine passports, will encompass:9
Health care — to access insurance, monitor health devices and wearables and prove qualifications (for providers)
Smart cities — to monitor devices that transmit data about energy usage, air quality and traffic congestion
Telecommunications — for individuals to use devices and service providers to monitor them
E-government — for individuals to file taxes, vote and collect benefits
Social platforms — for social interactions
E-commerce — to shop, conduct business transactions and secure payments
Financial services — to open bank accounts and carry out financial transactions online
Food and sustainability — to verify the origin of produce and enhance traceability in supply chains
Travel and mobility — to plan trips and go through border control between countries or regions
Humanitarian response — to access services and demonstrate qualifications to work in a foreign country
As an example of how this can translate to threatening something as foundational as your food choices, Lynn uses the example of the “entitlements digital currency” benefits program for food stamps in Illinois, which uses smart contracts and healthy eating tokens. She explains:10
“[O]nce you have been verified with your digital identity, you are given a benefit wallet that connects to smart contracts, and if you should ever try to purchase food items that do not fall into their determined ‘healthy food’ category, you won’t be able to purchase it. Surely they are just looking out for your health. What this really shows is their ability to block access to anything they don’t wish you to purchase or have access to.
Once all banks are connected into this digital identity (vaccine ID passport) system, they will be able to control your spending on everything. What happens if you do not get the Covid jab or booster? Every area of your life, included in the digital identity diagram above, will be controlled through this system.
All data on your life will be stored within your digital identity. They sell this enslavement system as ‘convenience’ and ‘equity,’ while ensuring you that ‘you’ll own nothing and you’ll be happy.’”
22 Ways to Stop Vaccine Passports
Your entire identity, including your medical history, finances, sexual orientation and much more, could soon be stored in a mobile app that’s increasingly required to partake in society. While some might call this convenience, others would call it oppression. Many others are being driven by fear to accept vaccine passports as “necessary” to protect safety.
In one survey that evaluated acceptance of vaccine passports, 60% stated they were in favor and only 20% stated they were strongly opposed. The study’s lead author, professor Stephan Lewandowsky, described those opposed as “surprisingly low,” adding, “It’s fascinating how people seem increasingly receptive to their personal data being used to inform themselves and others about what they can and can’t do.”11
There’s still time, however, to stop the imposition of totalitarian control worldwide, and a key way to do so is to fight back against vaccine passports. Lynn highlights 22 ways to do just, which we can all take part in to protect privacy, freedom and constitutional rights.12
Do not comply, whether or not you’re coerced, bribed, guilted, intimidated or manipulated into complying. “Civil disobedience is necessary.”
Contact your investment adviser or asset manager. Give them a list of companies involved in vaccine passports and pushing the agenda, and tell them you no longer want to support them.
Avoid all digital identities and vaccine ID passports offered by banks, driver’s license facilities and other industries as a means of increasing “access” or “convenience.”
Tell your friends, family and acquaintances about the real goal of digital identities, which is to “put you on the Blockchain to surveil and control your every move.”
Contact your local sheriff. There are 3,081 sheriffs in the U.S., who should be contacted by phone, email and mail. They have the power to refuse to enforce illogical or illegal demands.
Share messages of truth around your community. You can spread the word using flyers, postcards, stickers or “swag with a message.”
Don’t support establishments that require proof of a shot or negative test. If you do, give them a card that reads, “I will not be a human experiment of a gene therapy jab for a virus that has a 99.98% survival rate.”
Email your state representative to block vaccine passports and digital IDs. Support and consider donating to those who are taking action against injection mandates and passports.
Move your money from large banks to small, family-owned banks and small credit unions. “If 10% of people did this, it would create a huge shift.”
Build family or community energy and food systems, as “resilient energy and food supplies will go a long way against their digital financial blackmailing systems.”
Boycott Amazon and big box stores that are “building the infrastructure to enslave humanity.”
Use cash as much as possible, as it allows you to avoid being tracked via your bank account and keeps your spending behaviors from being analyzed and used to manipulate industries, supply chains and markets.
Leave your cellphone at home and avoid any and all data-tracking apps.
Limit the personal data you share online, on paper and anywhere else.
Call your senators and demand that they oppose the Federal Vaccine Database Bill H.R. 550, which would allow the development of a federal vaccination registry.
Avoid purchasing “smart” products of any kind, such as smart televisions and Alexa devices. “These products are all used for surveillance purposes via audio, some visual, and data aggregating, not to mention potential integrated mind control technologies.”
Establish financial security outside the system, such as by learning or teaching trade skills and establishing networking and teamwork opportunities for people to build and work together within their local community.
Clear as many debts as you can so you aren’t beholden to anyone. “Invest in people, learning trade skills, family and community, hard assets, proper schooling for your children — which might mean a local homeschool network — local farmers for your food, any necessary supplies or equipment you feel you need, your health and peace of mind.”
Maintain resources — medical, legal and otherwise — to fight the COVID-19 tyranny13 and stay updated on legal action and legislation against COVID-19 mandates.
Be aware that it is not legal to require a person to get injected while it’s still under emergency use authorization. “Though the FDA has approved Pfizer’s Comirnaty jab, Pfizer has chosen to not yet produce it for the U.S., and instead are continuing to supply the EUA jab.”
Be there for those who have received the injection and are having adverse events or choosing not to get boosters. “Help them through it and find medical professionals that are aware of what is happening and will assist them.”
“Visualize a better future for all, where these corrupt individuals are stopped in their tracks.”
The women featured in this video are not anti-vaccine. They did what the CDC told them and stepped to the plate and took their COVID shots.
What happened afterward to each of them, however, has every single one expressing her regret over getting the shot. Each has neurological and other problems and they are begging people to listen to their stories to set the record straight and help them get the help they so desperately need.
In mid-February 2021, Dr. Andrew Hill at Liverpool University published a scientific meta-analysis of six randomized controlled trials involving the use of ivermectin. The review, funded by the World Health Organization and UNITAID, found the drug increased viral clearance and reduced COVID-19 deaths by 75%, yet the conclusion of the paper was dismissive
In early April 2021, Hill was accused of scientific misconduct by the French civic group, Association BonSens. BonSens claims Hill manipulated data to downplay the usefulness of ivermectin. Hill admitted that the study sponsor had crafted the conclusion
In early August 2021, Hill published a public notice stating one of the six studies included in his analysis had been withdrawn due to fraudulent data. A revised analysis excluding that study was published in November 2021
In the November revision, Hill included 23 randomized clinical trials, concluding ivermectin had no statistically significant effect on survival or hospitalizations
Other meta-analyses of 13 to 24 studies have found reductions in death ranging from 62% to 91%. Recent research has also found a five-day course of ivermectin at a dose of 12 mg per day sped up viral clearance, reducing the duration of symptomatic illness by three days compared to placebo (9.7 days versus 12.7 days)
In mid-February 2021, Dr. Andrew Hill at Liverpool University published a scientific meta-analysis of six randomized controlled trials involving the use of ivermectin in 1,255 COVID-19 patients. (The paper was initially posted on a preprint server.)
The review, which was funded by the World Health Organization and UNITAID, found that ivermectin increased viral clearance and reduced COVID-19 deaths by 75%. This is a rather massive benefit, yet the conclusion of the paper was dismissive, saying additional large clinical trials were needed to make a determination about whether or not to recommend its use.
Hill Accused of Scientific Misconduct
In early April 2021, Hill and his coauthors were accused of scientific misconduct by a French civic group called the Association BonSens. The TrialSite News video report from April 5 above reviews the details of this story. BonSens — labeled by some a “controversial group” based on its anti-mask mandate stance — accused Hill of data manipulation to downplay the usefulness of ivermectin.
According to BonSens, Hill’s analysis was then used by the WHO to recommend against ivermectin, even though it appears to have significant benefit. BonSens called on Hill to retract the paper, but Hill remained “resolute and stands behind the study,” TrialSite News said.
At the time, TrialSite News claimed to have been in conversation with “relevant and associated parties,” some of whom have asked to remain anonymous, who say Hill’s study was in fact modified, but that this was done “separate and apart from the investigator,” and that Hill had no say in the matter.
However, since then, one of the six studies Hill included in his analysis has been withdrawn “due to fraudulent data.” In a public notice1 dated August 9, 2021, Hill and his coauthors addressed the matter, saying they would submit “a revised version excluding this study, and the currently posted paper will be retracted.” A revised and updated meta-analysis was published in November 2021.2
The updated review includes data from 23 randomized clinical trials with a total of 3,349 patients. Studies with “high risk of bias” were excluded. In this analysis, Hill found that “Ivermectin did not show a statistically significant effect on survival or hospitalizations,” and had only “borderline significant effect on duration of hospitalization in comparison with standard of care.”
No significant effect on clinical recovery time was detected. In conclusion, the paper states that the WHO “recommends the use of ivermectin only inside clinical trials.” Curiously, it also states that “a network of large clinical trials is in progress to validate the results seen to date.” What results might those be? Surely, they must be referring to positive results, or else a network of clinical trials would hardly be justified.
Positive Ivermectin Studies Largely Barred From Publication
December 3, 2021, TrialSite News interviewed Dr. Tess Laurie (above) about her own ivermectin analyses and that of Hill. She points out that she was concerned when she saw the initial meta-analysis Hill published, as the conclusion didn’t match the data. The reduction in death was significant, yet the conclusion was dismissive.
Laurie contacted Hill, asking him to explain his conclusion to her. He then told her that the conclusion of the paper was not his own. It had been written by his sponsor — the WHO. Laurie was shocked, she said, as this struck her as a clear conflict of interest.
In the interview, Laurie also discusses the general difficulty researchers have had, since the beginning, in getting papers published that support ivermectin. She admits her own team has downplayed the benefits by using extremely conservative analyses in an effort to get published.
“It seems, if you tell it like it is, you are not going to get published because you might be accused of overstating your case. And if you understate it, you’re told there’s not enough evidence,” Laurie says.
Strong Evidence for Ivermectin
According to Laurie, the evidence for ivermectin in the treatment of COVID-19 is strong. In a previous interview, she reviewed a 13-study meta-analysis that found a 68% reduction in deaths. A follow-up review that included 15 studies found a 62% to 72% reduction in deaths.3
A meta-analysis4 by Laurie and her team published in the July-August 2021 issue of the American Journal of Therapeutics, which included 24 randomized controlled trials with a total of 3,406 participants, reported reductions in death ranging between 79% and 91%.
A study published February 2021 also reported that a five-day course of ivermectin at a dose of 12 mg per day sped up viral clearance, reducing the duration of symptomatic illness by three days compared to placebo (9.7 days versus 12.7 days).5
According to Laurie, what makes ivermectin particularly useful in COVID-19 is that it works both in the initial viral phase of the illness, when antivirals are required, and in the later inflammatory stage, when the viral load drops off and anti-inflammatories become necessary.
Dr. Surya Kant, a medical doctor in India who has written a white paper6 on ivermectin, claims the drug reduces replication of the SARS-CoV-2 virus by several thousand times.7 Kant’s paper led several Indian provinces to start using ivermectin, both as a prophylactic and as treatment for COVID-19 in the summer of 2020.8
Africa and Japan Defy the Odds With Ivermectin
Japan and Africa have also defied the odds with ivermectin. As reported by NewsRescue at the end of August 2021, “Melinda Gates, co-chair of the Bill and Melinda Gates foundation predicted disaster in the developing world, but so far she has been dead wrong, at least as far as Africa is concerned.”9
Indeed, despite having nearly 1.4 billion people, Africa has maintained one of the lowest COVID caseloads and death rates in the world, accounting for just 4% of the global reported death rate as of mid-May 2021.10 While media feign confusion, ivermectin may well be the explanation for this phenomenon.
A study11 published at the end of December 2020 found that African countries that participated in the African Program for Onchocerciasis Control (APOC), where intensive ivermectin mass campaigns were carried out between 1995 and 2015, had 28% lower COVID-19 mortality and 8% lower infection rates than non-APOC countries that did not participate in the ivermectin campaign.
“That a mass public health preventive campaign against COVID-19 may have taken place, inadvertently, in some African countries with massive community ivermectin use is an attractive hypothesis,” the authors said.12
Similarly, Japan has seen a massive decline in cases after adopting ivermectin as standard treatment against COVID. November 3, 2021, Free West Media reported:13
“The head of the Tokyo Medical Association appeared on national television in September urging doctors to use Ivermectin and they listened. A little over a month later, COVID-19 is under control in Japan …
Japan had slavishly adhered to all the Big Pharma prescriptions, including quarantine, contact tracing, masking, social distance, but finally the pandemic had hit them hard after they started aggressive vaccination in May 2021.
The results looked good initially, but in mid-July they started rising again and on August 6 cases hit a new all-time high and continued to rise.
Ivermectin was allowed as a treatment on August 13 and after 2 weeks the cases started to come down. In fact, they are now down 99% from the peak … In Japan, doctors can now prescribe it without restrictions, and people can buy it legally from India.”
Doctors Urge Acceptance of Ivermectin to Save Lives
In the U.S., the Frontline COVID-19 Critical Care Alliance (FLCCC) has been calling for widespread adoption of ivermectin, both as a prophylactic and for the treatment of all phases of COVID-19.14,15
FLCCC president Dr. Pierre Kory, former professor of medicine at St. Luke’s Aurora Medical Center in Milwaukee, Wisconsin, has testified to the benefits of ivermectin before a number of COVID-19 panels, including the Senate Committee on Homeland Security and Governmental Affairs in December 2020,16 and the National Institutes of Health COVID-19 Treatment Guidelines Panel January 6, 2021.17 As noted by the FLCCC:18
“The data shows the ability of the drug Ivermectin to prevent COVID-19, to keep those with early symptoms from progressing to the hyper-inflammatory phase of the disease, and even to help critically ill patients recover.
Dr. Kory testified that Ivermectin is effectively a ‘miracle drug’ against COVID-19 and called upon the government’s medical authorities … to urgently review the latest data and then issue guidelines for physicians, nurse-practitioners, and physician assistants to prescribe Ivermectin for COVID-1919 …
… numerous clinical studies — including peer-reviewed randomized controlled trials — showed large magnitude benefits of Ivermectin in prophylaxis, early treatment and also in late-stage disease. Taken together … dozens of clinical trials that have now emerged from around the world are substantial enough to reliably assess clinical efficacy.”20
A one-page summary21 of the clinical trial evidence for Ivermectin can be downloaded from the FLCCC website. A more comprehensive, 31-page review22 of trials data has been published in the journal Frontiers of Pharmacology.
At the time of this writing, the number of trials involving ivermectin has risen to 71, including 31 randomized controlled trials. A listing of all the ivermectin trials done to date, with links to the published studies, can be found on c19Ivermectin.com.23
The FLCCC’s COVID-19 protocol was initially dubbed MATH+ (an acronym based on the key components of the treatment), but after several tweaks and updates, the prophylaxis and early outpatient treatment protocol is now known as I-MASK+24 while the hospital treatment has been renamed I-MATH+,25 due to the addition of ivermectin.
The two protocols26,27 are available for download on the FLCCC Alliance website in multiple languages.
Take Control of Your Health Care
If COVID-19 were an actual medical crisis and not an excuse for a tyrannical power grab, doctors would have been allowed, indeed encouraged, to work together to find solutions. Their successes would then have been announced everywhere. Without doubt, ivermectin would have featured heavily in such reports, as doctors around the world have attested to its benefits.
That’s not what happened, though, which tells us we’re not dealing with a medical crisis that governments actually want to solve. As reported by the FLCCC, its members have “been blocked in attempts to disseminate scientific information about ivermectin on Facebook and other social media with the FLCCC’s pages repeatedly being shut down.”28
Seasoned researchers like Laurie can’t get their research published, and the main thing they have in common is that they’re reporting positive results using ivermectin (and other common remedies). For nearly two years now, doctors and scientist have repeatedly shown we can control the COVID endemic, even with new variants. We can save the vast majority from severe illness and death.
Yet “authorities” within government, regulatory agencies and health agencies have refused to listen and insist there’s only one way forward — we need novel gene transfer injections that direct our cells to churn out the very toxin that makes COVID-19 so problematic. And when those shots are proven failures, the answer, these same “leaders” say, is more boosters!
Insanity is doing the same thing over and over, expecting different results. The good news is you can choose who you listen to. You can listen to frontline medical experts, like the FLCCC, and follow their advice.
In a blow to U.S. President Joe Biden’s plan to jab every federal employee with a COVID-19 shot, a judge in Texas blocked Biden’s order.
“Judge Jeffrey Vincent Brown called the mandate an overstep of presidential authority and cited the recent Supreme Court decision to strike down a separate administration mandate that had applied to private sector workers,” CNN reported.
Brown added that Biden has no statutory power to mandate vaccines for federal workers. The Biden administration responded immediately with an appeal to a circuit court.
Our next guest wants to remain anonymous, for understandable reasons. She’s a nurse in California, which might as well be Stalinist Russia for how it treats its inhabitants. Our whistleblower says she sees the same pattern repeat over and over: Patients get put on remdesivir and another deadly “medicine,” Vancomycin, which also damages the kidneys. Nobody is getting adequate nutrition or IVs. Nobody is given a nebulizer. Nobody gets antibiotics. The patients would end up dying from this, then the doctors rush in and rip their organs out since they’re donors. The Whistleblower Nurse joins us to discuss.
Humanity Is Carrying Out Its Own Great Reset Against Planet’s Corrupt Elite
The Alex Jones Show
Populist movements worldwide have done an excellent job of exposing the NWO corporate kleptocrats and their divide & conquer agenda! The corporate Deep State’s attempt to consolidate power via a controlled collapse has backfired and they are now a victim of their own evil designs! But the bad news is, like every tyrant & corrupt system in history, they are attempting to take us with them! Tune in NOW to lean how to stop them!
Phil tells the unfortunate story of his Grama’s short battle with Covid-19, and the circumstances surrounding her death. He then drops another key piece of intel to his followers, before taking a brief Q&A.
Canadian Prime Minister Justin Trudeau is a soft man.
His father, Fidel Castro, would probably call him a ‘useful idiot.’ Okay, maybe Castro isn’t Justin’s real father, but there certainly is a resemblance–and more importantly—Justin is acting like Castro.
Justin Trudeau praised Castro after his death. His father, Pierre Trudeau, visited Cuba about a year before Justin was born in order to praise the ruthless dictator in person. In fact, the entire Trudeau family seems to have a penchant for such dictators. Justin loves communist China and his father visited the Soviet Union in his younger years to praise Stalin. It’s no wonder Justin is becoming Canada’s tyrannical Prime Minister.
Justin is spoiled and morally squishy. To counteract his weakness he tries to look strong. He once put on fake eyebrows to make him appear more masculine.
He despises conservative media. Just before he arrived at an event, Justin ordered his government goons to rough up a Rebel News reporter. The physical assault was caught on camera. Justin would never dirty his snow white paws himself, but he has plenty of taxpayer-funded thugs willing to do it for him. The goons knew they would go unpunished. Justin, like Stalin and Castro, is not only above the law, he considers himself to BE the law. Justin said the Rebel News organization were not journalists, as if he gets to decide such a thing…just like Hillary thinks she can decide that Julian Assange is not a journalist.
Trudeau has had a field day with the so-called ‘pandemic.’ It enabled him to enter into a child-like state of glee at locking people down and insisting they get forcibly jabbed. Remember, Trudeau hates those who resist the dangerous and under-tested mRNA gene therapy drugs. He even called them ‘racist and misogynistic extremists.’ Like his fellow dictators Macron and New Zealand’s toothy Jacinda Andern, Trudeau is demonizing the unvaccinated in order to create division, fear, and paranoia that is necessary for them to cement their vaccine passport plans. They don’t care about health. They care about power and tracking everyone, which enables them to better manage through force the lives of their citizens on a granular level. It’s about replacing freedom with their tyranny of ’safety-ism.’
Now Trudeau must deal with outraged truckers who refuse the mandatory jabs along with millions of their countrymen who support them. They are driving to their Canada’s capitol, Ottawa, to express their anger. Will Justin use force to stop them? If he does, Canadian citizens will have a good opportunity to show just how soft Justin really is. Those who would use force against the truckers need to consider whether or not they are on the side of a dictator or the Canadian people who value freedom.
The world is being pushed around by a mere handful of power-mad monsters. All we have to do is stop complying and stop participating in the slavery they have baked up for us. I’ve read that Justin absolutely hates the rumor that Castro is his real father. We should all rub that in. The next time Justin faces crowds, perhaps they should chant, “Let’s go, Castro!”
America has been allowing and even legalizing the murder of the unborn for decades. They called it a woman’s right or choice, but they never included that it was a choice to murder their baby. All that has done is encourage those who are ok with murdering the most innocent among us to murdering them even when it’s not what mom wants. The evidence of this is the latest Pfizer documents that were examined by Dr. Mark Trozzi. I’ll share his findings that 100% of all the pregnant women who were followed through with on the COVID shots lost their babies.
Fauci now using CULT language to describe his “believers”
(Natural News) The infamous Tony Fauci appeared the other day on a Zoom call with Bloomberg‘s Francine Lacqua, during which he admitted that the Wuhan coronavirus (Covid-19) is nothing more than his own religious cult.
Lacqua read a question to Fauci from someone who wanted to know if we should all be worried about future Fauci Flu “variants” emerging, and what Fauci’s views are about Big Pharma companies taking advantage of this whole situation for profit.
Fauci responded with:
“Because there are some inherent non-believers that no matter what you say, they give you a real problem.”
In other words, not everyone belongs to Fauci’s virus cult. And these unbelievers are a problem because in order for his cult’s message and agenda to permeate and be a success, everyone must believe (watch below):
The strange digital meeting was attended by other covid cult members including Stéphane Bancel, a French billionaire and CEO of Moderna, as well as Richard Hatchett, CEO of the Coalition for Epidemic Preparedness Innovations (CEPI), and Annelies Wilder-Smith, a professor of infectious diseases research at the Lee Kong Chian School of Medicine in Singapore.
The logo of the World Economic Forum (WEF) was also stamped in the upper right-hand corner of the meeting. WEF founder Klaus Schwab, by the way, is the one spearheading the push for a “great reset” in which nobody owns anything and is still “happy.”
Fauci is on a crusade to force-convert more people into his covid religious cult
It turns out that the online gathering with Fauci was a WEF-launched effort to discuss the challenges the globalists are having in convincing the human “herd” to continue following along with the plandemic.
Many more people are now awake to the truth compared to in early 2020, and even some religious adherents who were full-fledged Branch Covidians have left the cult and never looked back.
This makes the Schwabs and Faucis of the world very nervous and upset because their religion requires full conversion and obedience, using force if necessary. Many no longer want to obey, and Fauci is now publicly drawing lines in the sand between believers and unbelievers in his religion.
“The emergence of the Omicron variant – and the reintroduction of national lockdowns, travel bans and quarantines – has reinforced the uncertainty of the COVID-19 pandemic,” reads a description about the event.
“Join experts and leaders to find out the possible scenarios for COVID in 2022 and beyond.”
Some people who were on the fence about Fauci now recognize that he is fully evil, based on his latest statements to the WEF. Hopefully his days in the limelight, and as a free man, are numbered.
Now that we have definitive proof of Fauci lying about illegal gain-of-function coronavirus research, among many other lies he has told, there is simply no more excuse as to why Fauci has not yet been arrested and tried for crimes against humanity.
“Oh patron saint of Wooohan, bestow your sanctum upon the unclean,” joked one commenter about Fauci and his death cult religion.
“I’m a believer,” wrote another. “I believe Fauxi is a lying tyrant whose fifteen minutes of fame were up two years ago.”
Another suggested that the believer vs. unbeliever narrative has been true since the very beginning, even if it took tyrant Fauci this long to fess up to it.
“Wishing, hoping or believing have nothing to do with the fact that you lied and the ‘vaccine’ isn’t a vaccine, it’s just a shot and it doesn’t work like you said it would and yet you double and triple down on the lies,” wrote another to Fauci. “That is a big wall of BS which will come crashing down on you.”
The latest news about the Fauci cult can be found at Evil.news.
After old age, obesity appears to be the most prominent risk factor for being hospitalized with COVID-19, doubling the risk of hospitalization in patients under the age of 60
Most COVID-19 patients have more than one underlying health issue. A study looking at 5,700 New York City patients found 88% had more than one comorbidity. Only 6.3% had just one underlying health condition and 6.1% had none
Obesity also makes you more vulnerable to infectious diseases by lowering your immune function
Elevated blood glucose levels appear to play a significant role in viral replication and the development of cytokine storms. The real pandemic here appears to be dysregulated glucose metabolism; in other words, insulin resistance
Amassing data suggest that even when in close, crowded quarters, the infection rate is rather low, and fit, healthy individuals are more likely to be asymptomatic than not when testing positive for SARS-CoV-2 infection
This article was previously published May 4, 2020, and has been updated with new information.
According to a January 2019 update by the U.S. Centers for Disease Control and Prevention, more than 122 million American adults have diabetes or prediabetes1 — conditions which have been shown to increase your chances of contracting and even dying from COVID-19.2,3,4,5,6,7 As noted in an April 16, 2020, report by The New York Times:8
“Obesity may be one of the most important predictors of severe coronavirus illness, new studies say. It’s an alarming finding for the United States, which has one of the highest obesity rates in the world.”
Obesity Appears To Be Independent Risk Factor for COVID-19
After old age, obesity appears to be the most prominent risk factor for being hospitalized with COVID-19 — doubling the risk of hospitalization in patients under the age of 60 in one study9 — even if the individual has no other obesity-related health problems. A French study10,11 also found obese patients treated for COVID-19 were more likely to require mechanical ventilation.
Dr. Leora Horwitz, director of the Center for Healthcare Innovation and Delivery Science at NYU Langone who co-wrote the paper12 “Factors Associated with Hospitalization and Critical Illness Among 4,103 Patients With Covid-19 Disease In New York City” — which has not yet been peer-reviewed — told The New York Times:13
“Obesity is more important for hospitalization than whether you have high blood pressure or diabetes, though these often go together, and it’s more important than coronary disease or cancer or kidney disease, or even pulmonary disease.”
Most COVID-19 Patients Have More Than One Comorbidity
While obesity may top the list of comorbidities — underlying conditions that make COVID-19 worse — investigations reveal most COVID-19 patients have more than one underlying health issue. A study14 looking at 5,700 New York City patients found 88% had more than one comorbidity. Only 6.3% had just one underlying health condition and 6.1% had none.
In this particular study,15 published in JAMA, high blood pressure at 53.1% beat obesity (41.7%) as the No. 1 most common comorbidity among hospitalized patients, followed by diabetes at 31.7% and coronary artery disease at 10.4%.
Co-author Karina Davidson, senior vice president for the Feinstein Institutes for Medical Research told Time magazine:16
“Having serious comorbidities increases your risk … We want patients with serious chronic disease to take a special precaution and to seek medical attention early, should they start showing signs and symptoms of being infected …”
Obesity Lowers Immune Function
According to The New York Times,17 one hypothesis for why obesity is worsening COVID-19 has to do with the fact that obesity causes chronic inflammation. Having more proinflammatory cytokines in circulation increases your risk of experiencing a cytokine storm. Obesity also makes you more vulnerable to infectious diseases by lowering your immune function.18,19,20,21,22,23
As noted in one such study,24 “there is a positive feedback loop between local inflammation in adipose tissue and altered immune response in obesity.” Yet another scientific review25 pointed out “There is strong evidence indicating that excess adiposity negatively impacts immune function and host defense in obese individuals.” A 2018 review article further explained:26
“Adipose tissue is now considered an extremely active endocrine organ that secretes cytokine-like hormones, called adipokines, either pro- or anti-inflammatory factors bridging metabolism to the immune system.
Leptin is historically one of most relevant adipokines, with important physiological roles in the central control of energy metabolism and in the regulation of metabolism-immune system interplay, being a cornerstone of the emerging field of immunometabolism.
Indeed, leptin receptor is expressed throughout the immune system and leptin has been shown to regulate both innate and adaptive immune responses.”
Glucose Metabolism Influences Cytokine Storms
An April 15, 2020, article27 in The Scientist also reviews new evidence28,29 that sheds further light on why obesity and diabetes are such potent risk factors for severe COVID-19 infection.
In a nutshell, higher blood glucose levels appear to play a significant role in viral replication and the development of cytokine storms. While the research in question looked at influenza A-induced cytokine storms, these findings may well be applicable in COVID-19 as well.
Cytokines are released by your immune system in response to foreign invaders. They, in turn, act as messengers that instruct other immune cells to fight the pathogen. In some cases, this immune response goes into overdrive, resulting in what’s known as a “cytokine storm” that can cause severe tissue damage and lead to death.
A cytokine storm response is typically the reason why people die from infections, be it the seasonal flu, Ebola, urinary tract infection or COVID-19. A critical player in cytokine production is the transcription factor interferon regulatory factor 5 (IRF5). In mice, genetically eliminating IRF5 protects them from influenza-induced cytokine storms.30
Interestingly, “the inflammatory response to influenza infections is also known to drive up glucose metabolism,” The Scientist reports,31 “in part so that immune cells have the necessary energy to mount a strong response, and also because the virus needs the sugar to replicate.”
According to researchers at the State Key Laboratory of Virology at Wuhan University, the hexosamine biosynthesis pathway — a glucose metabolism pathway — is responsible for activating IRF5-induced cytokine production in cells and mice. The same pathway is also responsible for viral replication, they say.32,33,34 As reported by The Scientist:35
“Hexosamine biosynthesis starts with glucose and results in an end product called uridine diphosphate N-acetylglucosamine (UDP-GlcNAc) … Liu’s team now shows that O-GlcNAcylation of IRF5 is necessary for the transcription factor’s cytokine-producing activity …
The team also showed that patients infected with influenza have higher blood glucose levels and more O-GlcNacylation of IRF5 than healthy controls. Furthermore, blood glucose levels correlated tightly with levels of inflammatory cytokines.
The results show that ‘there is a connection [between] influenza virus infection, enhanced glucose metabolism and cytokine storm, all linked through O-GlcNAcylation of IFR-5,’ Mengji Lu, a virologist at the University Hospital Essen and a coauthor of the study, writes in an email to The Scientist …”
In a Science Advances press release, co-author Shi Liu states:36
“We believe that glucose metabolism contributes to various COVID-19 outcomes since both influenza and COVID-19 can induce a cytokine storm, and since COVID-19 patients with diabetes have shown higher mortality.”
Insulin Resistance Is the Real Pandemic
So, to summarize, the real pandemic here appears to be dysregulated glucose metabolism; in other words, insulin resistance, which is exceedingly prevalent in the U.S.37,38 Insulin resistance, in turn, is a diet-induced condition.
Specifically, processed foods — which are loaded with added sugars, processed grains and industrially processed omega-6 vegetable oils — are the primary culprits causing insulin resistance, Type 2 diabetes and obesity, and according to FoodNavigator.com,39 doctors are finally starting to talk about the food industry’s role in the COVID-19 pandemic.
“A cardiologist has blamed the food industry for ‘normalizing’ ultra-processed junk food as more evidence emerges suggesting poor diet is the root cause behind increased mortality from COVID-19,” FoodNavigator states, adding:40
“In light of the mounting evidence that obesity and poor diet increases the risk of a severe response to COVID-19 infection, medical professionals now want the public health message urgently updated. And this, they warn, means the food industry bracing itself for regulation, such as bans on advertising and taxes …
Dr. Aseem Malhotra, a London-based cardiologist, told the BBC that a Government and Public Health England failure to tell the public to change its diet would represent an act of ‘negligence and ignorance’ … For him, the pandemic highlighted that it was in the interest of everybody, including those in the food industry, to make sure the population was as healthy as possible.”
Malhotra stresses these views in his April 16, 2020, article41 “COVID-19 and the Elephant in the Room,” published in European Scientist. “Obesity and chronic metabolic disease is killing COVID-19 patients: Now is the time to eat real food,” he says. Indeed, if our public health agencies really want to save lives, it’s time to get onboard with nutrition.
“If this is not the time for Britain to reverse its epidemic of Type 2 diabetes, which as a single condition has been the most costly to the NHS [National Health Service], then when is?” Malhotra writes.42
“Healthcare systems were already overstretched before COVID-19 because of decades of maldistribution of resources due to ‘too much medicine’ combined [with] our collective failure to implement policy changes to address the root cause of diet related disease — the unavoidable junk food environment.
The government public health message enhanced by the media to stay at home, protect the NHS and save lives has been powerful and effective. Given the speed at which health markers for metabolic disease improve from dietary interventions, an equally strong if not more significant population health message should now be to ‘eat real food, protect the NHS and save lives.’
Such implementation backed by policy changes may not just save hundreds and potentially thousands of lives around the world in the coming months but given the high likelihood of another international viral pandemic in the next decade a healthier population and a subsequently more manageable health service will be much better equipped to handle what would then be a smaller mortality peak on the next occasion.”
Junk Food Industry Faces Increasing Pressure
This is timely, considering a Corporate Accountability report,43 announced44 April 21, 2020, highlights the “outsized role” of International Life Sciences Institute (ILSI), a junk food industry front group funded by Coca-Cola, plays in shaping nutritional policies around the globe. According to the Corporate Accountability press release:45
“Notable among the findings is that more than half of the 2020 Dietary Guidelines Advisory Committee — the body that informs both national nutrition policy and how Americans eat and drink — has ties to ILSI …
The food and beverage industry’s role in stymying public health policy and propagating junk science is also taking on new dimensions during today’s pandemic. The surge of diet-related disease behind one in five deaths annually, is putting hundreds of millions of people at high risk of severe illness from COVID19.
‘For decades, Coke, its competitors, and its surrogates like ILSI have trafficked in junk science, co-opted public officials, and bullied advocates like myself …’ said Dr. Esperanza Ceron … ‘But we won’t be silenced. Too much is at stake’ …
‘It’s time for Coke to put something more on ice than its soft drinks,’ said Corporate Accountability Research Director Ashka Naik, a co-author of the report.
‘Coke is telling investors it cares about public health on the one hand, but funds ILSI to block public health safeguards on the other. Its misleading of investors and consumers is a liability that will only grow.’
A resolution … calls on Coke to come clean with its shareholders about its public health harms and liabilities. It would require a public, independent audit of how the corporation is contributing to the crisis of diet-related disease, whether through its products, its marketing, its political interference, or junk science.”
Data Show COVID-19 Isn’t a Significant Threat
In the featured Fundamental Health podcast above, Dr. Paul Saladino interviews Dr. Kirk Parsley about the lifestyle factors that are contributing to the high COVID-19 caseload in the U.S.
Saladino cites findings46 showing that of the roughly 4,800 crew on the U.S. aircraft carrier USS Theodore Roosevelt, 660 had tested positive for SARS-CoV-2. (As of April 23, when all of the crew had reportedly been tested, 840 tested positive.47) However, as noted by Saladino and reported by Business Insider,48 60% were asymptomatic, meaning they had no symptoms. Only one crewmember has died,49 and as of April 23, none were in intensive care.50
Similarly, among the 3,711 passengers and crew onboard the Diamond Princess cruise ship, 712 (19.2%) tested positive for SARS-CoV-2, and of these 46.5% were asymptomatic at the time of testing. Of those showing symptom, only 9.7% required intensive care and 1.3% died.51
Military personnel, as you would expect, tend to be healthier than the general population. Still, the data from these two incidents reveal several important points to consider. First of all, it suggests that even when living in close, crowded quarters, the infection rate is rather low.
Only 17.5% of the USS Theodore Roosevelt crew got infected — slightly lower than the 19.2% of those onboard the Diamond Princess, which had a greater ratio of older people.
Second, fit and healthy individuals are more likely to be asymptomatic than not — 60% of naval personnel compared to 46.5% of civilians onboard the Diamond Princess had no symptoms despite testing positive.
Saladino and Parsley go on to discuss current pandemic response efforts, such as the recommendation (and in some areas mandate) to wear a face mask when venturing outside. Both are convinced wearing a bandana across your face is completely useless, for the simple fact that the virus is so small it can easily slip through the fabric.
Parsley also reviews the statistics as of April 21, 2020, using Worldometer data,52 showing only 1.7% of American COVID-19 cases require hospitalization, and of those an even smaller ratio will actually die. Is it really reasonable to shut down the entire country and place everyone under house arrest over a 1.7% hospitalization rate?
So-called “COVID-19 cases,” by the way, simply means people who have tested positive using an RT-PCR (reverse transcription polymerase chain reaction) test, which is used to diagnose an active infection by detecting the presence of SARS-CoV-2 genetic material.53
Mortality Rates Are Still Vastly Overestimated
The hospitalization is actually bound to be even lower than 1.7% in real life, seeing how few people have actually been tested. Preliminary findings54 published April 17, 2020, reveal the actual infection rate in Santa Clara County, California, is likely to be between 50- and 85fold higher than the number of confirmed cases.
This is based on seroprevalence data, meaning antibody testing. If you have antibodies against a particular pathogen, you’ve been exposed to it in the past, whether you developed symptoms or not, and you’re now immune to it.
Between April 3 and April 4, 3,330 Santa Clara county residents were tested for antibodies to SARS-CoV-2 using a lateral flow immunoassay. In an effort to ensure results were as accurate as possible, they were adjusted for test performance characteristics using three estimates:
Test manufacturer data
A sample of 37 positive and 30 negative controls tested at Stanford
A combination of both
According to the authors:55
“The unadjusted prevalence of antibodies to SARS-CoV-2 in Santa Clara County was 1.5% … and the population-weighted prevalence was 2.81% … Under the three scenarios for test performance characteristics, the population prevalence of COVID-19 in Santa Clara ranged from 2.49% … to 4.16% …
These prevalence estimates represent a range between 48,000 and 81,000 people infected in Santa Clara County by early April, 50-85-fold more than the number of confirmed cases.
Conclusions: The population prevalence of SARS-CoV-2 antibodies in Santa Clara County implies that the infection is much more widespread than indicated by the number of confirmed cases. Population prevalence estimates can now be used to calibrate epidemic and mortality projections.”
Randomized antibody tests done in New York show that upward of 20% of the population in New York have been infected, suggesting that the virus had spread far more widely than known.56
This is also strong support for a lower fatality rate as previous inaccurate PCR tests were only done on sick people and there was no idea how many in the population had been infected. Since more people are infected, this increases the denominator in the calculation and lowers the mortality rate calculation.
Blood Pressure Drugs May Worsen COVID-19
Making matters worse, the drugs routinely used to treat lifestyle-induced afflictions such as high blood pressure, diabetes and heart disease may also be contributing to adverse outcomes in patients with COVID-19. According to Reuters:57
“A disproportionate number of patients hospitalized by COVID-19 … have high blood pressure. Theories about why the condition makes them more vulnerable … have sparked a fierce debate among scientists over the impact of widely prescribed blood-pressure drugs.
Researchers agree that the life-saving drugs affect the same pathways that the novel coronavirus takes to enter the lungs and heart. They differ on whether those drugs open the door to the virus or protect against it …
The drugs are known as ACE inhibitors and ARBs … In a recent interview with a medical journal, Anthony Fauci — the U.S. government’s top infectious disease expert — cited a report showing similarly high rates of hypertension among COVID-19 patients who died in Italy and suggested the medicines, rather than the underlying condition, may act as an accelerant for the virus …
There is evidence that the drugs may increase the presence of an enzyme — ACE2 — that produces hormones that lower blood pressure by widening blood vessels. That’s normally a good thing.
But the coronavirus also targets ACE2 and has developed spikes that can latch on to the enzyme and penetrate cells … So more enzymes provide more targets for the virus, potentially increasing the chance of infection or making it more severe.
Other evidence, however, suggests the infection’s interference with ACE2 may lead to higher levels of a hormone that causes inflammation, which can result in acute respiratory distress syndrome, a dangerous build-up of fluid in the lungs. In that case, ARBs may be beneficial because they block some of the hormone’s damaging effects.”
This presents significant challenges for patients and doctors alike, as there’s currently no significant consensus on whether patients should discontinue the drugs. The Centre for Evidence-Based Medicine at the University of Oxford in England recommends switching to alternative blood pressure medicines in patients who have only mildly elevated blood pressure and are at high risk for COVID-19.
A paper in NEJM stressed the potential benefits of the drugs instead, saying patients should continue taking them. However, several of the scientists who wrote that paper have done “extensive, industry-supported research on antihypertensive drugs,” Reuters notes.
Dr. Kevin Kavanagh, founder of the patient advocacy group Health Watch USA, believes it would be unwise to allow scientists funded by the drug industry to give clinical directions at this time. “Let others without a conflict of interest try to make a call,” he said.58
Restore Insulin Sensitivity for Long-Term Risk Mitigation
If we want people to survive the next pandemic, whatever that might be, then improving public health has got to be the No. 1 priority going forward. Waiting for a drug cure or vaccine is a fool’s game.
Health care really needs to start emphasizing strategies known to improve overall health rather than throwing drugs at symptoms that don’t address the underlying causes. Robust immune function is necessary to effectively combat COVID-19, and the same is true for all other infectious disease.
When it comes to improving health, addressing insulin resistance is truly key, seeing how it’s a factor in virtually all chronic diseases. And, to do that, we need to dramatically cut down on processed foods.
As noted by Dr. Sandra Weber, president of the American Association of Clinical Endocrinologists, in The New York Times,59 “We know that if you do not have good glucose control, you’re at high risk for infection, including viruses and presumably this one [COVID-19] as well … [improving glucose control] would put you in a situation where you would have better immune function.”
For those who desire more in-depth understanding of how you can become metabolically flexible and eliminate insulin resistance, consider picking up a copy of my book, “Fat for Fuel.” It goes into far greater detail, providing a comprehensive program that will help optimize your metabolic flexibility and strengthen your immune system — both of which are crucial components of health and disease prevention.
In January 2022, House Oversight Committee Republicans released National Institutes of Health emails that show Drs. Anthony Fauci and Francis Collins led the effort to bury the lab leak theory, even though the consensus in early February 2020 was that the virus likely leaked from the Wuhan lab
Fauci and Collins appear to have participated in the creation of a Nature Medicine article that denied the possibility of a lab leak in Wuhan, arguing instead for a natural origin of the virus
The Nature Medicine article is a glaring example of propaganda being promoted as science, and of science in turn being used for political aims
Behavioral scientist Simon Ruda, cofounder of the British Behavioral Insights Team, unofficially known as the “Nudge Unit,” confirms that the British government has been using propaganda tactics to scare the public into complying with COVID rules
Using behavioral science to manipulate people to achieve political goals is fundamentally anti-democratic
January 12, 2022, “Rising” cohost Ryan Grim reviewed the content of the National Institutes of Health emails released by the House Oversight Committee Republicans. According to Grim, the emails:
“… paint a damning picture of U.S. government officials wrestling with whether the novel coronavirus may have leaked out of a lab they were funding, deciding that it may very well have, and then actively suppressing those questions.”
What this latest cache of emails reveal is that February 1, 2020, Dr. Anthony Fauci, director of the National Institutes of Allergy and Infectious Diseases (NIAID), his boss, then-NIH director Dr. Francis Collins and at least 11 other scientists joined a conference call, during which they were told the SARS-CoV-2 virus might have leaked from the Wuhan Institute of Virology in Wuhan, China, and that it might have been genetically engineered.
What Was Said During the Secret Conference Call?
The next day, Dr. Jeremy Farrar, director of the Wellcome Trust, circulated a set of notes, summarizing the discussion. Mike Farzan, the scientist who discovered the SARS receptor, had reportedly stated that while the receptor binding domain (RBD) did not look engineered to him, he was bothered by the furin site.
According to Farrar’s note, Farzan “has a hard time explain[ing] that as an event outside the lab.” Farrar’s summary goes on to state that:
“… the likely explanation could be something as simple as passage SARS-live CoVs in tissue culture on human cell lines (under BSL-2) for an extended period of time, accidentally creating a virus that would be primed for rapid transmission between humans via gain of furin site (from tissue culture) and adoption to human ACE2 receptor via repeated passage …
So, I think it becomes a question of how do you put all this together, whether you believe in this series of coincidences, what you know of the lab in Wuhan, how much could be in nature — accidental release or natural event? I am 70:30 or 60:40.”
A note from professor and microbiologist Robert (Bob) Garry, Ph.D.,1 reads:
“Before I left the office for the ball, I aligned the nCoV with the 96% bat CoV sequenced at WIV. Except for the RBD the S proteins are essential identical at the amino acid level — well all but the perfect insertion of 12 nucleotides that adds [sic] the furin site.
S2 is over its whole length essentially identical. I really can’t think of a plausible natural scenario where you get from the bat virus or one very similar to it to nCoV where you insert exactly 4 amino acids 12 nucleotide [sic] that all have to be added at the exact same time to gain this function — that and you don’t change any other amino acids in S2?
I just can’t figure out how this gets accomplished in nature. Do the alignment of the spikes at the amino acid level — its [sic] stunning. Of course, in the lab it would be easy to generate the perfect 12 base insert that you wanted.
Another scenario is that the progenitor of nCoV was a bat virus with the perfect furin cleavage site generated over evolutionary times. In this scenario RaTG13 the WIV virus was generated by a perfect deletion of 12 nucleotides while essentially not changing any other S2 amino acid [sic]. Even more implausible IMO. That is the big if.”
Politics Overrode Scientific Consensus
So, in the earliest days of February 2020, the general consensus was that a WIV lab leak was a plausible scenario, and perhaps the most likely. However, politics rapidly entered the scene.
In a February 2, 2020, email, Collins stated that he was “coming around to the view that a natural origin is more likely,” and warned that “voices of conspiracy will quickly dominate” lest they convene a panel of experts to address the matter, and that such conspiracies could do “great potential harm to science and international harmony.”
Two days later, Fauci and Collins received a draft of the article, “The Proximal Origin of SARS-CoV-2,” later published in Nature Medicine.2 As noted by Grim, the actual draft is secret. All we have is an email reply from Fauci, in which he appears to flag or object to the inclusion of serial passage through humanized mice. Serial passaging is only briefly touched upon in the published article, which states:
“Furthermore, a hypothetical generation of SARS-CoV-2 by cell culture or animal passage would have required prior isolation of a progenitor virus with very high genetic similarity, which has not been described.
Subsequent generation of a polybasic cleavage site would have then required repeated passage in cell culture or animals with ACE2 receptors similar to those of humans, but such work has also not previously been described.”
If Fauci and Collins edited this article, “this is where they put the pressure of their pen the heaviest,” Grim says. Essentially, the issue of animal passage is raised, but then immediately dismissed.
Overall, the Nature Medicine article roundly dismissed the idea that the virus originated in a lab, proposing instead that, despite a dearth of evidence, it must have evolved naturally. The article didn’t stem the flow of questions, though. In a mid-April 2020 email to Fauci, Collins decried the continuation of the lab leak theory:
“Wondering if there is something NIH can do to help put down this very destructive conspiracy, with what seems to be growing momentum … I hoped the Nature Medicine article on the genomic sequence of SARS-CoV-2 would settle this. But probably didn’t get much visibility. Anything more we can do? Ask the National Academy to weigh in?”
Fauci replied, “I would not do anything about this right now. It is a shiny object that will go away in times [sic].” He was wrong, of course, and the reason questions didn’t go away was because emerging evidence kept strengthening the lab leak theory, while there is nothing with which to support natural evolution.
The COVID Propaganda Wars
The Nature Medicine article is a glaring example of propaganda being promoted as science, and of science in turn being used for political aims. There’s really nothing scientific about dismissing a valid origin hypothesis in order to maintain “international harmony.”
Of course, the entire COVID pandemic has been plagued by propaganda. Behavioral scientist Simon Ruda, cofounder of the British Behavioral Insights Team, unofficially known as the “Nudge Unit,” confirms that the British government has been using propaganda tactics to scare the public into complying with COVID rules.
According to Ruda, fear tactics such as an overemphasis on flawed models were initially deployed to secure compliance during the first lockdown. However, it then never ended. “That fear seems to have subsequently driven policy decisions in a worrying feed-back loop,” he wrote in a January 13, 2022, Unherd article.3 He goes on to state:
“I remain a supporter of the use of behavioral science in public policy, and of the Behavioral Insights Team, more commonly known as the Nudge Unit. However, witnessing how the UK and other governments have responded to the pandemic, I can now appreciate the vulnerabilities of well-intentioned, democratic regimes, and the potential for behavioral science to be used inappropriately …
In 2010, the Nudge Unit was the first and only government unit dedicated to behavioral science in public policy. By 2021, there were over 400 globally …
We advocated two new dimensions to policy making: behavior-focused models describing what drives human decision making; and the priority of empirical research over all other sources of information.
I believe this contribution has — and can — continue to serve governments well. But it must be used appropriately. For me, it means seeing the bigger picture: recognizing what you can and can’t measure, and seeing the potential for unintended consequences …
[I]nvoking different emotions to convince people to stay at home during the pandemic4is less appropriate. It could have negative consequences that are missed in the typical RCT evaluation.
This is because metrics will focus on proxies for behavior, but they probably can’t capture the potential longer-term effects of these campaigns beyond what is immediately measurable — such as worse inter-societal relations and reduced trust in institutions, the consequences of which could be significant …
In my mind, the most egregious and far-reaching mistake made in responding to the pandemic has been the level of fear willingly conveyed on the public …
Though I don’t think it’s fair to blame behavioral scientists for propagating fear (I suspect that this was more to do with Government communicators and the incentives of news broadcasters), it may be worth reflecting on where we need to draw the line between the choice-maximizing nudges of libertarian paternalism, and the creeping acceptance among policy makers that the state should use its heft to influence our lives without the accountability of legislative and parliamentary scrutiny.
Nudging made subtle state influence palatable, but mixed with a state of emergency, have we inadvertently sanctioned state propaganda?”
As noted by Ruda, it’s become quite clear over the past two years that we cannot rely on science or data alone in a pandemic. We also need “reflection, reason and debate … multidisciplinary teams” and “a strong culture of intellectual humility and designed-in cognitive diversity.”
Behavioral Science Has No Place in a Democracy
In his piece, Ruda acknowledges some of the criticism the Nudge Unit has received since its inception in 2010. But while Ruda still believes there’s a place for behavioral science in government, others say no way. In a January 14, 2022, Spiked article,5 Professor Emeritus of sociology Frank Furedi insists that “government’s use of behavioral science violates our freedom to judge and act for ourselves.”
“Ruda’s admission is … striking,” Furedi writes, adding that Ruda “even expressed concern about the state’s willingness ‘to use its heft to influence our lives without the accountability of legislative and parliamentary scrutiny.’”
Furedi goes on to cite a March 2020 paper by the Scientific Pandemic Influenza Behavior Advisory Committee, written on behalf of the U.K. government’s Scientific Advisory Group for Emergencies (SAGE), in which they stated that the people were “too relaxed about the pandemic.” Furedi writes:6
“‘A substantial number of people still do not feel sufficiently personally threatened,’ it stated, adding that too many ‘are reassured by the low death rate in their demographic group.’
It then urged the government to increase ‘the perceived level of personal threat… among those who are complacent, using hard-hitting emotional messaging.’ Some members of SAGE have since reported feeling ’embarrassed’ by the nature of SPI-B’s advice. As one regular SAGE attendee put it last year:
‘The British people have been subjected to an unevaluated psychological experiment without being told that is what’s happening.’
It is to be welcomed that at least some behavioral scientists are now questioning the political use of their discipline. But the problem goes deeper than fear-mongering during the pandemic. We need to address the corrosive influence of behavioral science on public life in general.”
Furedi stresses that the principal problem with “nudging” is that this kind of behavioral science is “fundamentally anti-democratic.” It’s based on the assumption that people “cannot be trusted to make rational choices,” and therefore must be subject to management by bureaucrats.
“They treat people’s emotional lives, lifestyles and relationships as legitimate objects of policymaking and professional intervention,” Furedi writes, adding that “This politics of behavior has given rise to a new form of technocratic governance.”
Indeed, over the past two years, subliminal psychological manipulation has near-universally replaced debate and discussion. The problem is that you cannot have a democracy without open debate. What we have now is, in fact, a technocratic form of governance, whether people realize it or not, and unless we pull the plug, there soon won’t be such a thing as democracy anywhere in the world.
‘Nudging’ Is Fundamentally Anti-Democratic
“When Britain’s then deputy prime minister, Nick Clegg, casually remarked in 2010 that the Nudge Unit could change the way citizens think, he spoke like a totalitarian ruler. Since when was it within a democratic government’s mandate to try to manipulate and change its citizens’ thoughts?” Furedi asks.
He points to a report called “Mindspace: Influencing Behavior Through Public Policy,”7 written by the U.K. Cabinet Office and the Institute for Government and published in 2010, in which they reveal and basically admit that the use of behavioral psychology in policymaking “deprives people of the power to democratically determine their future,” Furedi says.
The report actually presents this kind of government activity as a form of “surrogate willpower,” which on its face shows that individual freedom is not honored or even taken seriously. Instead, government is actively trying to make our decisions for us, in large part by indoctrinating us with certain “values” and ideas that we might not naturally share or agree with.
At the end of the day, whether behavioral psychologists get things “right” or “wrong,” they are violating people’s freedom to make their own decisions all the same, and as noted by Furedi:8
“This threatens the very pre-condition for a flourishing, democratic public life — namely, the existence of morally autonomous individuals. After all, it is only through the making of choices that people develop a sense of responsibility for themselves and for others in society.
As our experience of the pandemic shows, we need to respect the common sense of citizens and allow them to make choices in line with their circumstances … Our minds must be a no-go area for these self-appointed high priests of the soul.”
Weaponizing Behavioral Science
The danger of behavioral science is also in full display when we look at how it’s being weaponized against the very public it claims to serve. It started with people who refused to buy into the propaganda being labeled as “anti-science conspiracy theorists” and “anti-vaxxers.” Now, those same people are being labeled as terrorists and targeted by national security agencies.
“Concern for U.K. Security as Anti-Vaxxer Groups Evolve Toward U.S.-Style Militias,” a headline in The Guardian9 declared in mid-January 2022. “Counter-terrorism officials are monitoring movement amid military-style training and lurch towards violent extremism.” According to this report, such individuals might “undermine national health security.”
In other words, “health” itself has now been weaponized. The national vaccination program equates to “national security,” and sharing information that might cause vaccine hesitancy equates to an act of domestic terrorism. It’s ridiculous, of course, but that doesn’t make it any less serious.
The Davos Agenda
Between January 17 and 21, 2022, the World Economic Forum hosted its annual meeting in Davos, where the top technocrats in the world meet to hatch and share the next steps in the technocratic takeover of the world.
WEF founder Klaus Schwab opened the Forum’s virtual Davos agenda by introducing Chinese dictator Xi Jinping, general secretary of the Chinese Communist Party since 2012 and president of the People’s Republic of China since 2013.
Schwab’s short introduction makes it clear that this dictatorship is being looked to for inspiration and leadership as The Great Reset moves forward. Perhaps we shouldn’t be surprised that Fauci and Collins were more concerned about “international harmony” than getting to the bottom of where SARS-CoV-2 came from.
Using the Chinese model of behavior modification and social engineering through technological surveillance and coercion, the WEF and its global allies aim to:
Continue the building of a global biosecurity state in the name of fighting the COVID pandemic
“Revitalize the global economy and accelerate its transition to net zero”
“Preserve biodiversity by deploying nature-based solutions”
“Narrow the gap between the rich and the poor to achieve more sustainable global development”
Anyone familiar with technocracy will recognize what a pile of manure this is. Without understanding what these goals entail, they might sound good, but in reality, this agenda is a call to war against humanity as we know it.
More than 35 million Americans are on a statin drug, making it one of the most commonly prescribed medicines in the U.S. Lipitor — which is just one of several brand name statin drugs — is one of the most profitable drugs in the history of medicine
The “statin empire” is built on prescribing these drugs to people who really don’t need them and are likely to suffer side effects without getting any benefits
By simply revising the definition of “high cholesterol,” which was done in 2000 and again in 2004 in the U.S., millions of people became eligible for statin treatment, without any evidence whatsoever that it would actually benefit them
In 2013, the American College of Cardiology and AHA revised their statin guideline to include a CVD risk calculation rather than a single cholesterol number. This resulted in another 12.8 million Americans being put on statin treatment even though they didn’t have any real risk factors for CVD
Industry-biased research, the hiding of raw study data, deceptive statistical tricks, silencing of dissenters, censoring of critics and the use of fear-based PR are other strategies employed to manipulate public opinion and doctors to keep prescribing statins to an ever-widening population base
This article was previously published March 11, 2020, and has been updated with new information.
Statins are HMG-CoA reductase inhibitors; that is, they block the enzyme in your liver responsible for making cholesterol (HMG-CoA reductase). According to Drugs.com, more than 35 million Americans are on a statin drug, making it one of the most commonly prescribed medicines in the U.S.1
National Health and Nutrition Examination Survey data suggest 47.6% of seniors over the age of 75 are on a statin drug.2 Lipitor — which is just one of several brand name statin drugs — is one of the most profitable drugs in the history of medicine.3,4
Collectively, statins have earned over $1 trillion since they were introduced.5 This, despite their being off patent. There is simply no doubt that selling them is big business with major financial incentives to distort the truth to continue their sales.
Statin recommendations have become fairly complex, as they’re recommended for various age groups under different circumstances, and whether they’re used as primary prevention of cardiovascular disease (CVD), or secondary prevention. Guidelines also vary slightly depending on the organization providing the recommendation and the country you’re in.6
In the U.S., the two guidelines available are from the U.S. Preventive Services Task Force (USPSTF),7 and the American College of Cardiology and American Heart Association.8,9 The USPSTF guidelines recommend using a statin for the primary prevention of CVD when a patient:10
Is between the age of 40 to 75
Has one or more CVD risk factors (dyslipidemia, diabetes, hypertension or smoking)
Has a calculated 10-year risk of a cardiovascular event of 10% or greater
In secondary prevention of CVD, statins are “a mainstay,” according to the Journal of the American College of Cardiology.11 Secondary prevention means the drug is used to prevent a recurrence of a heart attack or stroke in patients who have already had one.
Regulators’ Role Questioned
A February 2020 analysis12 in BMJ Evidence-Based Medicine (paywall) brings up the fact that while the use of statins in primary prevention of CVD “has been controversial” and there’s ongoing debate as to “whether the benefits outweigh the harms,” drug regulators around the world — which have approved statins for the prevention of CVD — have stayed out of the debate. Should they? The analysis goes on to note:
“Our aim was to navigate the decision-making processes of European drug regulators and ultimately request the data upon which statins were approved. Our findings revealed a system of fragmented regulation in which many countries licensed statins but did not analyze the data themselves.
There is no easily accessible archive containing information about the licensing approval of statins or a central location for holding the trial data. This is an unsustainable model and serves neither the general public, nor researchers.”
Have We Been Misled by the Evidence?
In her 2018 peer-reviewed narrative review,13 “Statin Wars: Have We Been Misled About the Evidence?” published in the British Journal of Sports Medicine, Maryanne Demasi, Ph.D., a former medical science major turned investigative health reporter, delves into some of these ongoing controversies.
“A bitter dispute has erupted among doctors over suggestions that statins should be prescribed to millions of healthy people at low risk of heart disease. There are concerns that the benefits have been exaggerated and the risks have been underplayed.
Also, the raw data on the efficacy and safety of statins are being kept secret and have not been subjected to scrutiny by other scientists. This lack of transparency has led to an erosion of public confidence.
Doctors and patients are being misled about the true benefits and harms of statins, and it is now a matter of urgency that the raw data from the clinical trials are released,” Demasi writes.14
While Demasi’s paper is behind a paywall, she reviews her arguments in the featured video above. Among them is the fact that the “statin empire” is built on prescribing these drugs to people who really don’t need them and are likely to suffer side effects without getting any benefits.
For example, some have recommended statins should be given to everyone over the age of 50, regardless of their cholesterol level. Others have suggested screening and dosing young children.
Even more outrageous suggestions over the past few years include statin “‘condiments’ in burger outlets to counter the negative effects of a fast food meal,'” and adding statins to the municipal water supply.
Simple Tricks, Big Payoffs
Medical professionals are now largely divided into two camps, one saying statins are lifesaving and safe enough for everyone, and the other saying they’re largely unnecessary and harmful to boot. How did such a divide arise, when all have access to the same research and data?
Demasi suggests that in order to understand how health professionals can be so divided on this issue, you have to follow the money. The cost of developing and getting market approval for a new drug exceeds $2.5 billion. “A more effective way to fast-track company profits is to broaden the use of an existing drug,” Demasi says, and this is precisely what happened with statins.
By simply revising the definition of “high cholesterol,” which was done in 2000 and again in 2004, millions of people became eligible for statin treatment, without any evidence whatsoever that it would actually benefit them.
As it turns out, eight of the nine members on the U.S. National Cholesterol Education Program panel responsible for these revisions had “direct ties to statin manufacturers,” Demasi says, and that public revelation sowed the first seed of suspicion in many people’s minds.
Skepticism ratcheted up even more when, in 2013, the American College of Cardiology and AHA revised their statin guideline to include a CVD risk calculation rather than a single cholesterol number. U.S. patients with a 7.5% risk of developing CVD in the next 10 years were now put on a statin. (In the U.K., the percentage used was a more reasonable 20%.)
This resulted in another 12.8 million Americans being put on statin treatment even though they didn’t have any real risk factors for CVD. Worse, a majority of these were older people without heart disease — the very population that stand to gain the least from these medications.
What’s worse, 4 of 5 calculators were eventually found to overestimate the risk of CVD, some by as much as 115%, which means the rate of overprescription was even greater than previously suspected.
Industry Bias
While simple revisions of the definitions of high cholesterol and CVD risk massively augmented the statin market, industry-funded studies have further fueled the overprescription trend. As noted by Demasi, when U.S. President Ronald Reagan cut funding to the National Institutes of Health, private industry moved in to sponsor their own clinical trials.
The vast majority of statin trials are funded by the manufacturers, and research has repeatedly found that funding plays a major role in research outcomes. It’s not surprising then that most statin studies overestimate drug benefits and underestimate risks.
Demasi quotes Dr. Peter Gøtzsche, a Danish physician-researcher who in 1993 co-founded the Cochrane Collaboration and later launched the Nordic Cochrane Centre:
“When drug industry sponsored trials cannot be examined and questioned by independent researchers, science ceases to exist and it becomes nothing more than marketing.”
“The very nature of science is its contestability,” Demasi notes. “We need to be able to challenge and rechallenge scientific results to ensure they’re reproducible and legitimate.” However, there’s been a “cloud of secrecy” around clinical statin trials, Demasi says, as the raw data on side effects have never been released to the public, nor other scientists.
The data are being held by the Cholesterol Treatment Trialists (CTT) Collaboration at CTSU Oxford, headed by Rory Collins, which periodically publishes meta-analyses of the otherwise inaccessible data. While the CTT claims to be an independent organization, it has received more than £260 million from statin makers.
Inevitably, its conclusions end up promoting wider use of statins, and no independent review is possible to contest or confirm the CTT Collaboration’s conclusions.
Tricks Used to Minimize Harms in Clinical Trials
As explained by Demasi, there are many ways in which researchers can influence the outcome of a drug trial. One is by designing the study in such a way that it minimizes the chances of finding harm. The example she gives in her lecture is the Heart Protection Study.
Before the trial got started, all participants were given a statin drug for six weeks. By the end of that run-in period, 36% of the participants had dropped out due to side effects or lack of compliance. Once they had this “freshly culled” population, where those suffering side effects had already been eliminated, that’s when the trial actually started.
Now, patients were divided into statin and placebo groups. But since everyone had already taken a statin before the trial began, the side effects found in the statin and placebo groups by the end of the trial were relatively similar.
In short, this strategy grossly underestimates the percentage of the population that will experience side effects, and this “may explain why the rate of side effects in statin trials is wildly different from the rate of side effects seen in real-world observations,” Demasi says.
Deception Through Statistics
Public opinion can also be influenced by exaggerating statistics. A common statistic used to promote statins is that they lower your risk of heart attack by about 36%.15 This statistic is derived from a 2008 study16 in the European Heart Journal. One of the authors on this study is Rory Collins, who heads up the CTT Collaboration.
Table 4 in this study shows the rate of heart attack in the placebo group was 3.1% while the statin group’s rate was 2% — a 36% reduction in relative risk. However, the absolute risk reduction — the actual difference between the two groups, i.e., 3.1% minus 2% — is only 1.1%, which really isn’t very impressive.
In other words, in the real world, if you take a statin, your chance of a heart attack is only 1.1% lower than if you’re not taking it. At the end of the day, what really matters is what your risk of death is the absolute risk. The study, however, only stresses the relative risk (36%), not the absolute risk (1.1%).
As noted in the review,17 “How Statistical Deception Created the Appearance That Statins Are Safe and Effective in Primary and Secondary Prevention of Cardiovascular Disease,” it’s very easy to confuse and mislead people with relative risks. You can learn more about absolute and relative risk in my 2015 interview with David Diamond, Ph.D., who co-wrote that paper.
Silencing Dissenters and Fear-Based PR
Yet another strategy used to mislead people is to create the illusion of “consensus” by silencing dissenters, discrediting critics and/or censoring differing views.
In her lecture, Demasi quotes Collins of the CTT Collaboration saying that “those who questioned statin side effects were ‘far worse’ and had probably ‘killed more people’ than ‘the paper on the MMR vaccine'” … “Accusing you of murdering people is an effective way [to] discredit you,” she says.
Demasi also highlights the case of a French cardiologist who questioned the value of statins in his book. It received widespread attention in the French press, until critics started saying the book and resulting press coverage posed a danger to public health.
One report blamed the book for causing a 50% increase in statin discontinuation, which was predicted would lead to the death of 10,000 people. On this particular occasion, however, researchers analyzed the number of actual deaths based on national statistics, and found the actual death toll decreased in the year following the release of the book.
The authors, Demasi says, noted that it was “‘not evidence-based to claim that statin discontinuation increases mortality,’ and that in the future, scientists should assess ‘real effects of statin discontinuation rather than making dubious extrapolations and calculations.'”
Trillion-Dollar Business Based on Flimsy Evidence
Statins, originally introduced three decades ago as secondary prevention for those with established CVD and patients with congenital and familial hyperlipidemias, have now vastly expanded thanks to the strategies summarized above.
Tens if not hundreds of millions of people are now on these drugs, without any scientific evidence to show they will actually benefit from them. As noted in the EBM analysis, “Statins for Primary Prevention: What Is the Regulator’s Role?”:18
“The central clinical controversy has been a fierce debate over whether their benefits in primary prevention outweigh their harms … The largest known statin usage survey conducted in the USA found that 75% of new statin users discontinued their therapy by the end of the first year, with 62% of them saying it was because of the side effects.
Regardless of what level of prevention statin prescription is aimed at, the proposed widening of the population to over 75s de facto includes people with multiple pathologies, whether symptomatic or not, and bypasses the distinction between primary and secondary prevention …
The CTT Collaboration estimates the frequency of myopathy is quite rare, at five cases per 10,000 statin users over five years. But others have contended that the CTT Collaboration’s work ‘simply does not match clinical experience’ … [Muscle-related adverse events] reportedly occur with a frequency of … as many as 20% of patients in clinical practice.”
Regulators Have a Duty to Create Transparency
Considering the discrepancy in reported side effects between statin trials, clinical practice and statin usage surveys, what responsibility do regulators have?
According to “Statins for Primary Prevention: What Is the Regulator’s Role?”19 regulators have a responsibility to “engage and publicly articulate their position on the controversy and make the evidence base underlying those judgments available to third parties for independent scrutiny,” none of which has been done to date. The paper adds:
“Regulators holding clinical trial data, particularly for public health drugs, should make these data available in searchable format with curated and dedicated web-based resource. If national regulators are not resourced for this, pooling or centralizing resources may be necessary.
The isolation of regulators from the realities of prescribing medications based on incomplete or distorted information is not enshrined in law but is a product of a subculture in which commercial confidentiality is more important than people. This also needs to change.”
Do Your Homework Before Taking a Statin
There’s a lot of evidence to suggest drug company-sponsored statin research and its PR cannot be trusted, and that few of the millions of people currently taking these drugs actually benefit from them.
Some of the research questioning the veracity of oft-cited statin trials is reviewed in “Statins’ Flawed Studies and Flawed Advertising” and “Statins Shown to Extend Life by Mere Days.”
To learn more about the potential harms of statins, see “Statins Double Diabetes Rates,” “Statins Trigger Brain Changes With Devastating Effects,” and “5 Great Reasons You Should Not Take Statins.”
In a non-peer-reviewed research paper just this week published, Stephanie Seneff, Ph.D., describes a mechanism of the COVID shots that results in the suppression of your innate immune system. It does this by inhibiting the type-1 interferon pathway
The COVID jab can cause neurons in your brain to produce toxic spike protein, or take up circulating spike protein, and the neurons try to eliminate the spike protein by transmitting them through exosomes. The exosomes are picked up by microglia, immune cells in your brain, which activate an inflammatory response, which can contribute to degenerative brain disorders
Two microRNAs, miR-148a and miR-590, are central in this process. These microRNAs — excreted in the exosomes along with the spike protein — significantly disrupt the type-1 interferon response in any cell, including immune cells
On average, there are twice as many reports of cancer following the COVID shots compared to all other vaccines combined over the last 31 years
The fact that the signal is that strong is even more remarkable when you consider that most people don’t think the COVID shot could be a variable in their cancer emergence, so they never report it
In this interview, return guest Stephanie Seneff, Ph.D., a senior research scientist at MIT who has been at MIT for over five decades, discusses her latest paper, “Innate Immune Suppression by SARS-CoV-2 mRNA Vaccinations. The Role of G-quadruplexes, Exosomes and MicroRNAs,” co-written with Dr. Peter McCullough, along with two other authors, Dr. Greg Nigh and Dr. Anthony Kyriakopoulos.
Previously, Nigh and Seneff co-wrote an entire paper detailing the differences between the spike protein and the COVID jab spike protein. In a non-peer-reviewed research paper just this week published on the pre-print service authorea, they and their other co-authors delve deeply into the mechanisms of the COVID shots, showing how they absolutely, in no way, shape or form, are safe or effective. The shots actually suppress your innate immune system.
“I think McCullough is fantastic and I’m so happy to have him collaborate with me,” Seneff says. “I really hope we will be able to find a journal that is willing to publish it. We may have to seek some kind of alternative media to get it published.
It’s really incredible the amount of censorship that’s going on right now. I’m in a state of shock all the time. I just keep thinking it’s not going to get any worse, and it’s truly going to get better, and it just seems to keep on getting worse and worse.
I don’t know where the end is. It’s very discouraging … Pharma has so much money behind [them] and they’ve got it all set up to make sure that nothing gets past them …
We’re hoping to put it up as a preprint, but … remarkably, they can reject it at the level of preprint as well. We’re working on that angle, but it’s not easy. When you’re writing something this radical, they really fight hard to keep it off the web.”
On January 16, 2022, the pre-print service Authorea published this paper on its web site, assigning it a DOI, thus making it official.
Exceptionally Strong Safety Signals
As noted by Seneff, when you look at the various databases for adverse effects, you can see an exceptionally strong safety signal — and the COVID shot developers know that. “The numbers are out of sight,” Seneff says, and this goes for all levels of side effects, from mild to catastrophic.
Seneff has been looking at the cancer data, for example, and on average, there are twice as many reports of cancer following the COVID shots compared to all other vaccines combined over the last 31 years.
“It’s just amazing, because it’s overall two times [higher]. Breast cancer, for example, is three times [higher] for these vaccines in one year, as they are for all the other vaccines for 31 years. It’s a hugely strong signal,” Seneff says.
“Lymphoma is also showing up much more frequently with these [COVID shots]. There’s just an amazing signal there in VAERS [the U.S. Vaccine Adverse Events Reporting System].”
The fact that the signal is that strong is even more remarkable when you consider that most people don’t think the COVID shot could be a variable in their cancer emergence, so they never report it. “It puzzles me that they’re willing to do such damage to the health of the whole population of the world. I don’t understand that degree of evilness,” Seneff says.
Type-1 Interferon Disruption
The shots suppress your innate immune system by inhibiting type-1 interferon. One of the first studies to tip off Seneff and McCullough to this was an Indian study, in which human cells grown in a culture were exposed to the DNA nanoparticles that instruct them to make SARS-CoV-2 spike protein, much like the COVID shots do.1
The cell strain is called HEK-293. These are cells that were taken from the kidneys of an aborted fetus in the 1980s and are frequently used in research. While taken from the kidneys, these cells have neuron-like properties. When programmed to make spike protein, these cells release that spike protein inside exosomes — lipid nanoparticles inside which the spike protein is packaged.
Exosomes act as a communication network for cells. When a cell is under stress, it releases exosomes containing some of the molecules that are stressing it. So, in the case of the COVID shots, the exosomes contain spike protein and microRNA. MicroRNAs are signaling molecules that are able to influence cell function. They cause the cell to change its behavior or metabolism. Typically, they do this by suppressing certain enzymes.
The Indian study found two specific microRNAs inside the exosomes released by these neuron-like cells: miR-148a and miR-590. The researchers then exposed microglia (immune cells in your brain) to these exosomes. So, as explained by Seneff, you’ve got neurons in your brain producing spike protein, or taking up spike protein that is in circulation, and reacting to it by releasing exosomes.
The exosomes are then picked up by microglia, the immune cells in your brain. When the immune cells receive those exosomes, they turn on an inflammatory response. This is primarily a response to those microRNAs, the miR-148a and miR-590. Of course, you also have the toxic spike protein there.
Combined, they cause inflammation in the brain, which damages neurons. This inflammation, in turn, can contribute to a number of degenerative brain disorders. The lipid particles in the COVID shot, which contain the mRNA, are similar to exosomes, but not identical. They’re also very similar to low-density lipid (LDL) particles.
“I think the exosomes are probably quite a bit smaller. The vaccine particles are bigger. They’re more like an LDL particle. The vaccine particles have cholesterol in their membrane, and they have lipoprotein. So, they’re made to look like an LDL particle.
But then they throw in this cationic lipid, which is really, really toxic — a synthetic cationic lipid that makes it positively charged. Experimentally, they’ve found that this lipid, when the particle is taken up by the cell, is released into the cytoplasm, [where] that mRNA then makes spike protein.
[The COVID shots] are very cleverly designed, both in terms of protecting the RNA from getting broken down, and in terms of making the RNA be very efficient at making spike protein. It’s very different from the mRNA that the virus makes, even though it codes for the same protein.”
Seneff wrote an entire paper2 detailing the differences between the viral spike protein and the COVID jab spike protein, together with Greg Nigh, which was published in the International Journal of Vaccine Theory, Practice and Research in May 2021. It basically serves as a primer for understanding what we discuss here.
Getting back to the Indian paper cited above, they found that the microglia ended up producing inflammation in the brain, and the two microRNAs were central in this process. The miR-148a and miR-590 were put into those exosomes with the spike protein, and these two microRNAs are able to significantly disrupt the type-1 interferon response in any cell, including immune cells.
Type-1 interferon also keeps latent viruses like herpes and varicella (which causes shingles) viruses in check, so if your interferon pathway is suppressed, these latent viruses can also start to emerge. The VAERS database reveals many who have been jabbed do report these kinds of infections. Suppressed interferon also raises your risk of cancer and cardiovascular disease.
Type-1 Interferon Response Is Crucial in Viral Infections
As explained by Seneff, the type-1 interferon response is absolutely crucial as the first-stage response to a viral infection. When a cell is invaded by a virus, it releases type-1 interferon alpha and type-1 interferon beta. They act as signaling molecules that tell the cell that it’s been infected.
That, in turn, launches the immune response and gets it going early in the viral infection. It’s been shown that people who end up with severe SARS-CoV-2 infection have a compromised type-1 interferon response. As noted by Seneff:
“It’s ironic that the vaccines are being given to protect you from COVID, yet, they produce a situation where your immune cells are ill-equipped to fight SARS-CoV-2 if it gets into the cell. The trick is, the vaccine produces a tremendous antibody response, and that’s typical of severe disease.
So, the [COVID shot] fools your immune system into thinking that you’ve had a severe case of COVID. It’s really interesting that way, because it’s gotten past the mucosal barrier of the lungs, it’s gotten past the vascular barrier of the blood, into the muscle. Also, it’s been disguised.
The RNA doesn’t look like a virus RNA, it looks like a human RNA molecule. Part of the modifications [made to the mRNA in the jab] was to make it very sturdy, so it can’t be broken down. It’s also very good at making [spike] protein fast, which also has a problem because it leads to a lot of errors, which is another issue …
The immune cells take up the nanoparticles and carry them through the lymph system into the spleen. Multiple studies have shown that it ends up in the spleen … the ovaries, the liver, the bone marrow … The spleen, of course, is very important for producing antibodies.”
Importantly, the antibody response you get from the COVID shot is exponentially higher than what you get from natural infection, and research has shown that the level of antibody response rises with disease severity. So, the shot basically mimics severe infection. In mild infection, you may not produce any antibodies at all, because the innate immune cells are strong enough to fight off the infection without them.
It’s when your innate immune system is weak that you get into trouble, and part of that weakness is a suppressed type-1 interferon response. If your type-1 interferon response is deficient, your immune cells are not very capable of stopping the spread of the virus in your body.
According to Seneff, the reason type-1 interferon supplementation has not been recommended thus far is because you have to time it perfectly in order for the immune cascade to function properly. Type-1 interferon plays a definitive role only at the very earliest stage of the infection. Once you’ve entered a moderate or severe infection stage, it’s too late to use it.
COVID Shots Confuse Your Immune System
As noted by Seneff, the COVID shots are so unnatural that your immune system doesn’t quite know what to do anymore.
“My impression is that the immune cells don’t know what the hell’s going on. There’s this toxic protein being produced in massive amounts by the immune cells. That’s extremely unusual. There’s no sign of any kind of viral infection because these RNAs look like human RNAs.
It’s as if the human immune cells suddenly decided to make a really toxic protein, and make lots of it — which is exactly what they’re doing — and the immune system is completely baffled by this. The immune cells have no clue what to do with it.
Of course, these immune cells that are overloaded with all this spike protein, they say, ‘I’ve got to get rid of this stuff,’ so they ship it out as these exosomes. The microRNAs [in the exosomes] think that the recipient cells are going to need those particular signaling molecules to help it do whatever it needs to do to cope with this toxic load.
So, you’re spreading the spike protein around to the rest of the body, just to dissipate the toxicity you’re coping with in the spleen, I think. Those exosomes are also very good for training antibodies. There was a nice paper that showed the exosomes being released [have] spike protein in their membrane, the exterior of the exosome.
It’s quite cool that the spike protein is displayed there, because this allows the immune cells — the B-cells and the T-cells that need to get up close and personal to it — to figure out how to shape their antibodies. The antibodies get shaped to match the toxic protein that’s exposed on the surface of the exosomes.
After something like 14 days of the second [jab], the exosomes induced an antibody response. [The researchers] felt the exosomes played a critical role in this extreme antibody response that was produced by the B-cells and the T-cells, the adaptive immune system.
But I think the way the vaccine works is that there’s no game that you can choose other than to make antibodies. It’s the only way you can fight this. It’s a toxic protein that’s being produced and released by these immune cells, and the only thing you can do to stop it is to make antibodies.
They try to make lots and lots of antibodies that will glue onto those toxic spike proteins and block them from being able to get in through the ACE2 receptor. That’s the job of the antibodies. They do a good job of it, initially … It’s true that they do protect you from disease. Unfortunately, the antibody levels drop pretty dramatically, pretty quickly.”
There are also antibodies that enhance disease rather than fight it, and the level of these antibodies declines at a slower pace than the protective antibodies. So, after a number of months you end up with a NEGATIVE immune response. In other words, you’re now more prone to infection than ever before. As explained by Seneff:
“There’s a crossover point at which the enhancing antibodies can be stronger than the protective antibodies, and that’s when you can get this antibody dependent enhancement (ADE) that people have seen in the past with [other] coronavirus vaccines. We’re still trying to see if that’s the case with [the COVID jabs]. There is some evidence here and there, but it’s not [conclusive yet].”
The Importance of Cytotoxic T-Cells
After the India study tipped off Seneff and McCullough to the interferon problem, they came across a Chinese study3 that tracked the effect of the COVID jab on the immune system over time. Here, they discovered that the infection caused an increase in CD8+ T-cells, important cytotoxic T-cells that actually remove infected cells.
As noted by Seneff, the CD8+ cells are an important part of the defense against SARS-CoV-2. Importantly, CD8+ T-cells were enhanced in response to natural infection, but not in response to the COVID shot. They too found type-1 interferon suppression post-jab. So, in the aftermath of the jab, not only is your first-line response depressed — the type-1 interferon response — but you’re also missing the part of the immune response that cleans away infected cells.
The microRNA That Influences Myocarditis Risk
A third microRNA (mRNA) created by natural SARS-CoV-2 infection is miR-155, and it plays an important role in heart health. Early on in the pandemic, there were reports of COVID-19 causing heart problems.
Seneff suspects the miR-155-containing exosomes may also be present post-jab, and may play a role in the heart damage that’s being reported. Specifically, miR-155 is associated with myocarditis. As mentioned earlier, microRNA suppresses certain proteins that then cause a complicated cascade response. When a particular protein that is a critical player gets suppressed by a microRNA, then a whole different cascade takes place.
Why Autoimmune Problems May Arise Post-Jab
The antibodies produced by the jab also have several short peptide sequences in them that have previously been found in several human cells that are related to autoimmune disease. Seneff explains:
“Kanduc has written a lot about this. She’s an expert on these antibodies … The [SARS-CoV-2] spike protein is very overlapped with human protein. That means when you build a really strong antibody response to the spike protein, those antibodies can get confused and they can attack a human protein that has a similar sequence.
That’s a classic form of autoimmune disease. It’s called molecular mimicry. There were many different proteins that matched. It was quite surprising … It seems to be very well designed to induce autoimmune disease, if you produce antibodies to those sequences in the spike protein.”
Neurological Problems in Women
The shots are also tightly associated with neurological problems such as uncontrollable tremors and shaking. Curiously, this side effect disproportionally affects women. The mechanism here again involves the exosomes. Seneff explains:
“I feel there’s a very strong signal for the idea, which I’m pushing, that you have those immune cells in the spleen making spike protein and releasing it in exosomes. It’s been shown in studies on Parkinson’s disease that those exosomes travel along nerve fibers.
They’ll go along the splanchnic nerve, they’ll hook up with the vagus nerve, they’ll go up to the brain and get into all these different nerves in the brain. When you look at the VAERS database, you see tremendous signals for all kinds of things that suggest different nerves are being inflamed.
For example, there are 12,000 cases of tinnitus associated with the COVID-19 vaccine, and that’s only what’s reported. Tinnitus is a strong signal. Tinnitus is going to be inflammation of the auditory nerve. This means you have to go all the way from the spleen, up the vagus nerve, and then connect to the auditory nerve to cause tinnitus.
Then you have Bell’s palsy, which is inflammation of the facial nerve. You have migraine headache. There are over 8,000 cases of migraine headache, which is linked to an inflammation of the trigeminal nerve.
It probably also goes, I suspect, along the nerve fibers of the spinal column, which may be causing some of these cases where they’re finding paralysis. People have a lot of mobility issues connected with these vaccines.
I see the possibility of causing a lot of disturbances to the myelin sheath, and we talk about that in the paper. It involves, again, complex signaling. You can get to the myelin sheath problem through the type-1 interferon disruption.
That, again, involves something called interferon response factor 9 IRF9. This protein triggers the production of sulfatide in the liver, and this protein gets suppressed by these microRNAs that I mentioned earlier.”
Sulfatide, an important lipid carrier, is the only sulfonated lipid in the human body. Your liver makes most of the sulfatide, which is then carried by your platelets (blood cells) to other areas in your body. The myelin sheath contains high amounts of sulfatide. It’s part of what protects the myelin sheath. In demyelinating diseases, that sulfatide erodes, ultimately allowing the myelin to be attacked.4
Seneff believes the COVID jab results in significant myelin damage, thanks to these inflammatory exosomes. This damage does not necessarily show up right away, although some jab recipients experience acutely devastating effects. It could take 10 years or more before a demyelinating disease sets in.
“I think we’re going to see people getting these neurodegenerative diseases earlier and earlier in life than they used to,” Seneff says, “and I think anybody who already has any of these diseases is going to have accelerated progression.”
We May Soon See an Explosion of Parkinson’s Cases
Disturbingly, loss of smell and dysphagia, the inability to swallow, are both signs of Parkinson’s disease, and both of these conditions are being reported post-jab by the thousands. So, in years to come, we could be looking at an explosion of Parkinson’s.
“Parkinson’s studies have shown that you can get pathogens in the gut that produce a prion-like protein, which is what the spike protein is. The immune cells then take it up and take it to the spleen. This, of course, causes stress.
A stressed immune cell in the spleen upregulates and produces more alpha-synuclein. Alpha-synuclein is a molecule that fights infection, and that’s the molecule that misfolds in association with Parkinson’s disease.
I’m fascinated with all of these molecules that are prion-like. There’s the prion protein itself, which is associated with CJD, Creutzfeldt-Jakob disease, but then there’s the alpha-synuclein and amyloid beta, there’s TDP-43, which is associated with ALS.
All of those diseases are overrepresented in the VAERS database for the COVID shots, compared to all the other vaccines combined over 31 years. It’s just completely out of line.
There are 58 cases of Alzheimer’s in association with the COVID vaccines, and 13 in association with all the other vaccines over 31 years. That’s several times more — 58 versus 13.
CJD is also much more common. It’s almost seven times as common in the COVID vaccine cases. CJD is a terrible disease. You get very crippled and die after a few years. That’s the classic prion protein [disease]. It’s extremely rare. Only 1 in 1 million gets CJD.
There was a person who contacted me from France whose wife got CJD just a few weeks after the second vaccine. He was absolutely convinced the vaccine caused it. There are actually 27 cases [of CJD] reported in VAERS for the COVID-19 vaccines, against only four cases over the entire history of all other vaccines combined.”
Health Problems We Can Expect to See More Of
In time, Seneff predicts we’ll see a dramatic increase in infections and cancers of all types, autoimmune diseases, neurodegenerative diseases and reproductive issues. As mentioned, research has demonstrated that the spike protein accumulates in the spleen and women’s ovaries.
Without doubt, inflammation in the ovaries is not a good thing. Men also report swollen testes, and that could be indicative of inflammation as well. Preliminary data show women who get the jab within the first 20 weeks of pregnancy have a miscarriage rate of 82% to 91%.5 There are also VAERS reports describing fetal damage. Of course, it could also impair future fertility.
As described earlier, some antibodies produced by the jab can react to human proteins. One protein that is similar to the spike protein that the antibodies attack is syncytin, which is essential for the fertilization of the egg. The concern is that the antibodies might attack and destroy syncytin, thereby disrupting and preventing implantation in the placenta.
Omicron — A Blessing in Disguise?
The jabs also perpetuate COVID, with ever-new variants of the virus.
“In the first paper that Greg and I wrote, we predicted the vaccines would cause an increased emergence of variants of spike protein, altered versions of the virus, under the pressure of the vaccine,” Seneff says.
“Indeed, it looks to me like that’s what’s happening. But I’m really hopeful with Omicron, because Omicron looks like it’s a milder virus, but incredibly infectious. It’ll flash through the population and give everybody, essentially, a vaccine. It’s kind of like a natural vaccine, I think.
[Research] showed that … having had Omicron, you were protected, to some extent, from Delta. Delta’s disappearing anyway, because Omicron is chasing it out. It’s really great. I think Omicron is God’s gift from heaven.”
That blessing may be canceled out in those who have received multiple COVID jabs, however. Each dose erodes your immune response, such that it becomes increasingly compromised with each jab. Again, this has to do with the suppression of type-1 interferon, discussed earlier.
What Catalyzes Damage in Athletes?
More than 400 cases of serious heart problems and death have also been reported among professional athletes,6 who are some of the healthiest people on the planet. What mechanism can account for this phenomenon? How is it that the COVID jabs can cause enough damage to take out young people with optimized biology?
Seneff suspects that being fit might cause you to have more ACE2 receptors in the heart, and the S1 portion of the SARS-CoV-2 spike protein binds to the ACE2 receptor. She believes the spike protein is being delivered to the heart via exosomes, by way of the vagus nerve, and, again, the miR-155 exosome is associated with heart problems.7
Additionally, when the S1 spike protein binds to the ACE2 receptor,8 it disables the receptor. When you disable ACE2, you get an increase in ACE, which causes high blood pressure and elevates angiotensin 2. When angiotensin 2 is overexpressed, you can get intense inflammation in the heart. If you’re engaging in intense exertion and your heart is inflamed, you can trigger cardiac arrest, which is what we see in many of these athlete cases. They’re collapsing on the field.
G-Quadruplexes
Another focus of Seneff’s and McCullough’s paper is something called G4 or G-quadruplexes.
“G-quadruplexes are really fascinating, and I don’t have a handle on them at all,” Seneff says. “It’s hard biology, even harder than a lot of the other stuff that I’ve been reading …
G4s are basically an arrangement of [guanines]. Guanines are one of the four nucleotides that make up DNA or RNA. Guanine is the G in the G4. What happens is that a sequence of nucleotides on a DNA or an RNA string can fold in on itself and form G-quadruplexes. It’s four guanines, at different places on the protein, winding back around and sticking together.
There’s a metal in the middle — often potassium or calcium — that helps to stabilize these G4s. The interesting thing about them is that they make the water around them structured. They make gelled water [aka exclusion zone (EZ) water] …
Those G4s can form in the DNA, and that actually keeps it from becoming active. [The DNA] doesn’t get converted into RNA, and it doesn’t make protein if it has those G4s. Probably, the EZ water doesn’t allow anything to get close. Think of it as being stuck in a gel.
There are a lot of G4s in the promoter regions of these DNA sequences, and there are lots of proteins that have these G4s in their promoter region. Interestingly, there are certain proteins that can unravel them. There are proteins that can bind to them and cause the G4 to undo, and that activates or allows the protein to be expressed.
It’s a regulatory element that controls which proteins get to be expressed from the DNA. Many of the proteins that have these G4s in their promoter are cancer oncogenes. As long as they stay gelled, they’re inactive, but if they become ungelled, they become active.
It turns out that prion proteins … [are] made from RNA, and the RNA has these G4s. The protein can bind to the G4s in the RNA and both of them react. The theory is that the protein becomes prion-like. These prion proteins have two ways to be, one is safe and one is not safe, and the G4s increase the risk for prion protein misfolding.
The presence of those G4s, and the meeting with those G4s, increases the risk of misfolding in the prion-like configuration.9 The interesting thing about that is that spike protein is a prion-like protein. The RNA they built for the [COVID jab], they did something called codon optimization, which involved putting a lot more guanines into the RNA than [found] in the original [virus]. They enhanced the guanine.
Enhancing the guanine means increasing the number of G4s, which means increasing the risk of the spike protein misfolding into a prion like protein. I think that the G4s increase the risk, the danger of spike protein [acting] as a prion-like protein.
But we don’t really know what the consequence of having all these G4 RNAs in the cytoplasm will be. We have massive numbers of these RNAs sitting there with their G4s. What is that going to do to the rest of the G4 regulatory process? We do not know. Nobody knows. Nobody has a clue.”
Summary
To summarize the central point of Seneff’s latest paper, the COVID jab causes alpha interferon suppression, which weakens your immune system. Indeed, regulators in the European Union are now warning that repeat COVID shots can weaken overall immunity.10
The primary mechanism is the impairment of alpha interferon response, which is essential for the proper activation of your innate immune system, your cellular immunity, mostly your T-cells and killer cells. When functioning properly, the cell launches the type-1 interferon response as soon as it’s infected with a virus.
It triggers the immune cells to come in, kill the virus and remove the debris. This activates the humoral component of your immune system, the antibody production, which takes longer. (That’s why they say you are not protected until 14 days after the injection.)
How is type-1 interferon suppressed by the jab? It’s suppressed because type-1 interferon responds to viral RNA, and viral RNA is not present in the COVID shot. The RNA is modified to look like human RNA molecule, so the interferon pathway is not triggered. Worse, the interferon pathway is actively suppressed by the large number of spike proteins produced from the mRNA in the shot, and by the microRNAs in the exosomes released by the stressed immune cells.
(Natural News) Many decades ago a Canadian scientist figured out how to turn deadly rapeseed oil, a known insecticide, into a cheap, “FDA-approved” oil to be used as a preservative in foods. Now canola oil is a top export from Canada to the USA, and several “natural food” stores, including Trader Joes and Whole Foods, are putting it in thousands of products because most Americans, even many natural health advocates, have no idea the damage it does to the body and brain.
Some consumers think canola oil must be okay if it’s certified organic, or expeller-pressed, or simply sold at a “natural foods” store, but they would be dead wrong. Comprehensive studies done on canola oil, sourced in this article, reveal damage that’s done to the heart and brain, not to mention that rapeseed oil causes memory loss and mass weight gain. So where might this far-from-nutritious oil be found? One would need to write an entire book to list all the products, but let’s start here.
Whole Foods and Trader Joes put canola oil in thousands of their products — it’s cheap and hardly anyone knows it causes weight gain and memory loss
Head on out to a “Canola Joes” in your town and start flipping over nearly every processed and prepared product in the store, and read the ingredients carefully. Remember, the closer to the beginning of the ingredients list you find it, the more the product has in it, compared to other ingredients.
Start with prepared hummus, potato salad, salad dressings, soups, mayonnaise (even vegan), and most prepared foods that are mixed up in a creamy way. Even bugs won’t eat this stuff. This is done because it keeps the food from spoiling so fast, so Trader Joes can keep it all on the shelves much longer, making them more money while unknowing Americans suffer the health consequences, all while thinking they’re buying “healthier” food.
Don’t forget to also check for canola oil in chip bags, breads, cookies, cakes, nuts, seeds, most desserts and nearly all the frozen prepared meals that contain rice, vegetables, fried meats and more.
Canola study reveals direct link to heart lesions and a decrease in working memory
Here’s what happens when you consume canola oil regularly. Scientists have discovered a DIRECT LINK to a loss of working memory, heart lesions and cardiovascular problems. Rats that consume it also experience rapid weight gain. Maybe that’s why every third American is overweight, and half of those folks are considered obese. Canola is the opposite of “heart healthy” as the lying corporate labels imply. Plus, more than 90 percent of canola oil is genetically modified to contain even more pesticides.
How does canola oil mess up your brain? Researchers concluded canola oil increases plaque build-up that causes degenerative diseases like dementia and Alzheimer’s. Memory function for rats tested decreased while body weight increased significantly. Most restaurants in America use canola oil also, because it’s so cheap and they don’t have to reveal it on the menus.
If you’re ever driving and see huge fields of yellow flowers, especially in Europe, you are probably looking at rapeseed flowers. The toxic oil that comes from processing rapeseed is called erucic oil, and it’s still present in canola oil. It raises bad cholesterol in humans, both young and adult.
If you still feel you must micro-shop at Canola Joes or Canola Foods stores, be sure not to purchase any products that contain canola oil, or you might lose so much memory that you don’t even remember reading this article.
Tune your internet dial to FoodSupply.news for updates on contaminants purposely put in the American food supply, so you don’t eat them anymore.
Criminal complaint filed in Texas accuses COVID-19 vaccine makers and pushers of “murder” and “crimes against humanity”
(Natural News) A massive criminal complaint filed last week with Texas Attorney General Ken Paxton’s office accuses the makers of COVID-19 vaccines, as well as all corporate and government officials involved in pushing and distributing them, with “murder” and “crimes against humanity.”
The complaint, which was filed by Harris County resident Jack E. Boteler, represents “all interested parties and subscribed citizens and residents of the United States of America who received any Emergency Use Authorization investigational injection of genetic biologic material (mRNA or adenoviral DNA) coding for the Wuhan spike protein known to be the pathogenic structure of SARS-CoV-2 designed to provoke the human body to produce antibodies for Covid 19, commonly referred to as the ‘Covid 19 vaccines.’”
Some of those specifically named in the complaint include:
— Dr. Anthony Fauci, director of the National Institute of Allergy and Infectious Diseases and the Chief Medical Advisor to President Joe Biden;
— George Soros, billionaire financier and globalist counter-revolutionary
— Dr. Deborah Birx, White House Coronavirus Response Coordinator under President Donald Trump
— Director-General Tedros Adhanom Ghebreyesus of the World Health Organization
— Dr. Francis Collins, former director of the National Institutes of Health
— CNN founder and billionaire media mogul Ted Turner
— Billionaire Microsoft founder and noted vaccine pusher Bill Gates
— The directors and principals of the Food and Drug Administration, Dept. of Health and Human Services; the NIH, NIAID, and several other U.S. government agencies;
— Big Pharma
— Anyone else associated with manufacturing, marketing, and distributing COVID vaccines.
“This Complaint alleges murder and crimes against humanity arising from a collection of facts, observations, expert opinions, media reports and eye-witness testimony,” Boteler’s complaint continues.
“It will show that Defendants planned and executed, jointly and/or severely, the development and release of a bio warfare toxin, referred to herein as either “SARS-CoV-2” or “Covid 19” and/or as the ‘Spike Protein’ component with the dual objectives of: 1) global depopulation, and 2) population control leading to a one-world government by inducing panic, economic hardship, terror, death and injury to global populations,” it adds.
Boteler also explained:
By employing psychological warfare mechanisms, including but not limited to media reports, public policy, coercion, deceit, mandates, bribes, travel restrictions, employment restrictions, free speech restrictions and liberty restrictions, this complaint will also show that Defendants seek to induce the global population into receiving a pre-planned experimental gene therapy commonly referred to as “Covid 19 Vaccines” in furtherance of their aforementioned objectives.
The complaint then laid out cases against Fauci, Gates and others who are listed as defendants, citing reams of data, several reports and a timeline of events spanning decades and leading up to what the complaint alleges was the purposeful release of SARS-CoV-2 after it was manufactured in a Wuhan, China lab. It also cites Fauci for allegedly funding “gain of function research” that creates hyper-infectious viruses, ostensibly for the purpose of research.
It also quotes Fauci, who reportedly met with then-President-elect Donald Trump to warn: “There is no question that there will be a challenge to the coming administration in the arena of infectious diseases. … The thing we’re extraordinarily confident about is that we are going to see this in the next few years.”
The complaint concludes, “The overwhelming sum of information presented herein, much of it incontrovertible, offers more than sufficient probable cause to believe that one or more of the named Defendants has committed the offenses alleged in this Criminal Complaint, specifically mass murder through the commission of crimes against humanity.”
Defendants “planned, coordinated, colluded and collaborated among two or more named and unnamed Defendants to design a criminal enterprise” surrounding the creation of COVID-19, says the complaint, adding they also conspired to create a biological weapon which was eventually unleashed on the world.
(Natural News) As the narrative surrounding the Wuhan coronavirus (Covid-19) global psy-op (psychological operation) continues to break down, here are five things you need to know (as explained by Steve Kirsch):
1) Even the World Health Organization (WHO) is warning against covid “booster” shots
It made sense to some people to just go along with it when it was just one or two doses. But now that governments want people to take a third or even a fourth injection for the Fauci Flu, many are saying enough is enough.
Both EEU regulators and officials at WHO now admit that booster shots do not make sense, which is why they are advising the public against taking them. There is no evidence to support a booster shot program and everybody knows it.
2) More jabs means more infections
They have been trying to hide this fact from the public, but the data clearly shows that the more shots people get, the more likely they are to develop symptoms associated with “covid.”
The unvaccinated, meanwhile, are healthier, on average, compared to their “fully vaccinated” counterparts.
3) Covid jabs are NOT safe
On top of not working as claimed, covid injections are also unsafe. Many formerly pro-vaccine doctors and other health experts are speaking out against the shots, warning that they do not work.
“This is great news,” Kirsch writes. “Nobody is going public yet, but they are all [upset] and realize they have been misled. It will not be pretty. This is of course great news.”
4) Face masks do not protect against disease (hint: they spread MORE of it)
It took a long time to get to this point, but the U.S. Centers for Disease Control and Prevention (CDC) has finally admitted that cloth masks are useless at preventing the spread of covid or any other disease.
Corrupt CDC head Rochelle Walensky had no way out of fessing up to this truth after data was published showing that face veils are more of a religious rite than a viable medical intervention.
“The other mask types don’t work either, but it will take them longer to figure out the obvious,” Kirsh says.
“P100 respirators do work but only a small percentage of people know that. I can’t wait to see Rochelle Walensky wear a P100 respirator; after all, she should be modelling best practices.”
5) Young people especially should not be getting “boosted”
Even though Tony Fauci claims otherwise, there is zero evidence to suggest that covid injections are safe or effective for young people.
In fact, many doctors and other health experts are warning against parents getting their children “boosted,” despite the fact that leftist colleges and universities all across the country are demanding them of students who wish to return to campus.
“Someone is very wrong here and for once it isn’t the WHO,” Kirsh says.
A few other things Kirsch says people should know is that remdesivir is dangerous and ineffective. It has become standard procedure to administer this drug to covid patients at hospitals across America, but only because Fauci makes money every time remdesivir is injected into a patient’s body.
Also, social distancing is a farce. MIT came out with a study back in April which found that avoiding other people and treating them like the walking plague does nothing to stop the spread of disease.
“6 feet or 60 feet made no difference,” Kirsch writes. “People still haven’t figured this out.”
One of Kirsch’s subscribers pointed out that it was obvious from the beginning that all of this was nonsense. But better late than never, right?
The latest news about the Fauci Flu can be found at Pandemic.news.
Too many people submitted to the mandates to save their jobs.
For some, that has meant injury or death.
The numbers are still a mystery due to lack of transparency by our medical-industrial complex.
Steve Kirsch (Executive Director of the Vaccine Safety Research Foundation) has the data.
He used a government database and the CDC’s methodology for determining number of deaths, because VAERS is under-reported.
He discovered that 150K to 400K people are being killed — to save fewer than 10K lives.
Watch health care workers and other professionals blow the cover off the false narrative that normal people are spreading sickness. Normal people are being referred to as “the unvaccinated” while it’s the injected people who are getting sick and clogging the hospitals.
The FACTS and Data tell the TRUTH … those who are INFECTED and SICK in the Hospitals are the VACCINATED! The BIO-WEAPON is doing what it was designed to do … Genetically Modify People, Destroy their Immune System and Depopulate Humanity … causing CHAOS … which will lead to a the NWO RESET!
Source: Paul Joseph Watson
★AND WE KNOW PINS – 14k Gold Plated And We Know is based on Romans 8:28 “And we know that all things work together for good to them that love God, to them who are the called according to his purpose.” ★ Proudly Made in the USA https://thepatriotpin.com/AndWeKnow?tracking=AndWeKnow
★ 14k Gold Plated American Eagle Pin will show your support for America.
Proudly wear your American Eagle Pin on your hat or collar or anything
you want. https://www.andweknow.com/servicesmagazine
★ 14k Gold Plated GOP Elephant pin will show your support for the
Republican party. Order several for your Republican friends. https://www.andweknow.com/servicesmagazine
Beginning January 27, 2022, England will no longer require COVID vaccine passports for entry into certain public places and events. They also are ending mask mandates, including those for schoolchildren. Work-from-home requirements are also being dropped.
Prime Minister Boris Johnson announced the abrupt change in COVID-19 policies to cheers and applause from House of Commons members. He also is dropping testing rules for vaccinated UK-bound travelers.
Only Britain’s health care workers will still be under a vaccine mandate.
In a compilation of the propaganda-filled narratives that the NIH and other public health and government officials have been feeding the world during the pandemic, Awaken With JP points out 16 ways their narrative is now falling apart.
From a stunning revelation uncovered by Project Veritas to the real reason so many children are hospitalized to pointing out the CDC’s mistakes made through Dr. Rochelle Walensky, Awaken With JP tells it all.
“People are intelligent enough that you can’t fool them forever,” he says.
A British radio presenter, Lisa Shaw, died in May 2021, three weeks after taking her first dose of AstraZeneca’s COVID-19 vaccine.
She initially developed severe headaches, then went to the hospital for help, where she later died. Doctors confirmed Shaw died from the shot, saying, “it was clearly established Lisa’s death was caused by vaccine-induced thrombocytopenia, blood clots and swelling to the brain.”
SOURCE: Odysee January 4, 2022
A video interviewing an American doctor whose license to practice was suspended because of “misconduct” that included prescribing ivermectin and hydroxychloroquine to treat COVID-19 was removed by YouTube almost as soon as it was published.
Dr. Meryl Nass was interviewed by journalist Tessa Lena, who then posted it to YouTube. Lena said YouTube pulled removed the video after only five minutes so she had to repost it to Rumble, where freedom of speech is still free. Nass, who early in the pandemic concluded that the virus was lab-originated, made a post of her own, commenting that an online news magazine, American Thinker, had covered her case with “balance.”
For the record, Nass also broke the news that the hydroxychloroquine used in a study that “proved” it was lethal and didn’t work was actually administered at near-lethal doses — ensuring that the study would “prove” HCQ was “dangerous.”
Along with her suspension, Nass was also ordered to undergo a psychiatric evaluation.
Have you ever wondered what differentiates the COVID jabs from normal vaccines that you are more familiar with, such as measles, chickenpox and mumps? In an astutely written commentary, an anonymous nurse has compiled a provocative list comparing regular vaccines to the shots for COVID.
For example, she says: “I have never seen a vaccine that forced me to wear a mask and maintain my social distance, even when you are fully vaccinated … I have never seen a vaccine that threatens the relationship between family, colleagues and friends. I have never seen a vaccine used to threaten livelihoods, work or school.”
Her list is longer, but blogger and vaccine investigator Steve Kirsch has more of his own thoughts to add, including “It does all these things except IMMUNIZATION.” He adds, “If we still need a booster dose after we are fully vaccinated, and we still need to get a negative test after we are fully vaccinated, and we still need to wear a mask after we are fully vaccinated, and still be hospitalized after we have been fully vaccinated, it will likely come to “It’s time for us to admit that we’ve been completely deceived.”
He adds a few more, which are well worth reading, including thoughts on the lockdowns and deaths as a result of the shots.
In this short video we learn why freedom is a value, not an instinct, and why every new generation must be taught the supreme importance of freedom.
We also must learn how to distinguish totalitarianism from true empathy, as many oppressors will say what they’re doing to you is only done in the name of compassion — a type of faux compassion that actually means your freedoms are being compressed and eliminated one step at a time.
In essence, by acquiescing, you are allowing someone else to squelch you into submission and silence until your freedoms are gone.
Compelling research published in the January 2022 issue of Journal of Natural Products shows that certain compounds found in cannabis can block COVID-19’s entry into cells.
Specifically, as summarized by Forbes, “two cannabinoid acids commonly found in hemp varietals of cannabis, cannabigerolic acid, or CBGA, and cannabidiolic acid, also known as CBDA, can bind to the spike protein of SARS-CoV-2, the virus that causes Covid-19. By binding to the spike protein, the compounds can prevent the virus from entering cells and causing infection, potentially offering new avenues to prevent and treat the disease.”
Since these compounds are abundant in hemp and hemp extracts, they are not controlled substances like THC in marijuana, Forbes explains. Plus, “they have a good safety profile.”
Robert F. Kennedy Jr. succinctly summarizes how Dr. Anthony Fauci wields his power to control and manipulate science across the globe
It’s Fauci’s job to conduct research on chronic diseases to figure out their etiology and environmental causes to protect public health, but instead he turned the NIAID into an incubator for pharmaceuticals
Fauci has a $7.6 billion annual budget that he uses to develop new drugs, which he then farms out to universities
Fauci’s control — in collusion with that of Bill Gates — has rendered the majority of global scientific research nothing more than pharmaceutical propaganda
Fauci shares drug patents with universities, sells them to drug companies, splits the patents with them, and walks those drugs through the FDA approval process, which he also controls; once approved, Fauci himself often profits
Robert F. Kennedy Jr. succinctly summarizes how Dr. Anthony Fauci wields his power to control and manipulate science in this riveting episode of The Jimmy Dore Show.1 Fauci has been painted as a hero throughout the pandemic, an image that is not only misleading but wildly inaccurate, as detailed in Kennedy’s best-selling book, “The Real Anthony Fauci.”
“I wrote the book because so many Americans were looking at Tony Fauci as this kind of savior,” Kennedy said. “… [T]he man on the white horse, or in the white lab coat, that would ride us out of this coronavirus crises but I knew from the beginning … that he does not do public health and has not done public health since the 1980s.”2,3
Rather than looking out for public health, Fauci and his agency, the National Institute of Allergy and Infectious Diseases (NIAID), prioritize pharmaceutical promotion. Kennedy refers to Fauci as the “leader of the pack” when it comes to those promoting pharmaceutical products, profiteering from Big Pharma and promoting their own personal power.
Public Health Plummeted During Fauci’s Reign
In 1984, when Fauci was appointed director of NIAID, 11.8% of Americans had chronic disease, but this has risen sharply since.4 Fauci doesn’t talk about this public health failure — at least not publicly — but as Kennedy noted, it was Fauci’s job to figure out why cases of autism, food allergies, ADHD, sleep disorders, juvenile diabetes, rheumatoid arthritis and many other chronic and infectious diseases have skyrocketed.
It was Fauci’s job to conduct research on these diseases to figure out their etiology and environmental causes to protect public health, but instead he turned the NIAID into an incubator for pharmaceuticals. According to Kennedy:5
“When Tony Fauci came in, 6% of American children had chronic disease. By 2006, 54% had it. We went from being the healthiest country in the world with the healthiest children to the sickest. Literally, we do not even qualify as a developed nation. We are 79th in the world, behind Nicaragua and Costa Rica in terms of our health outcomes.
And why did that happen? Well, the one figure who is more responsible for that than anybody else in the world is Tony Fauci. He is the reason we take more pharmaceutical drugs than any other nation in the world. Three times the average among western countries. We pay the highest prices and have the worst outcomes.”
Fauci’s Multibillion-Dollar Budget Gives Him Immense Power
Fauci has a $7.6 billion annual budget, which in total during his entire tenure is more than half a trillion dollars that he’s been in control of. Instead of using that to reveal the environmental issues leading to outbreaks of chronic disease, he uses the money to develop new drugs, Kennedy explains, which he then farms out to universities:6
“He shares the patents with them, and then he sells them to the drug companies, splits the patents with them, and he walks those drugs through the FDA approval process, which he completely controls from the bottom up. And then he gets them approved and in many cases he himself profits. People within his agency can collect $150,000 a year from royalties off each of these products.”
The NIH owns half the patent for Moderna’s COVID-19 injection, which means that it stands to make billions of dollars as a result. Four of Fauci’s top deputies will also collect $150,000 a year for life as a result — from a product they’re responsible for regulating, an obvious massive conflict of interests.
“The mercantile and commercial interests have overwhelmed the regulatory function at that agency and it no longer does public health — it does pharmaceutical promotion,” Kennedy said.7 As an example, between 2009 and 2016 there were 240 new drugs approved by the FDA, all of which came out of Fauci’s “shop,” he added. “He is the incubator for the whole pharmaceutical industry.”8
How Fauci Controls Science Globally
Fauci has spread the notion that he is untouchable, going so far as to tell MSNBC that an attack on him is an attack on science:9
“It’s very dangerous … because a lot of what you’re seeing as attacks on me quite frankly are attacks on science, because all of the things that I have spoken about consistently from the very beginning, have been fundamentally based on science.”
Throughout the pandemic, “trusting the science” has become a cultural statement and propaganda tool, but one that’s far from what true science is all about. Far from being a source of independent science, in essence Fauci’s control — in collusion with that of Bill Gates — has rendered the majority of global scientific research nothing more than pharmaceutical propaganda. Kennedy explains:10
“Every virologist in the world knew that the coronavirus was engineered. All you have to do is look at the genome. Everybody knew that and they kept silent for a year, and here’s how. He gives away $7.6 billion a year. That’s two to three times what [Bill] Gates gives away. Him and Gates work tandemly. They partner up on everything. They talk together a couple times a week.
They are business partners … in 2000, in Gates’ library, the two of them got together and they formally formed a partnership. You take those two and one other guy — Jeremey Farrar — who is their other de facto partner who is the head of the Wellcome Trust, which is the U.K. version of the Bill and Melinda Gates Foundation. Between those three men, they control 61% of the biomedical research funding on Earth.
So if you want to get your study funded, you’ve got to go to those guys. Not only can they give you the money, but they also can kill a study because they control all of the other funding sources. They can kill a study, they can ruin a career, they can bankrupt colleges who do science that they don’t want done. So they are able to really dictate virtually all the science on the globe.”
Drug Companies and Universities All Benefit
Kennedy gives a theoretical example of how Fauci yields his immense power to influence science: In his lab, Fauci develops a molecule that kills a virus. This is done by scientists dropping molecules onto one of countless viruses — influenza, Ebola, coronaviruses, zika and others — in petri dishes and test tubes to see if it kills them. If the molecule works to kill the virus in a petri dish, they move on to testing it on rats infected with the virus.
“If the rats don’t die, now he’s got a drug,” he says. “It’s an antiviral and it’s usable in mammals because it will kill the virus but it won’t kill the mammal. Then he farms it out to the university.”11There, a PI, or principal investigator, who is usually a person of power, such as the dean of a department, does a phase I trial, experimenting on animals and around 100 humans. Kennedy explains:12
“For each of the humans that he recruits — he’s a medical doctor, he brings in patients, persuades them to take part in the study — Tony Fauci’s agency gives him $15,000 for every one of those patients. The university keeps 50% of that so now they’re also part of this process. And then if the drug gets through that phase I, then they move on to phase 2 and phase 3. So now they have to bring in 20,000 or 30,000 people.
They bring in a drug company as a partner, and they go through the phase 2 and phase 3 [trials], and then at the end of it, they all split up the patents. So the drug company owns half, Tony Fauci’s agency may get part of it and he and his cronies take little slivers of it so they get paid for life. The university gets a part of it, so now you have all the medical schools in the country … dependent on this income stream.”
‘Independent Panels’ Aren’t Independent
At this point, the new drug still has to get regulatory approval, which brings it before a supposedly independent panel of experts. But this panel isn’t made up of independent scientists looking for the truth about whether or not the drug is safe and effective; it’s made up of Fauci’s and Gates’ PIs, who often have drugs of their own in development. Kennedy continues:13
“When this drug goes to FDA to get approved, it goes to a panel. Tony Fauci’s always saying it’s an independent panel who decides, based upon real science, whether or not this drug is worthy of approval. It’s not an independent science. They’re virtually all his PIs or Gates’ PIs.
Those guys go sit on that panel for a year, and they know that they’ve got their own drugs back at Baylor University they’re working on, or Berkeley or Columbia, that they know are going to be in front of that same panel next year. And they’re all scratching each other’s backs. And they approve that drug and then they go off the panel, finish their drug, and then that drug goes in front of a panel that’s similarly constituted and populated.”
These principal scientists act as gatekeepers to the public, spreading the official narrative under the guise of independent science, often pushing questionable COVID-19 policies. “These PIs control the journals, they control the public debate, they’re on TV all over the world, and these are the people that form the narrative, that protect the orthodoxy,” Kennedy says.14
“If you look at Tony Fauci as the pope, the PIs are the cardinals, the bishops and the archbishops. And they’re the ones that protect the orthodoxy, that make sure that the heretics burn, that doctors who disagree are … delicensed, that they get discredited, that they get gaslighted and vilified and marginalized. They’re the army that controls the narrative.”15
Waking up to Fauci’s façade is necessary to understand the orchestrated planned use of pandemics to clamp down totalitarian control. You can find even more details about the coalition of sinister forces — intelligence agencies, pharmaceutical companies, social media titans, medical bureaucracies, mainstream media and the military — that are intent on obliterating constitutional rights globally in “The Real Anthony Fauci.”
Kennedy’s book has been a best seller for two months now and if you haven’t already picked up a copy I would encourage you to do so now.
Eric Trump, Lance Walnau, Dr. David Martin, Comedian Jim Breuer, Dr. Vladimir Zelenko, Del Bigtree, Dr. Peter McCullough, Sean Feucht, Karen Kingston, Debbie G. Are Joining the ReAwaken America Tour!!!
The Historical Price of Gold:
Price Per Ounce – 1971 – $44.60
Price Per Ounce – 1999 – $278.86
Price Per Ounce – 2006 – $604.34
Price Per Ounce – 2021 – $1,895.50
The Biggest Weapon Threats Facing America:
Chemical
Biological
Radiological
Nuclear
General Flynn’s ReAwaken America Tour Gains Momentum!!!
Eric Trump, Kim Clement’s Daughter (Donné Clement Petruska), Dr. Zelenko, Sean Feucht, Dr. Jane Ruby, Charlie Kirk, Roger Stone, Dr. Judy Mikovits, Dr. Peter McCullough, Dr. Stella Immanuel, Dr. Sherri Tenpenny, Lance Walnau, Hi-Rez & Jimmy Levy, Comedian Jim Breuer, & Dr. Martin Join the Tour…
Request Tickets Today At: https://www.thrivetimeshow.com/reawaken-america-tour/
*Phoenix, AZ – January 14th & 15th – 12 Tickets Remain
*Canton, OH – February 18th & 19th – Tickets On Sale
*San Diego, CA – March 11th & 12th – Tickets On Sale
*Redmond, OR – April 1st & 2nd – Tickets On Sale
ReAwaken America Tour History:
*April – Tulsa, Oklahoma was 100% Sold Out
*June – Tampa, Florida Was 100% Sold Out
*July – Anaheim, California Was 100% Sold Out
*August – Grand Rapids, Michigan Was 100% Sold Out
*September – Colorado Springs, CO Was 100% Sold Out
*November – San Antonio, TX Was 100% Sold Out
*December – Dallas, TX Was 100% Sold Out
ReAwaken America Tour Featured / Past Speakers Include:
General Flynn, Mike Lindell, Robert F. Kennedy, Texas Attorney General of Texas Ken Paxton, Charlie Kirk, Chad Prather, Pastor Phil Hotsenpiller, Robert Kennedy Jr., Ian Smith, Roger Stone, Alex Jones, Owen Schroyer, Melissa Tate, Trump-Attorney Jenna Ellis, Dave Scarlett, Senator Wendy Rogers, Doctor Richard Bartlett, Gene Ho, Patrick Byrne, Scott McCay, Anna Khait, Sam Sorbo, Doctor Mark Sherwood, Attorney Thomas Renz, Doctor Stella Emmanuel, Attorney Leigh Dundas, Doctor Jim Meehan, Sheriff Vic Regalado, Joey Gilbert, Doctor Sherri Tenpenny, Doctor Rob Marsh, Leila Centner, Lori Gregory, Kevin Jenkins, Doctor Carrie Madej, Doctor Judy Mikovits, Steve Maxwell, Doctor Eric Nepute, Alfie Oakes, Sidney Powell, Doctor Alan Keyes, Pastor Artur Pawlowski, Mike Provenzano, Doctor Shannon Kroner, Doctor Andy Wakefeld, Pastor Jackson Lahmeyer, Amanda Grace, Doctor Cordie Williams, Pastor Mark Burns,etc.
Find Jobs That Don’t Require the COVID-19 Vaccines- https://timetofreeamerica.com/no-jab-jobs/
Request Your COVID-19 Vaccine Religious Exemptions: http://www.NewLifeHarvestChurch.org & http://www.JacksonLahmeyer.com
Want to Join the ReAwaken America Tour? Request Tickets At: https://timetofreeamerica.com/
Episode 1 of the ReAwaken Tour Documentary Has Been Released – WATCH NOW – https://reawakeningseries.com/
Join the Airline Injunction Action Against the COVID-19 Vaccine Mandate: https://timetofreeamerica.com/airline-injunction/#scroll-content
Find Affordable & Effective COVID-19 Treatments: https://tapme.ws/rnJfL4
Buy ReAwaken America Shirts, Hoodies and Books Today At: https://tapme.ws/COuEDM
Get the 100% Affordable & Effective COVID-19 Treatments At: https://timetofreeamerica.com/proven-treatments/#scroll-content http://www.VladimirZelenkoMD.com/ – 7,000 COVID-19 Patients (3 Deaths) http://www.Sherwood.TV – 9,000 COVID-19 Patients (0 Deaths) http://www.MeehanMD.com – 3,200 COVID-19 Patients (0 Deaths) http://www.MyGoToDoc.com – 4,500 + COVID-19 Patients (0 Deaths) http://www.OneCrossHealth.com – 1,500 COVID-19 Patients (0 Deaths) http://www.NeputeWellness.com – 10,000 COVID-19 Patients (0 Deaths) http://www.SynergyHealthDPC.com/ http://www.DrStellaMD.com http://www.AmericasFrontLineDoctors.org http://www.BudesonideWorks.com – Doctor Richard Bartlett http://www.MyFreeDoctor.com
*********************************************************************************
Learn How to Wake Up Your Friends and Family While Showing Your Support: https://store.thrivetimeshow.com/
Support Mike Lindell and America’s Quest for Election Integrity At: https://www.mypillow.com/clay
The Fourth Industrial Revolution and genetically modified humans – https://rumble.com/vld6yh-the-fourth-industrial-revolution-and-genetically-modified-humans.html
Question #1 – Does the Mark of the Beast Technology Now Exist?
Why Did Microsoft File for a Patent for a Cryptocurrency System Using Body Activity with a Publication Number WO-2020-060606? https://patentscope.wipo.int/search/en/detail.jsf?docId=WO2020060606
Revelation Chapter 13: 16-18 (Revelation was written by John the Apostle While Being Exiled On the Island of Patmos)
16 And he causeth all, both small and great, rich and poor, free and bond, to receive a mark in their right hand, or in their foreheads:
17 And that no man might buy or sell, save he that had the mark, or the name of the beast, or the number of his name.
18 Here is wisdom. Let him that hath understanding count the number of the beast: for it is the number of a man; and his number is Six hundred threescore and six.”
Methods and systems of prioritizing treatments, vaccination, testing and/or activities while protecting the privacy of individuals – Methods and Systems Patent #11-107588 – https://trea.com/information/methods-and-systems-of-prioritizing-treatments-vaccination-testing-andor-activit/patentgrant/e2dfec3c-d33d-44ac-bdb9-a5cfd91f1193
Why Are There Advanced Nano-Technologies Found Inside the COVID-19 Vaccines? Their Patents Prove Their Nefarious Plan
Patent # 10-703-789-B2 – https://www.modernatx.com/sites/default/files/US10703789.pdf
Patent # 2010 0216804 – https://patentimages.storage.googleapis.com/25/ce/6d/84cb16adb713b2/US20100216804A1.pdf
Patent # 20201859
Patent # 2012 0265001 ?
Down a Vaccination Exemption Form Today At: http://www.Team1986.com
Models are false – https://timetofreeamerica.com/the-models/#scroll-content
PCR tests are false – https://timetofreeamerica.com/case-inflation/#scroll-content
COVID is 100% treatable https://timetofreeamerica.com/case-inflation/#scroll-content
Kary Banks Mullis was an American biochemist. In recognition of his invention of the polymerase chain reaction technique, he shared the 1993 Nobel Prize in Chemistry with Michael Smith and was awarded the Japan Prize in the same year.
There is no SAVIOR without the luciferase vaccines: https://pubmed.ncbi.nlm.nih.gov/24715289/
Bill Gates Spirit Advisor – https://duckduckgo.com/?q=marina+abramovic+spirit+cooking&t=hd&va=u&iax=images&ia=images
Jeffrey Epstein / Bill Gates Worked to Create Their Own Race – https://www.nytimes.com/2019/07/31/business/jeffrey-epstein-eugenics.html
WO2020060606 – CRYPTOCURRENCY SYSTEM USING BODY ACTIVITY DATA https://patentscope.wipo.int/search/en/detail.jsf?docId=WO2020060606
What Is In the COVID-19 Vaccines? https://timetofreeamerica.com/vaccines-gates/#scroll-content
Question #2 – Why Is Congress Working On Legislation Called H.R.666? – Anti-Racism in Public Health Act of 2021 Proposed Legislation? – https://www.congress.gov/bill/117th-congress/house-bill/666
Question #3 – Why Is Congress Working on Legislation Called H.R.6666? – COVID-19 Testing, Reaching, And Contacting Everyone (TRACE) Act? https://www.congress.gov/bill/116th-congress/house-bill/6666/text
Question #4 – Why Is the Centers for Disease Control Calling for the Implementation of Nazi-Style Concentration Camps That They Are Calling Green Zones? https://www.cdc.gov/coronavirus/2019-ncov/global-covid-19/shielding-approach-humanitarian.html
Why Did the Governor of Tennessee Sign an Executive Order Authorizing the State to Remove People from Their Homes? https://publications.tnsosfiles.com/pub/execorders/exec-orders-lee83.pdf – Read Paragraphs 8, 14 and 18
Why Is GovernmentJobs.com Hiring Isolation & Quarantine Team Consultants, Isolation, and Vaccine Strike Team Staff?
Lewis County – Centralia, WA Isolation & Quarantine Team Consultants (PS2) – Non-Permanent – DOH5814 https://www.governmentjobs.com/jobs/3233390-0/isolation-quarantine-team-consultants-ps2-non-permanent-doh5814
Thurston County, WA Isolation & Quarantine Facility Staffing – COVID-19 Response https://www.governmentjobs.com/jobs/2918801-0 via @GovernmentJobs
Columbus, GA COVID-19 Vaccine Strike Team Staff https://www.governmentjobs.com/jobs/3220847-0 via @GovernmentJobs
Why Does the Centers for Disease Control Have a Section on Their Website Dedicated to Describing Quarantine Stations and Their Jurisdictions? https://www.cdc.gov/quarantine/quarantine-stations-us.html
Bill Gates- and George Soros-Backed Organization Buys Out COVID-19 Testing Company – https://www.theepochtimes.com/mkt_breakingnews/bill-gates-and-george-soros-buy-out-covid-19-testing-company_3909833.html?utm_source=News&utm_medium=email&utm_campaign=breaking-2021-07-20-2&mktids=4c7b77485753b708172bad88c5db2e09&est=Pntf4x%2FYSo3qmf8tbswC35G5Or9yEvDiGG0nyIkn%2B6jUssSBm7uf7Yc4ZKjFAJWiNsX2
Question #5 – Why Are International Celebrities and Powerful People Like Bill Gates Celebrating and Seeking the Satanic Guidance of the Spirit Cooking Marina Abramović Spirit Cooking? https://duckduckgo.com/?q=marina+abramovic+spirit+cooking&t=hc&va=o&iax=images&iar=images&ia=images
Microsoft Commercial – https://www.youtube.com/watch?v=0XmTRpfTvKI
Question #6 – Why Are Satanists Suing for Their Religious Right to Ritual Abortions? https://www.washingtontimes.com/news/2021/mar/6/satanists-sue-for-religious-right-to-ritual-aborti/
Question #7 – Why is Senomyx A Food Additive In the American Food Supply?
Senomyx develops patented flavor enhancers by using “proprietary taste receptor-based assay systems.” These receptors are made from HEK293. HEK stands for Human Embryonic Kidney cells.
Which Companies Are Using Aborted Human Fetuses in Their Food? https://dta0yqvfnusiq.cloudfront.net/allnaturalhealingsrq/2019/05/Companies-That-use-Aborted-Human-Fetuses-in-their-Foods-5ce5f2e5eb52e.pdf
Company Uses Cells From Abortions to Test Artificial Flavors – https://www.lifenews.com/2011/03/29/company-uses-fetal-cells-from-abortions-for-artificial-flavors/ https://www.lifesitenews.com/blogs/confused-about-the-pepsi-fetal-cell-issue-here-are-the-facts/ http://www.stopthecrime.net/senomyx.pdf
Which Companies Are Using Aborted Human Fetuses in Their Food? https://dta0yqvfnusiq.cloudfront.net/allnaturalhealingsrq/2019/05/Companies-That-use-Aborted-Human-Fetuses-in-their-Foods-5ce5f2e5eb52e.pdf
Question #8 – Why Was Jeffrey Epstein Working to Seed the Human Race With His DNA? https://www.nytimes.com/2019/07/31/business/jeffrey-epstein-eugenics.html
What’s Included In the COVID-19 Shots?
Dr. Jane Ruby
Why is graphene oxide, PEG (Polyethylene Glycol), M-RNA modifying nano-technology, SM-102, luciferase, fetal-tissue cell lines and inside the COVID-19 vaccines? Watch – https://rumble.com/vl9hlz-dr-jane-ruby-are-the-covid-19-vaccine-mandates-a-campaign-of-murder.html
VAXXED Patients’ Blood Examined, Horrific Findings Revealed by German Physicians! – https://rumble.com/vldaex-vaxxed-patients-blood-examined-horrific-findings-revealed-by-german-physici.html
Question #9 – Why Are Bill Gates, Elon Musk, and Others Obsessed with Transhumanism (Mixing Clay with Iron)?
Could Elon Musk’s Neuralink brain chips make us all as smart as he is? https://nypost.com/2021/03/06/rockets-brain-chips-is-elon-musk-superhero-or-supervillain/
“Please consider working at Neuralink! Short-term: solve brain/spine injuries Long-term: human/AI symbiosis. Latter will be species-level important. Work at either at our Bay Area or Austin locations.” – https://twitter.com/elonmusk/status/1356027336387252235?lang=en
Daniel Chapter 2: 40 – 43: “40 And the fourth kingdom shall be strong as iron: forasmuch as iron breaketh in pieces and subdueth all things: and as iron that breaketh all these, shall it break in pieces and bruise.
41 And whereas thou sawest the feet and toes, part of potters’ clay, and part of iron, the kingdom shall be divided; but there shall be in it of the strength of the iron, forasmuch as thou sawest the iron mixed with miry clay.
42 And as the toes of the feet were part of iron, and part of clay, so the kingdom shall be partly strong, and partly broken.
43 And whereas thou sawest iron mixed with miry clay, they shall mingle themselves with the seed of men: but they shall not cleave one to another, even as iron is not mixed with clay.”
Question #10 – Why The Satanic Temple of Texas files suit to defend its religious right to child sacrifice…tell us more about this? https://www.washingtontimes.com/news/2021/mar/6/satanists-sue-for-religious-right-to-ritual-aborti/
Why does the Pope’s Audience Hall look like a Snake Head? https://duckduckgo.com/?q=pope+snake+building&t=h_&iax=images&ia=images&iar=images https://duckduckgo.com/?q=pope+audience+hall+stage&t=h_&iar=images&iax=images&ia=images&iai=https%3A%2F%2Fi.pinimg.com%2F736x%2F9f%2Ff0%2F7c%2F9ff07ccc8521044593f7971a13bef0e6–paul-vi-pope-john-paul-ii.jpg
Question #11 – Why Did Jeffrey Epstein Have a Satanic Temple on His Island? https://duckduckgo.com/?q=jeffrey+epstein+island+temple&t=hc&va=o&iar=images&iax=images&ia=images
Question #12 – Why Did the Billionaire Bill Gates Who Is Developing the Vaccines Choose to Invest His Time with the World’s Most Prolific Pedophile Jeffrey Epstein? https://www.nytimes.com/2019/10/12/business/jeffrey-epstein-bill-gates.html
Question #13 – Why Are Luciferians Obsessed with Wearing Masks and Standing 6 Feet Apart from Each Other During Their Satanic Rituals? https://duckduckgo.com/?q=bohemian+grove&t=hc&va=o&iax=images&ia=images&iai=https%3A%2F%2Fsecureservercdn.net%2F198.71.233.44%2F8m7.439.myftpupload.com%2Fwp-content%2Fuploads%2Fimage31Optimized.jpg%3Ftime%3D1574392049
Question #14 – Why Would the Executive Chairman of the World Economic Forum Klaus Schwab Write a Book Titled COVID-19 – The Great Reset, Which Advocates for the Complete Destruction of Our God-Given Freedoms, the American Way of Life and the Implementation of a One World Government? Imphttps://http://www.amazon.com/COVID-19-Great-Reset-Klaus-Schwab/dp/2940631123/ref=sr_1_2?dchild=1&keywords=the+great+reset&qid=1615556362&sr=8-2
Question #15 – Why Is Moderna Now Referring to Their Vaccines Technology As the “Software of Life”? Technology – https://www.modernatx.com/mrna-technology/mrna-platform-enabling-drug-discovery-development
Question #16 – Why is Luciferase Technology Being Developed? https://www.moleculardevices.com/sites/default/files/en/assets/newsletter/november-2020.html#gref An enzyme that catalyzes the oxidation of a luciferin, causing it to produce a visible glow.
Question #17 – What Is the Statistical Probability of This?
“2 And the beast which I saw was like unto a leopard, and his feet were as the feet of a bear, and his mouth as the mouth of a lion: and the dragon gave him his power, and his seat, and great authority.” Revelation 13:2
Question #18 – Why is graphene oxide, PEG (Polyethylene Glycol), M-RNA modifying nano-technology, SM-102, luciferase, fetal-tissue cell lines and inside the COVID-19 vaccines?
Graphene Oxide – Graphene oxide (GO) is a unique material that can be viewed as a single monomolecular layer of graphite with various oxygen-containing functionalities such as epoxide, carbonyl, carboxyl, and hydroxyl groups.
Learn What Is In the COVID-19 Shots: https://timetofreeamerica.com/vaccines-gates/#scroll-content
Question #19 – Are We Living Through Matthew Chapter 24?
And Jesus went out, and departed from the temple: and his disciples came to him for to shew him the buildings of the temple.
And Jesus said unto them, See ye not all these things? verily I say unto you, There shall not be left here one stone upon another, that shall not be thrown down.
And as he sat upon the mount of Olives, the disciples came unto him privately, saying, Tell us, when shall these things be? and what shall be the sign of thy coming, and of the end of the world?
And Jesus answered and said unto them, Take heed that no man deceive you.
For many shall come in my name, saying, I am Christ; and shall deceive many.
And ye shall hear of wars and rumors of wars: see that ye be not troubled: for all these things must come to pass, but the end is not yet.
For nation shall rise against nation, and kingdom against kingdom: and there shall be famines, and pestilences, and earthquakes, in divers places.
All these are the beginning of sorrows.
Then shall they deliver you up to be afflicted, and shall kill you: and ye shall be hated of all nations for my name’s sake.
And then shall many be offended, and shall betray one another, and shall hate one another.
And many false prophets shall rise, and shall deceive many.
Examples:
Mainstream Media
Doctor Fauci
Bill Gates
And because iniquity shall abound, the love of many shall wax cold.
But he that shall endure unto the end, the same shall be saved.
And this gospel of the kingdom shall be preached in all the world for a witness unto all nations; and then shall the end come.
Elon Musk’s Starlink to Deliver Internet Nearly Worldwide Within Weeks https://www.bloomberg.com/news/articles/2021-06-29/musk-s-starlink-to-bring-internet-nearly-worldwide-within-weeks
Question #20 – If God Has Not Given Us a Spirit of Fear, Who Has Been Giving Us the Spirit of Fear? 2 Timothy 1:7
Where did the fear start?
FACT – The models created by the Abdul Latif Jameel Institute and Neil Ferguson that said that 2.2 million people would die were nefariously false.
NOTABLE QUOTABLE – “7 For God hath not given us the spirit of fear; but of power, and of love, and of a sound mind.” – 2 Timothy 1:7
NOTE: Fear blocks logic by causing your amygdala to become overactive
Question #21 – Why Would the Majority of Pastors Refuse to Teach from the Book of Revelation Chapter 13?
Revelation 13:2 – 2 And the beast which I saw was like unto a leopard, and his feet were as the feet of a bear, and his mouth as the mouth of a lion: and the dragon gave him his power, and his seat, and great authority.
Revelation 13: 9-18 – If any man have an ear, let him hear
10 He that leadeth into captivity shall go into captivity: he that killeth with the sword must be killed with the sword. Here is the patience and the faith of the saints.
11 And I beheld another beast coming up out of the earth; and he had two horns like a lamb, and he spake as a dragon.
12 And he exerciseth all the power of the first beast before him, and causeth the earth and them which dwell therein to worship the first beast, whose deadly wound was healed.
13 And he doeth great wonders, so that he maketh fire come down from heaven on the earth in the sight of men,
14 And deceiveth them that dwell on the earth by the means of those miracles which he had power to do in the sight of the beast; saying to them that dwell on the earth, that they should make an image to the beast, which had the wound by a sword, and did live.
15 And he had power to give life unto the image of the beast, that the image of the beast should both speak, and cause that as many as would not worship the image of the beast should be killed.
16 And he causeth all, both small and great, rich and poor, free and bond, to receive a mark in their right hand, or in their foreheads:
17 And that no man might buy or sell, save he that had the mark, or the name of the beast, or the number of his name.
18 Here is wisdom. Let him that hath understanding count the number of the beast: for it is the number of a man; and his number is Six hundred threescore and six.
NOTE: The book of Revelation which warned Christians about “The Mark of the Beast” was written on the island of Patmos by John.
Could It Be That We Are Wrestling Not Against Flesh and Blood, But Against Principalities, Powers, Rulers of the Darkness of this World and Against Spiritual Wickedness in High Places?
Question #22 – Why Is It Only Christians By and Large Who Know the Truth About What Is Really Going On?
FACT – The 100% effective COVID-19 treatments and therapies are being withheld from you for nefarious purposes.
NOTABLE QUOTABLE – “31 Then said Jesus to those Jews which believed on him, If ye continue in my word, then are ye my disciples indeed; 32 And ye shall know the truth, and the truth shall make you free.” – John 8:30-36
Question #23 – COVID-19 = Certificate Of Vaccination ID – 19 (AI)
Why Did MIT Develop Specialized Dye, Delivered Along with a Vaccine That Could Enable “on-patient” Storage of Vaccination History? https://news.mit.edu/2019/storing-vaccine-history-skin-1218
Question #24 – Why Did the Military Just Now Develop a New Weapon Called LOCUST?
“15 And the four angels were loosed, which were prepared for an hour, and a day, and a month, and a year, for to slay the third part of men.” – Revelation 9:15
“9 And the fifth angel sounded, and I saw a star fall from heaven unto the earth: and to him was given the key of the bottomless pit. 2 And he opened the bottomless pit; and there arose a smoke out of the pit, as the smoke of a great furnace; and the sun and the air were darkened by reason of the smoke of the pit. 3 And there came out of the smoke locusts upon the earth: and unto them was given power, as the scorpions of the earth have power.” – Revelation 9: 1-3 https://www.youtube.com/watch?v=qW77hVqux10
“And the light of a candle shall shine no more at all in thee; and the voice of the bridegroom and of the bride shall be heard no more at all in thee: for thy merchants were the great men of the earth; for by thy sorceries were all nations deceived.” – Revelation 18:23
Question #25 – Are the Elements Ready to Create the Third Temple?
“25 “Know and understand this: From the time the word goes out to restore and rebuild Jerusalem until the Anointed One,[a] the ruler, comes, there will be seven ‘sevens,’ and sixty-two ‘sevens.’ It will be rebuilt with streets and a trench, but in times of trouble. 26 After the sixty-two ‘sevens,’ the Anointed One will be put to death and will have nothing.[b] The people of the ruler who will come will destroy the city and the sanctuary. The end will come like a flood: War will continue until the end, and desolations have been decreed. 27 He will confirm a covenant with many for one ‘seven.’[c] In the middle of the ‘seven’[d] he will put an end to sacrifice and offering. And at the temple[e] he will set up an abomination that causes desolation, until the end that is decreed is poured out on him.” – Daniel 9:25-27
Daniel 9:25-27
Admit You Are a Sinner
Believe Christ Is Lord and Died for Our Sins
Confess Your Sins
Revelation 11 – “And there was given me a reed like unto a rod: and the angel stood, saying, Rise, and measure the temple of God, and the altar, and them that worship therein.
2 But the court which is without the temple leave out, and measure it not; for it is given unto the Gentiles: and the holy city shall they tread under foot forty and two months.
3 And I will give power unto my two witnesses, and they shall prophesy a thousand two hundred and threescore days, clothed in sackcloth.
4 These are the two olive trees, and the two candlesticks standing before the God of the earth.
5 And if any man will hurt them, fire proceedeth out of their mouth, and devoureth their enemies: and if any man will hurt them, he must in this manner be killed.
6 These have power to shut heaven, that it rain not in the days of their prophecy: and have power over waters to turn them to blood, and to smite the earth with all plagues, as often as they will.
7 And when they shall have finished their testimony, the beast that ascendeth out of the bottomless pit shall make war against them, and shall overcome them, and kill them.
8 And their dead bodies shall lie in the street of the great city, which spiritually is called Sodom and Egypt, where also our Lord was crucified.
9 And they of the people and kindreds and tongues and nations shall see their dead bodies three days and an half, and shall not suffer their dead bodies to be put in graves.
10 And they that dwell upon the earth shall rejoice over them, and make merry, and shall send gifts one to another; because these two prophets tormented them that dwelt on the earth.
11 And after three days and an half the spirit of life from God entered into them, and they stood upon their feet; and great fear fell upon them which saw them.
12 And they heard a great voice from heaven saying unto them, Come up hither. And they ascended up to heaven in a cloud; and their enemies beheld them.
13 And the same hour was there a great earthquake, and the tenth part of the city fell, and in the earthquake were slain of men seven thousand: and the remnant were affrighted, and gave glory to the God of heaven.
14 The second woe is past; and, behold, the third woe cometh quickly.
15 And the seventh angel sounded; and there were great voices in heaven, saying, The kingdoms of this world are become the kingdoms of our Lord, and of his Christ; and he shall reign for ever and ever.
16 And the four and twenty elders, which sat before God on their seats, fell upon their faces, and worshipped God,
17 Saying, We give thee thanks, O Lord God Almighty, which art, and wast, and art to come; because thou hast taken to thee thy great power, and hast reigned.
18 And the nations were angry, and thy wrath is come, and the time of the dead, that they should be judged, and that thou shouldest give reward unto thy servants the prophets, and to the saints, and them that fear thy name, small and great; and shouldest destroy them which destroy the earth.
19 And the temple of God was opened in heaven, and there was seen in his temple the ark of his testament: and there were lightnings, and voices, and thunderings, and an earthquake, and great hail.”
Question #26 – Why Is Hydra Bulgares In the COVID-19 Vaccines?
Learn more about Hydra Bulgares https://biology.ucdavis.edu/news-events/model-organisms/hydra https://biology.ucdavis.edu/news/1-million-keck-foundation-grant-backs-research-build-brain
Listen to Kim Clement Prophecies: https://www.youtube.com/watch?v=WxvPiERZSQo
The Poem Referenced by Dr. Zelenko:
“Do you believe in life after delivery?” The other replied, “Why, of course. There has to be something after delivery. Maybe we are here to prepare ourselves for what we will be later.”
“Nonsense” said the first. “There is no life after delivery. What kind of life would that be?”
The second said, “I don’t know, but there will be more light than here. Maybe we will walk with our legs and eat from our mouths. Maybe we will have other senses that we can’t understand now.”
The first replied, “That is absurd. Walking is impossible. And eating with our mouths? Ridiculous! The umbilical cord supplies nutrition and everything we need. But the umbilical cord is so short. Life after delivery is to be logically excluded.”
The second insisted, “Well I think there is something and maybe it’s different than it is here. Maybe we won’t need this physical cord anymore.”
The first replied, “Nonsense. And moreover if there is life, then why has no one has ever come back from there? Delivery is the end of life, and in the after-delivery there is nothing but darkness and silence and oblivion. It takes us nowhere.”
“Well, I don’t know,” said the second, “but certainly we will meet Mother and she will take care of us.”
The first replied “Mother? You actually believe in Mother? That’s laughable. If Mother exists then where is She now?”
The second said, “She is all around us. We are surrounded by her. We are of Her. It is in Her that we live. Without Her this world would not and could not exist.”
Said the first: “Well I don’t see Her, so it is only logical that She doesn’t exist.”
To which the second replied, “Sometimes, when you’re in silence and you focus and you really listen, you can perceive Her presence, and you can hear Her loving voice, calling down from above.”
– Útmutató a Léleknek
Eric Trump, Lance Walnau, Dr. David Martin, Comedian Jim Breuer, Dr. Vladimir Zelenko, Del Bigtree, Dr. Peter McCullough, Sean Feucht, Karen Kingston, Debbie G. Are Joining the ReAwaken America Tour!!!
STORY AT-A-GLANCE
The Awareness Foundation COVID-19 Roundtable is a sign of wakefulness and hope during times of censorship and suppression
It includes honest opinions and expertise from 14 high-profile doctors, including myself, with a focus on the potential dangers being posed by the experimental mass COVID-19 vaccination campaign
Experts discuss how COVID-19 vaccines may cause a coming tsunami of hospitalization and deaths, along with debilitating chronic disease, early signs of which are already appearing
All agree that there’s enough evidence to halt the global COVID-19 vaccination campaign, either for everyone or — particularly — for those to whom the vaccines pose the greatest risks with little to no benefit, namely children and young people, pregnant women and those who have already recovered from COVID-19
In this time of extreme censorship and suppression of scientific debate, The Awareness Foundation COVID-19 Roundtable,1 hosted by Katherine Macbean of the Awareness Foundation, is a sign of wakefulness and hope. It includes honest opinions and expertise from 14 high-profile doctors, including myself, with a focus on the potential dangers being posed by the experimental mass COVID-19 vaccination campaign.
Each has faced censorship when speaking out, and though there are some differing viewpoints, all agree that there’s enough evidence to halt the global COVID-19 vaccination campaign, either for everyone or — particularly — for those to whom the vaccines pose the greatest risks with little to no benefit. This includes children and young people, pregnant women and those who have already recovered from COVID-19.
I highly recommend setting aside two hours to watch this roundtable discussion in full — it’s a rarity in the present day to hear such candor and open debate. However, I’ve also compiled some of the highlights below, which include warnings about the dangers these experimental vaccines may pose to society.
A Tsunami of Chronic Disease and Death
Will COVID-19 vaccines cause a coming tsunami of hospitalization and deaths, along with debilitating chronic disease? One expert on the panel, Dr. Peter McCullough, an internist, cardiologist, epidemiologist and full professor of medicine at Texas A&M College of Medicine in Dallas with a master’s degree in public health, said he’s focused more on the short-term adverse effects from the shot. These nonfatal injuries fall into four major categories:
Neurologic
Immunologic
Hematologic
Cardiac
“What I’m seeing is just the late emergence of various neurologic syndromes. And it probably depends on where the seeding occurs of, uh, of, you know, the uptake of the genetic material in the brain or support cells in the brain, but there’s a whole variety of cerebral, cerebellar, even peripheral nervous system abnormalities,” McCullough said, adding:2
“I’ve seen it in my clinic and they seem to be emerging three, four or five, six months later after vaccination … So I’m getting increasingly alarmed here that this is not just a simple one- or two-day problem. And so there’s great concern, particularly in younger kids that over a course of three or six or nine months, they’ll end up with heart failure or cardiac death.
… What I see is, potentially from these signals, not mass death, but just a large number of Americans and people around the world with a new chronic disease of some sort of neurodegenerative disease or cardiac disease. The patients that I’m aware of, these problems seem to be quite disabling.”
Another panel member, Dr. Vladimir Zelenko, who has treated thousands of COVID-19 patients using hydroxychloroquine (HCQ), azithromycin and zinc sulfate,3 with great success, has a different take. He believes there is a very distinct possibility that everyone who receives the COVID jab may die from complications in the next two to three years:4
“I’m just going to give you the perspective of a clinician who deals with people that are dying … 4 million dead people can testify to the unique clinical syndrome to put them there. Basically, a natural animal virus was changed to infect humans, and then its lethality was augmented to cause blood clots and lung damage.
And in concept here, we’re dealing with a Hitler/Stalin type of mentality with weapons of mass destruction and the way to win this war — and it’s very winnable — is in the following manner. It’s a narrative war. So we need to spread the following two ideas … Don’t give into the fear and choose to destroy yourself, No. 1. No. 2, treat your problem early. If these two ideas could penetrate the fixed calls of humanity, then it’s really the end of this crisis.”
Dr. Tess Lawrie, whose company The Evidence-Based Medicine Consultancy has worked with the World Health Organization, agreed that the vaccines are unsafe for children and adults alike:5
“They’re actually not safe for anybody, and it’s clear. The databases are screaming. The databases are early warning systems, and the databases around the world are screaming that we are facing a tsunami of chronic disease.”
Inflammatory Disorders, Cancer Markers on the Rise
Dr. Richard Urso, an ophthalmologist in Houston, Texas, is also concerned:6
“Early on, we were seeing things, mostly thrombotic, but later, as we get into two and three months [after vaccination], we’re seeing a lot of inflammatory issues. I’ve had a host of people with inflammatory ocular disorders, as well as having orbital inflammatory diseases.
I typically don’t see this rash number of people. For people who don’t know, my clinical practice is probably one of the largest in the United States, if not the largest, and we get a tremendous number, in volume, of patients who come through our office. And I’m seeing late inflammatory disease, and it responds quite well to inflammatory medicines.”
Some have brushed off the notion that the virus could be a bioweapon because it didn’t cause sudden, mass deaths. But this is a misconception. A successful bioweapon can be something that causes long-term, progressive, chronic-type diseases, noted Dr. Richard Fleming, a physicist, nuclear cardiologist and attorney.
In 1994, Fleming introduced the theory of inflammation and vascular disease, which explains why these inflammable thrombotic diseases, and the causes, including viruses like SARS-CoV-2, produce disease states like COVID-19.
“As I laid out in the theory in 1994,” Fleming said, “you’re going to see an inflammable thrombotic response. That’s the primary thing that people are noticing, be that heart disease or retinol disease.” The other factor is a prion component of this virus, “which is also a chronic smoldering disease.” Fleming noted:7
“If you’re going to actually develop something that’s going to have a massive effect on your ‘enemy,’ your goal isn’t to kill the enemy any more than it was the goal of the United States in Vietnam to kill the enemy.
The goal was to maim the enemy so that more of the enemy would be taken off the field. What we’ve seen is something that’s been implemented that is an ideal by a weapon designed to demoralize and to feed people the enemy, and to cause a slow smoldering process.”
Fleming cited data from Pfizer that showed in the 12 to 14 days following the second injection of the Pfizer mRNA vaccine, elderly individuals had a 2.6-fold increase in symptoms of Alzheimer’s disease. “This is an inflammable thrombotic process affecting every organ system and prion diseases that not only affect the brain, but also affect the heart and other vital organs of the body.”8
Dr. Ryan Cole, a Mayo Clinic-trained, triple-boarded pathologist, also said that he’s seeing potential cancer-causing changes, including decreases in receptors that keep cancer in check, and other adverse events post-vaccine:9
“I’m seeing countless adverse reactions … it’s really post-vaccine immunodeficiency syndrome … I’m seeing a marked increase in herpetic family viruses, human papilloma viruses in the post-vaccinated. I’m seeing a marked uptick in a laboratory setting from what I see year over year of an increase of usually quiescent diseases.
In addition to that — and correlation is not causation — but in the last six months I have seen — you know, I read a fair amount of women’s health biopsies — about a 10- to 20-fold increase of uterine cancer compared to what I see on an annual basis. Now we know that the CD8 cells are one of our T-cells to keep our cancers in check.
I am seeing early signals … what I’m seeing is an early signal in the laboratory setting that post-vaccinated patients are having diseases that we normally don’t see at rates that are already early considerably alarming.”
Do the Vaccinated Pose a Risk to the Unvaccinated?
Sherri Tenpenny has heard thousands of anecdotal reports that something is being transmitted from the vaccinated to the unvaccinated:10
“We’re injecting a synthetically made messenger RNA and strips of synthetically made double-stranded DNA by different mechanisms, and if that transmission goes to the other person, they don’t get COVID, they don’t get COVID symptoms that we typically recognize as COVID. They get bleeding, they get blood clots, they get headaches, they get heart disease, they get all of these different things.”
Dr. Robert Malone, the inventor of the mRNA and DNA vaccine core platform technology,11 doesn’t agree that anything is being “passed” from vaccinated people to others, adding that while it may be possible for mRNA to be shed through breast milk to nursing infants, possibly causing gastrointestinal symptoms, anything else is just speculation.
Others suggest it could be more of a hormonal or pheromonal issue than some type of “shedding,” which may help explain why women are also reporting abnormalities with their menstrual cycles following vaccination. Dr. Lee Merritt, an orthopedic and spinal surgeon, brought up a 2015 report by the U.S. Food and Drug Administration, which looked at “shedding” in mRNA vaccines, which they call gene therapies.12 She explained:13
“They talk about, they’re very concerned about the shedding — and they do call it shedding, whether that’s technically correct … And they tell you in this thing who to protect, they tell you to protect neonates, immunocompromised people and elderly with bad immune systems.
They also say, we don’t know what’s being shed. They say it could be genetic material. It could be activated viruses and it could be a recombinant product. This is what’s in the FDA data.”
Immediately Halt the Vaccine Program
All of the experts agreed that evidence suggests the mass COVID-19 vaccination program should be halted. “There is enough evidence now just from the European Medicines Agency alone, 1.7 million in reported adverse events and 17,000 deaths that the four clinical trials should be stopped,” said Dolores Cahill, a professor at the school of medicine at the University College Dublin.
“They are detailed in the classifications, cardiac related immune, uh neuropathological and fertility associated.
So I think we all have duties as doctors and scientists to say, if something is causing more harm than good, which this clearly is, we should, I think, unify and called for a stop to the clinical trials worldwide, and also that any individual prime ministers and regulators that continue the trial would have to be liable for any adverse events.”
Malone believes that the vaccines have merit for certain populations, namely the elderly, but is advocating for prohibition on vaccination for infants and newborns, through young adults up to ages 30 to 35. “And specifically,” he said, “I’m trying to stop this crazy effort to force universities and schools to have universal vaccination.” In addition, he added:
“We can argue about risk-benefit for elderly, but the risk-benefit ratio for newborns through young adults is explicitly clear. It is upside down. It’s not subtle there. You’re going to kill more. And, and personally, I also feel that we can dig in really hard on the reproductive health in pregnancy, in women, that there just aren’t data to support the use of this product because of the potential female reproductive health consequences.”
Dr. Urso added the other significant population that has far more to risk than gain from vaccination: the COVID-recovered. “The immune status should be more important than the vaccination status,” he said.
“So I think there’s three groups that are easily winnable arguments [to avoid vaccination]: pregnant women, the young and … the COVID recovered … I mean, that’s a, that’s a lousy thing to do to get all these people that are COVID recovered, good immune status and give them a vaccination for something they don’t need.”
How to End Fear and Optimize Your Immune System
The roundtable participants are planning to continue their discussion offline to formally request an end to mass COVID-19 vaccination for the mentioned groups as well as create a statement to end government interference with the practice of medicine. Many physicians have had their hands tied when it comes to prescribing early treatments for COVID-19, like ivermectin. As Fleming noted:
“… The reason why people die with COVID is because they’re not receiving treatment, so I would argue that we need to make certain that people, the physicians, are allowed to treat without government interference and that we put a hold on the dissemination of the vaccines at this point in time, until we can further investigate them safely.”
Dr. Sam White, whose reputation has been under attack since he released a video on social media detailing his concerns about the suppression of the science around therapeutics in the U.K., added:
“We could end the fear overnight by allowing access to therapeutics and changing the mainstream media narrative that there’s no need for masks. There’s no need for lock downs. This is more treatable than flu, as far as I’m concerned, we’re just not allowed to do any treatment. If the public knew that it changes the narrative overnight.”
While we work on changing the narrative, or at least opening up discussions of science outside of the narrative, it’s always a good idea to optimize your immune system.
Toward this end, I recommend optimizing your vitamin D levels to 60 to 80 nanograms per milliliter and improving your metabolic flexibility so your body can seamlessly transition between burning fats and glucose as your primary fuel. One way to do this is to condense your eating window to about six to eight hours a day.
Even without changing your calories, this can make a profound difference, but from a perspective of choosing the right foods, one of the most important strategies that I’ve learned over my four decades of studying this is to avoid processed foods, nearly all of which are loaded with vegetable, or seed, oils.
These oils have a high content of linoleic acid, which contributes to mitochondrial instability and increases susceptibility to oxidative stress. This, in turn, increases immune dysfunction and mitochondrial dysfunction. These are simple strategies I recommend, as they’re useful to improve your overall health and resiliency to fight any infection.
As mentioned, I highly recommend listening to the discussion in full to get all of the details that weren’t included here. At the next meeting, the group plans to discuss how to move forward to challenge the narrative in greater detail, including fighting back against the organizations, such as the Wellcome Trust and the Bill & Melinda Gates Foundation, that are heavily investing in this.
French virologist & Nobel prize winner Professor Luc Montagnier gets the hero’s welcome on his arrival to today’s protest;
Montagnier: “The non vaccinated will save humanity”.
“There are images, also extraordinary for me, of small bacteria even in the intestine, which are full of viruses. And this is a battle between bacteria and viruses, which must be defeated even with proper nutrition and hygiene. It is not just the vaccine that will cure it, but it is the combination of treatments that will eliminate this disease. There was a huge strategic mistake, something was synthesized and isolated, a huge strategic mistake.
Contrary to what was said at the beginning, these vaccines do not protect absolutely, and this is coming slowly. This is scientifically recognized by all today.
I ask all my colleagues to absolutely stop vaccinating with this type of vaccine.
Doctors today are perfectly informed of what I am saying, and therefore they should intervene immediately because the future of humanity is at stake. Many countries have forgotten about treatments, there is not only the vaccine, there are drugs that have not been used and that work very well, such as antibiotics.
It depends on you, above all on you not vaccinated that a tomorrow they will be able to save humanity. Only the unvaccinated will be able to save the vaccinated.
Vaccinated who will, in any case, contact the medical centers to be saved.
We must avoid listening and giving a voice to those who do not have the right to do so and let science speak. I repeat: it is the unvaccinated who will be able to save humanity.
At the beginning, the large pharmaceutical multinationals were very interested in vaccines for an economic issue.
The research continues, and I and my whole team continue to research this virus. The research does not stop, we have not yet reached the point. Man will win if he focuses on the law of nature and only on that. Every citizen is free and must also follow political ideas, take advantage of the upcoming elections to express your opinion.
What would I say to a young person today? You absolutely must act, each of you, and find the truth hidden behind the lies. Long live freedom “.
Dr. Ardis on Hospital, Fauci, Myocarditis Scandals! CirstenW Truth.
Dr. Ardis Immune-C & Achne Treatments:
thedrardisshow.com/shop-all/
Use Promo Code B2T to save 10% off your order
Help Mike Lindell fight! See over 100 products here: https://www.mypillow.com Promo Code: B2T (up to 65%+ off)
Show Smartmatic and the Cancel Left They Won’t Win!
Join Rick to help the hurting! Free Group platform: https://b2tneighborhood.com
Christian Patriot Platform! Facebook for the Remnant!
Dozens of peer-reviewed studies show that when COVID-19 is treated within the first few days of symptom onset, there’s an 85% reduction in hospitalization and death
With Omicron, we have been gifted a best-case scenario. The highly contagious virus can rip through the population, causing only mild cold symptoms, thus producing herd immunity without the risk of mass casualties
Two months before the rollout of the COVID shots, the U.S. Food and Drug Administration was aware that they could cause serious problems, including heart attacks, strokes, myocarditis, blood clots, neurological problems and more, yet they pushed them anyway
Dr. Vladimir Zelenko believes SARS-CoV-2 is a bioweapon. Patents spanning two decades support this view. Those who created the weapon also investigated and identified antidotes, which includes the zinc ionophore hydroxychloroquine
The antidote to COVID was intentionally suppressed to encourage people to get the COVID jab, which Zelenko believes is a tool to tag people for the New World Order slave system
Dr. Vladimir Zelenko, whom I’ve interviewed twice previously, was among the first U.S. physicians to develop an early treatment program for the novel SARS-CoV-2 infection. He popularized the use of hydroxychloroquine and zinc, and when hydroxychloroquine became increasingly difficult to obtain, he was also among the first to identify quercetin as a viable alternative.
When the pandemic started, Zelenko was practicing in New York. He has since moved to Florida, where he’s been giving interviews for several hours a day, trying to spread the word about early treatment and prevention. As noted by Zelenko:
“It’s a very treatable infection — or should I say bioweapon? — if done within the first few days, because COVID is two diseases. It’s the infectious stage of the virus, and then a week later, you have the pathogenic inflammatory reaction that does all the damage to the lungs and causes blood clots.
So, it’s all about timing. And the data is very clear. There are dozens of peer-reviewed studies that prove if you treat COVID within the first few days, you have an 85% reduction in hospitalization and death. It’s a no-brainer. You could have saved 700,000 people from going to the hospital out of 800,000.”
While licensed to practice medicine in Florida, Zelenko now spends most of his time educating the public and other doctors. He’s also available via telemedicine, but his passion has become researching and developing simple, natural approaches to complex health problems — including his own.
The Road Less Traveled
Zelenko has a rare type of cancer called pulmonary artery sarcoma, which is typically fatal. He’s also undergone two open-heart surgeries and three years of chemo and radiation, none of which has resolved his problems.
“Almost four years ago, I was diagnosed with pulmonary artery sarcoma. There are only 10 cases on average per year, and they’re all found at autopsy. In my case, they thought it was a blood clot that didn’t respond to blood-thinning medication.
So, the decision was made to do an embolectomy, open my chest, go into the pulmonary artery and take out the blood clot. But when they did that, they saw it was a tumor, and it had completely destroyed my right lung. So, I lost my right lung. And they resected a large part of the pulmonary artery and had to reconstruct it because you need that artery to live.
Then I was in chemo … I was pretty good for two years, and then it came back and had spread to my hip as well. And so, I had another open-heart surgery. They had to replace one of my heart valves, pulmonic valve. Then I went for radiation to my hip [followed by] really heavy chemo.
After two months on that, I went into congestive heart failure and developed cardiomyopathy … I recovered from that, and was put on heart failure medication … A month after that … I developed COVID pneumonia … I was pretty sure I was going to leave in a box, yet I recovered.
A few months later, I went for another CT scan, and they found, again, the tumor was back in the pulmonary artery, but this time, no doctor wanted to operate on me. A third open-heart procedure is very dangerous. They estimated more than 50% likelihood I would die on the table, which I didn’t like. So, I ended up having pretty intense radiation to my mediastinum, where the tumor was.
That’s when you came into the picture, in terms of advising me about treatment. I ended up having immunotherapy in Europe for two months with checkpoint inhibitors, but also hyperthermia and mistletoe injections, and alpha lipoic acid, high-dose vitamin C [infusions] and different other modalities. And I feel better than ever.
I had a CT scan last week, and it showed the tumor shrank by one-third. I spoke to the radiation oncologist who told me that a good result would’ve been the same size or smaller. It takes years to resolve. So, time will tell, but it’s easier for me to walk, and hemodynamically I’m more stable, and I feel good. Amen.”
The Surprising Role of Immunotherapy in Cancer
Overall, the “COVID story has completely changed the way I look at life,” Zelenko says. When he saw how natural, effective, over-the-counter solutions for COVID were suppressed, while experimental gene transfer shots were pushed, he realized other treatments might also be suppressed, such as cancer treatments.
“Probably, effective approaches were marginalized in lieu of the more expensive pharmaceutical approaches,” he says. “I’ll give you one example. Dr. [William] Coley was an oncological surgeon who lived around 100 years ago, maybe 120 years ago. He noticed that he would operate on his patients, and the tumor would come back and they would die. And then he observed something very interesting.
He had a patient with pancreatic cancer, Stage 4, inoperable. That patient got very sick with an infection and became septic. He almost died, but he recovered and his tumor went away. He noticed that type of phenomenon a few more times, and realized that there must be some immune reaction, immune response to the infection that wakes up the immune system to also attack the tumor.
So basically, in my opinion, that was the birth of immunotherapy. Fever seems to play a role. It seems to have antitumor properties, as well as activating certain parts of your immune system. So, it’s fascinating. And that information was buried for a good long time — 50, 60 years — until some doctors rediscovered it and started doing research. And I benefited from that in Europe.”
Hyperthermic Treatment for Cancer
We’ve come a long way since the days of Coley, who used toxins to trigger infection and fever. Today, hyperthermic treatment is used instead. Basically, it’s all about raising your body temperature to about 104 degrees Fahrenheit for four to six hours. Zelenko describes the treatment he underwent:
“It was quite an experience, having a temperature around 40 Celsius, let’s say 104 degrees Fahrenheit, for five hours. You become a little loopy and a little anxious, but I drank a lot of fluids and had a nurse with me all the time. It was a pretty interesting experience.
There were whole-body hyperthermia machines and localized hyperthermia. Both are basically a fancy sauna. It was like a spa actually. I did enjoy the treatment in most cases.”
As an aside, I sincerely believe sauna bathing is one of the most powerful biohacks available. I do it four times a week. I get my temperature up to about 102 degrees F. or so, for 20 minutes. I’ve found it to be a profoundly effective health habit to nip infections in the bud, and may also help put the brakes on any potential malignancies. I am currently using a prototype full-spectrum SaunaSpace sauna that is EMF-free, has eight 250 watt bulbs and will likely be available later this year.
Omicron Is Unstoppable, But Not To Be Feared
Getting back to the issue of COVID, over the past two years, the SARS-CoV-2 infection has gone through a number of changes. Omicron, for example, is far more contagious, but has far less severe symptoms. As noted by Zelenko:
“Omicron is unstoppable. It’s more infectious than measles. Everyone’s going to get it. Sorry, but that’s the case. However, it seems to attack only the upper airway in most cases, and there are very few deaths. It’s very responsive to treatment as well, so there’s no reason to be afraid of it.”
In fact, we appear to have been gifted a best-case scenario, in which a highly contagious virus will rip through the population, causing only mild cold symptoms, thus producing herd immunity without the risk of mass casualties. “When two-thirds of the population gets through it, it essentially shuts down the pandemic,” Zelenko says.
Vaccinating During a Pandemic Breeds Variants
In the interview, Zelenko explains how the many variants we’ve seen have probably been a result of the mass “vaccination” campaign.
Three respected immunologists, Dr. Luc Montagnier (who won the Nobel Prize in 2008 for his discovery of the HIV virus), Dr. Sucharit Bhakdi, the most published immunologist in history, and Dr. Geert Vanden Bossche, a top immunologist in The Netherlands, have all warned that when you mass vaccinate in the middle of an active outbreak, you cause variants to emerge.
“You exert evolutionary pressure and breed more varying viruses,” Zelenko says. “Now, there are two or three possibilities. One could be that it was unintentional. Good, well-meaning people developed what they thought would help — a vaccine. However, giving it to people during a pandemic has been an absolute failure. ‘Oops, we’re sorry.’ That’s one possibility.
The other possibility is that whoever has orchestrated this knows exactly what they’re doing, and they are doing it on purpose to maintain the new variants and the consequences of that, which is essentially a psyop [to cause] a global psychosis due to fear, lockdowns and wearing a face diaper.
There’s one more possibility. There’s no dispute; everyone who knows the facts and has studied the issue knows that COVID-19 is a weapon made in a laboratory. Gain-of-function research is nothing more than making a weapon of mass destruction and genocide, and there’s a patent trail 20 years long that documents the different stages of development of this weapon.
And here’s my supposition. I have no evidence of this, but I could say the following: If I could make the original virus, I could make variants. It’s very easy. You just change a few sequences of the code that goes with the spike protein. You change its three-dimensional shape, and if you do it enough, eliminate existing antibodies.
So again, I don’t have evidence for that, but I do have evidence that [SARS-CoV-2] is an artificially-made bioweapon. So why wouldn’t it be possible to make variants the same way? I think it’s kind of a combination, multifactorial cause of variants — the natural God factor, the evolutionary pressure exerted by vaccinating people during an active pandemic, and then just outright making them.”
Antidotes to the Bioweapon Were Developed Beforehand
Zelenko goes on to recount a relatively recent realization. Back in March 2020, he saw a MedCram video, episode 34,1 in which Dr. Roger Seheult explained some of the principles that he then ended up building his COVID protocol on. Seheult specifically quoted a paper that explained the functioning of zinc ionophores.
That mechanism is what Zelenko relied upon when developing his own protocol. However, he didn’t realize until December 2021 that the author of that central paper was Dr. Ralph Baric. Why does that matter? Zelenko explains:
“In 1999, Ralph Baric, funded by the U.S. government, at the University of North Carolina at Chapel Hill, figured out how to take an animal virus and have it be able to infect other species, different animals, in other words, cross-species infection.
In 2015, the same Dr. Ralph Baric, and Dr. Zhengli [at the Wuhan Institute of Virology in China], funded by the National Institutes of Health, figured out how to make a corona bat virus infect human beings, and augmented its lethality to human lives. That was in 2015. But in 2010, Baric published that paper that I’m referring to.
So, the development of the weapon happened in stages, but before it was unleashed onto the human population, or the development of it being able to infect human beings, an antidote was made. Research paid for by the government was published.
The same people that made the bomb, let’s say, also created the antidote to diffuse the bomb. And then, when the pandemic arrived, doctors like myself, out of necessity, came up with creative solutions, based — in my case, unknowingly — on this work. And immediately, that information was marginalized and suppressed, and doctors were deplatformed for advocating for it.
So, the government who made the bomb also knew about the solution. And the reason why is they didn’t want to die. The stakeholders here don’t want their families to die. But for you and for me, they have a different agenda. So, they had that information.
I have knowledge that the Google executives are all taking hydroxychloroquine and ivermectin for prophylaxis, as is half of Congress. And so, the people that have orchestrated this knew the answer, and use it for themselves. Even doctors know the answer for themselves.
They prescribe [these drugs] for themselves, or they call me. But when patients come, they say there’s no treatment, go home, take Tylenol. So, this is mass murder.”
The COVID Jabs — Another Crime Against Humanity
In addition to killing untold numbers of people by denying and suppressing early treatment options, governments around the world are also killing people with the COVID jabs. A year into the aggressive campaign to inject as many people as possible, it’s likely the shots have killed more people than have died from the infection. It’s very difficult to tell, unfortunately, because the data are so seriously manipulated.
Zelenko estimates somewhere between 500,000 to 1 million Americans have been killed by the shots to date. Disturbingly, the U.S. Food and Drug Administration was aware that the shots could have serious consequences, yet they pushed them anyway. What’s more, they refuse to address the mindboggling number of adverse events reported to the Vaccine Adverse Events Reporting System (VAERS). The safety signal couldn’t possibly be clearer.
“In October, 2020, two months before the vaccine rollout, there was an internal presentation in the FDA to its scientists, and on slide 16 of that presentation, there was a list of side effects: death, heart attack, stroke, blood clots, horrific neurological diseases, myocarditis and many, many more,” Zelenko says.
“Now keep in mind, this is two months prior to the rollout. After the vaccines were rolled out, and a few months into it, when the VAERS database started showing the side effects that people were experiencing, there’s a 100% correlation with what that slide said would happen, and what actually happened to human beings.
That is premeditated mass murder. FDA knew exactly what it was doing. They knew exactly the side effects, and they released it anyway …”
What’s the Real Agenda?
Why would the FDA behave this way? Why aren’t they safeguarding public health from a clearly lethal treatment? And on the other hand, why aren’t they allowing doctors to help people with early treatment? Zelenko explains:
“In the mid-‘90s, it became obvious that the American economy was doomed. The Medicare and Social Security systems would become insolvent, and that would cause a tsunami-like effect nationally and internationally. And it was unstoppable. It was [mathematically inevitable].
Medicare, according to Congressional Budget Office, in 2027 will begin the process towards bankruptcy. So, security as of today [will last until] 2034. Now, the major stakeholders in the world economies saw an existential threat. They understood that their power and wealth was in real jeopardy.
And so a plan was developed, which was beyond the technology at that time, but the technology was being developed. So, for example, the Human Genome Project was mapped and completed.
Then CRISPR technology was developed, which is gene editing or gene splicing in very precise ways. That was sold as a way to cure genetic diseases. There’s a defective gene. You can just cut it out and splice in, cut and paste, basically, a healthy gene.
That’s the upside. The downside is that it creates possibilities to do gene editing for nefarious reasons. In 2015, Bill Gates said that the world population needs to be reduced by 15% through the use of vaccines because of global warming.
The same Bill Gates in 2020 said 7 billion people must be vaccinated. So, the obvious rhetorical question is, ‘Why would I take a vaccine for my health from someone who’s advocating the use of vaccines to reduce the world population?’
In 2016, Klaus Schwab, in an interview said something very strange. He said that within 10 years, by 2026, every single human being will be tagged with a digital identifier. What does that mean, and why?
Let’s go through the sequence of events. A bioweapon is made with an antidote, which is being suppressed and hidden. [The bioweapon] is released. It’s extremely easy to treat. However, that information is being suppressed, and access to those medications is being suppressed, and doctors who are advocating for it are being persecuted.
Anything that seems to give people hope, lessen anxiety, encourage reintegration with your loved ones seems to be immediately vilified, even early intervention. If you look at the NIH, they recommend, as of today, not to treat COVID unless they’re in the hospital with lung damage. Don’t do that.
And so, I was wondering, what is really going on? And why this incessant push to vaccinate everyone? Why jail doctors for using meds at work? Because it encourages the vaccine hesitancy.
Then I realized something. There were two patents that I became aware of. They’re separated by a year, but they’re linked in the puzzle, in the concept. One was August 31, 2021, that describes … nanotechnology engineering.2 It basically describes the following:
That there is the capability, the technology, already existing, in these vaccines that allows for the measurement of biometric data, meaning your heart rate, your respiratory rate, temperature, and then the transmission of that data with your location to a third party.
That didn’t even make sense to me. Like what? But then I realized there’s another patent owned by Microsoft. This one I remember by heart. It’s an international patent, WO202060606. You can’t make this stuff up. That patent describes linkage of biometric data transmission to cryptocurrency.
Then I got it. And by the way, 2026, when everyone’s supposed to be tagged with a digital ID, let’s call it an internal Auschwitz tattoo, is a year before the beginning of the insolvency of Medicare and the beginning of economic collapse. And so, the real agenda has become obvious to me.
It’s never been about health. COVID-19 is easy to treat. It was always about using fear and mass psychosis to get 7 billion people to willfully get injected with the technology that would permit them to participate in the new cryptocurrency-based system, the system that the world will use for finance.
Fiat currency and all the traditional ways of transactions will be gone. The only way that you actually will be able to participate in transactions, of buying bread, let’s say, is having a transmitting sensor of information with your location. It’s the mark of the beast, if you really want to know. With that, you can then buy bread for your family …
Gates and Schwab [are] both talking talk about how these vaccines change who you are. What does that mean? They explain it. [With] the gene editing technology, they are making the human better. That’s transhumanism. I call it Human 2.0. Human 1.0 is the version made by God. We are is imprinted [with God] in our genetic code. We’re made in the image of God because we have his code in us.
Now, would you give Bill Gates or Klaus Schwab the password to your home security system? Why would we give him access to our genetic code? Human 2.0, in the demented, depraved, deranged minds of these people is the next step up in the evolution of human beings. And I’m saying that if you allow that to happen to yourself, you’re no longer made in the image of God. You’re made in the image of Bill Gates and Klaus Schwab.”
A Ploy to Tag Us for the NWO’s Slave System
So, in summary, Zelenko believes that everything we’ve experienced so far — the aggressive marketing of the shots, the coercion and threats made to get as many injected as possible — has all been a ploy to “tag” as many people as possible in preparation for the New World Order’s cryptocurrency system, which will be managed by a small select group, and used to enslave all of humanity.
As noted by Zelenko, the World Economic Forum has publicly announced that by 2030, the U.S. will no longer be a superpower, and a few countries will be in charge of global governance. Now, how do you destabilize an economic engine like the U.S.?
“You create a pandemic,” Zelenko says. “You lock down middle class businesses, small businesses … But you leave Walmart and Home Depot open … It’s a wealth transfer from the middle class to the people in power. It’s a robbery, basically.
This is one big attempt at enslaving humanity. It’s a brilliant plan, by the way. It’s evil, but it’s brilliant because slavery has always been the most lucrative industry and asset throughout human history. Now is no different. And so, you have a few sociopaths who believe in their immortality and think that they’ll transfer their consciousness to some cyborg, enjoying the whole world as their playground.”
Zelenko goes on to discuss the statements inscribed on the Georgia Guidestones, a huge granite monument erected anonymously in a small town in Georgia, which lays out 10 commandments. The first one is that the world population should be reduced to and maintained at 500 million. If the COVID shots continue, it’s not inconceivable that the human population might be reduced to that size.
The Why Behind the Genocide
A few months ago, Elon Musk debuted his humanoid robots, saying that since these robots will eliminate 90% of the workforce, we therefore need universal basic income. This too is part of The Great Reset plan, which embraces both technocracy and transhumanism.
“Keep in mind that in the minds of these people, we’re not made in the divine [image]. We’re cockroaches. And they’re not going to throw endless universal income resources at cockroaches for too long. They’ll do it initially to identify the useless eaters, and then they will be liquidated. This has happened before.
Just 80 years ago you had the Nazi ideology based on eugenics, which created three classes of people. You have the ubermensch, what Nietzsche would call Superman. Then the mensch, which is the human, and then the untermensch, which is the subhuman. In the [Nazi] model, the [Nazis were] Supermen, descendants of Aryan gods. That gave them the power to enslave others.
So, for example, the Anglo-Saxons, basically Europeans, were meant to be slaves to the Aryans. And the subhumans, which I belong to — Jews, gypsies, Slavs, handicapped, political prisoners — we were meant to be vaporized, become dust.
That ideology did not go away. It resurfaced with the nuance that is not antisemitic right now. In a kind of an abstract way, we’re all Jews this time, because the hierarchy here is not based on religion or identity, but rather on the deranged belief that they’ve evolved, the Superman of this generation, into a higher level of consciousness.
They’re woke and they understand and are enlightened about the nature of the human condition. They’re custodians of the planet, and therefore it’s their responsibility to make sure the planet has solvency, that it continues to exist. And therefore, we have to reduce the world population.”
Cause for Optimism
While humanity is in a most precarious situation, Zelenko is optimistic about the future.
“I’ll tell you what I really think is going on,” he says. “There’s what we see, and then there’s the, let’s call it spiritual physics, at play. Karl Jung, the famous psychoanalyst, wrote, ‘The moral degradation of society begins with the degradation of the individual.’ From that, we can actually learn that moral improvement of society begins with improvement of the individual.
We, as a society, over the last 50, 60 years, have made some very bad choices. For example, we’ve desanctified or defiled gender roles … Marriage has lost its sanctity. The unborn are being massacred. In the Bible, there are two cities that were destroyed, Sodom and Gomorrah, and there’s an analysis why that happened. It wasn’t because of the immorality, because the whole world was immoral.
It was because they codified immorality into the law of the land. That’s exactly what has happened in [the U.S.] We’ve devolved … We worship the God of science, the god of technology, the god of money, god of power. Anything but [the true] God. And we are clearly practicing child sacrifice.
Dr. Michael Yeadon, former VP of Pfizer, told me personally, and then he actually publicized it, that for every one child that dies of COVID, 100 die from the vaccine. The [COVID shot] is 100 times more lethal to children than COVID. What do you call that? That’s child sacrifice.
So, I feel that, by way of analogy, we’re in the generation of flood. The house is going to get cleaned, and each individual is given a choice to get on the ark or not.
Or, to make it simpler, who do you bow down to? Do you bow down to your creator, who makes you in every instant of time? Do you ask [God] for fortitude, endurance, strength, resolve, the ability to deal with the unknown and fear? Or are you going to give in to the fear and bow down to corrupt sociopaths, oligarchs, corrupt governments, and the false promise of the golden calf of these vaccines?
Because at this point, in this country at least, no one’s holding you down and putting a needle into your arm. The majority of people, they want to travel by plane. They don’t want to lose their job. They want to go to school. It’s all these kinds of quality of life decisions. In other words, in a normal society, the parents sacrifice for the well-being of the children. In pagan societies, we sacrifice the children for the purpose of the adults.”
Peaceful Civil Disobedience Is the Answer
So, what’s the answer? Can we stop this transhumanist trajectory that threatens the very core of what makes us human? Can we prevent this plan for our enslavement from coming to fruition? Zelenko believes there is a way, as do I.
“The answer is we need organized civil disobedience. Do not comply. They can’t imprison everyone. They can’t fire everyone. They can’t expel everyone. They can’t lock down everyone. There’s many more of us than them. And actually, let me speak to the military leaders, to the police, to people that are charged to protect society.
You also have children. You also have parents. And we are relying on you to do what’s best for the citizens of this country, to protect us from all enemies, foreign and domestic. All we need to do is to coalesce with like-minded people. Take your kids out of school. Homeschool them. You can teach them morality.
The World Health Organization came out with an edict that if your kids go to school, that’s implied consent for the vaccine because you could have not sent them. And since you sent them to school, that’s implying that you’re consenting for them to be vaccinated, even without your knowledge.
Basically, we have to make small pockets, like cities of refuge, in a sense, of like-minded people; create an alternate society; do commerce with ourselves. I know there are forces really working hard to create an alternate cryptocurrency or blockchain system that is decentralized and would allow for people who don’t want to be tagged with a digital identifier to transact with each other.”
As noted by Zelenko, it’s becoming more and more obvious that the pandemic measures were never about protecting us from COVID. It was always about creating a new world order. It was about setting the stage for a Great Reset to “Build Back Better.”
But better for whom? The Build Back Better plan is about building “a society run by a few sociopaths and the rest of us enslaved,” Zelenko says. The good news is that more and more people are now starting to see this plan, and “once that realization reaches a certain threshold of people, countries are going to change and fall like dominoes,” he says.
As for when we might get our freedom back, that depends on us. As noted by Zelenko, “freedom isn’t free.” We were free (at least up until 2020) because our forefathers had the courage to confront tyranny. If we want our children to be free, we now have to display that same courage.
“Whether or not our children will be free depends on whether or not we are ready to sacrifice,” Zelenko says. “Are we ready, in this generation, to pay the price to ensure that our children thrive in freedom and have the ability to maintain God consciousness?
It’s going to happen. The unknown variable is to body count. I would hope that this interview reaches the consciousness of every single human being. People must choose to say no from this point on.”
In real time the human race and its modern civilization are being setup for premeditated extinction and collapse. Yet the bureaucratic country club members elected by We The People continue their comfortable compliance onslaught of the greatest national security threat the United States has ever known. Using the power afforded them to turn their backs and unleash the horrors of the Great Reset upon American citizens. All for a fleeting taste of power that will ultimately result in their own doom.
OAN has been taken off satellite, MyPillow has been de-banked, and the Justice department has declared that all Trump supporters are terrorists. TUNE IN to the most important broadcast in the history of Infowars.
The New World Order knows that America & Western Civilization are fighting to escape their tyrannical system! Now, globalists are set to stage terror attacks that will be blamed on populist movements as the pretext to carry out mass arrests of their opposition! Join Alex Jones with special guest Mancow Muller who is running for governor of Illinois! Also, an Oath Keeper whistleblower will take us inside the events that led to Jan 6 and the infamous false flag. Tune in NOW.
Be sure to join Alex Jones and Infowars on GETTR! Save the future and join the next Renaissance by following these accounts for breaking news and exclusive information today!
The COVID shots are based on the SARS-CoV-2 spike protein, which is the most pathogenic part of the virus, responsible for the worst symptoms of COVID-19, such as the abnormal blood clotting seen in severely ill patients
Pfizer’s and Moderna’s mRNA shots, and Janssen’s vector DNA shot, all inject genetic material into your body that program your cells to start producing this spike protein. They’re gene transfer technologies that instruct your body to produce a dangerous protein inside its own tissues
A Pfizer biodistribution study showed both the mRNA and spike protein is widely distributed in the body. In particular, it accumulates in the ovaries. Despite that, reproductive toxicology studies were eliminated in the interest of speed
The average number of adverse event reports following vaccination for the past 10 years has been about 39,000 annually for all vaccines combined, with an average of 155 deaths. The COVID jabs alone now account for 701,126 adverse events in U.S. territories as of December 17, 2021, including 9,476 deaths
Cases of myocarditis explode after the second shot, and disproportionally affect boys; 90% of post-jab myocarditis reports are males, and 85% of reports occurred after the second dose. Cases are also inversely correlated to age, with younger boys being at greater risk. The estimated incidence for post-jab cardiac adverse events is 162 per million for boys aged 12 through 15, and 94 per million for boys aged 16 to 17
In the video presentation above, Dr. Peter McCullough, a highly credentialed and published cardiologist, internist and epidemiologist, and one of the primary physicians leading the charge to provide commonsense clinical wisdom into COVID treatments, explains what the SARS-CoV-2 spike protein is and how it harms human biology — whether it comes from a natural SARS-CoV-2 infection or a COVID jab.
The presentation was given at the Burleson, Texas, COVID Symposium: A Legal Perspective, which streamed live December 3, 2021. He begins by addressing the necessity for safety whenever a new biologic product is launched. Safety is not something we can simply ignore, no matter what else is at stake. We must demand that whatever we’re given actually meets some kind of safety standard.
Warning bells started ringing in McCullough’s ears in the summer of 2020, long before the COVID shots were rolled out. “I was telling lawmakers that we’ve got a problem,” McCullough says, because corners were being cut that might result in a dangerous product. Safety studies, for example, were truncated down to a mere two months, which doesn’t allow for adequate evaluation.
Why Did They Use Spike Protein?
He also had several other concerns about the development program. Notably, the shots were based on the SARS-CoV-2 spike protein, which by then we already realized is the most pathogenic part of the virus, responsible for the worst symptoms of COVID-19, such as the abnormal blood clotting seen in severely ill patients.
As explained by McCullough, the virus can be illustrated as a ball with spike-like protrusions on its surface. Those spikes are what’s causing the problems.
“They had been genetically altered and engineered in a lab in Wuhan, China” McCullough says, “to be particularly infectious, and to be particularly dangerous when they get into the human body.
The last thing you want in your body is one of those [spike proteins], let alone billions of them because [they] damage the brain, they damage the heart, they damage bone marrow, they can tear up platelets and red blood cells. Very importantly, they damage blood vessels and cause blood clotting.”
Pfizer’s and Moderna’s mRNA shots, and Janssen’s vector DNA shot, all inject genetic material into your body that programs your cells to start producing the spike protein. They’re gene transfer technologies.
In short, the shots instruct your body to produce a dangerous protein inside its own tissues. “We’ve never done that before in the history of medicine,” McCullough says, and for good reason: It’s a bad idea. “It’s almost like a science fiction story going bad,” he says.
The idea is that by making your body produce this damaging spike protein, your body will react and fight it off, thereby creating immunity. However, in the process, the spike protein can do near-incomprehensible damage. In some people, the spike protein is lethal.
Uncontrolled Spike Protein Production
What’s more, we have uncontrolled production of spike protein, both in terms of quantity and time. The May 2021 paper,1 “Circulating SARS-CoV-2 Vaccine Antigen Detected in the Plasma of mRNA-1273 Vaccine Recipients,” proved the spike protein circulated in the blood stream for an average of 15 days’ post-injection. The longest was 29 days.
This refuted the claim that the mRNA simply stayed in the arm and didn’t circulate out of the injection site. Logically, that claim doesn’t make much sense, and the Japanese government, early on, demanded Pfizer do a study to show them where the injected mRNA actually goes.
Pfizer did that biodistribution study,2 which showed both the mRNA and spike protein were widely distributed in animals’ bodies. In particular, it was found to accumulate in the ovaries. Despite that, the Pfizer biodistribution data package reveals reproductive toxicology studies were eliminated in the interest of speed.
June 25, 2021, a paper was posted on the preprint server BioRxiv, showing the S1 portion of the spike protein remains detectable for up to 15 months after you recover from COVID-19.
“No wonder people have long-COVID syndrome,” McCullough says. “The body is trying to clean out this spike protein that’s not supposed to be there, 15 months after you’ve had the infection.”
McCullough points out that Bruce Patterson, the Stanford scientist who led that study, also continues to find the whole spike protein — both the S1 and S2 segments — in patients who got the COVID jab, months post-injection.
So, as of right now, we don’t know when the spike protein production ceases. What we do know, with great certainty, is that the spike protein damages the human body and contributes to both acute and chronic health conditions and diseases.
Australia has already purchased 14 doses of the COVID jabs for every person. This is meant to cover them for seven years, at one dose every six months. As noted by McCullough, some people simply aren’t going to survive that kind of continuous and ever-increasing onslaught of spike protein.
Urgent Questions on Vaccine Safety
Clear danger signals were apparent in April 2021, and May 24, 2021, McCullough published a paper along with 56 other international scientists in the journal Authorea.3
The paper, “SARS-CoV-2 Mass Vaccination: Urgent Questions on Vaccine Safety that Demand Answers from International Health Agencies, Regulatory Authorities, Governments and Vaccine Developers,” demanded the injections be pulled from the market unless or until safety concerns are addressed. Key clinical concerns raised include:
The potentially hazardous mechanisms of action of the shots resulting in cell, tissue and organ damage
The presence of harmful spike protein in donated blood
Lack of genotoxicity, teratogenicity and oncogenicity studies
The effects of bioaccumulation in women’s ovaries
The potential for reduced fertility
The lack of a data and safety monitoring board (DSMB) to oversee clinical trials and post-market surveillance
The lack of human ethics committee to oversee clinical trials
The lack of restrictions on exempted groups from randomized controlled trials (RCTs) such as pregnant women, women of childbearing potential, COVID survivors (previously immune)
The lack of risk stratification for hospitalization and death in the clinical trials
The lack of data transparency
The lack of public risk mitigation (early and at-home treatment options)
The paper was sent to every health and regulatory agency in the world. Here we are in early 2022 and, well, you can see what the response was. It’s been nonexistent.
A Critical Appraisal of VAERS
In October 2021, Jessica Rose, Ph.D., with the Institute for Pure and Applied Knowledge in Israel, published a report in the Science, Public Health Policy, and the Law journal.4 The report, “Critical Appraisal of VAERS Pharmacovigilance: Is the US Vaccine Adverse Event Reporting System (VAERS) a Functioning Pharmacovigilance System?” details three primary problems found:
Recoding of Medical Dictionary for Regulatory Activities (MeDRA) terms from severe to mild
It also includes bar plots showing the extreme difference between the COVID shots compared to all other vaccines on the market. If the shots were safe, the number of VAERS reports would remain relatively steady, not varying much from previous years, but what we see is a staggering spike in vaccine injuries reported in 2021.
The average number of adverse event reports following vaccination for the past 10 years has been about 39,000 annually, with an average of 155 deaths. That’s for all available vaccines combined.
The COVID jabs alone now account for 701,126 adverse events in U.S. territories as of December 17, 2021, including 9,476 deaths. If you include international reports that make their way into the VAERS system, we’re looking at 983,756 adverse event reports and 20,622 deaths.5
As staggering as these numbers are, they are just the tip of the iceberg. When you add in the underreporting factor, which is believed to be anywhere from five to 40, the numbers are simply astronomical.
VAERS is an early warning system and is supposed to alert our government to potentially hazardous vaccines once they’ve been rolled out. The signal from VAERS is so clear there’s simply no doubt we have a safety problem on our hands.
Can COVID Shots Cause Death?
As noted by McCullough, there’s a very tight temporality to the shots in most deaths. Half have occurred within 48 hours of injection, and 80% have died within one week of their jab (be it the first, second or third dose).6
Temporality is one of the 10 Bradford Hill criteria used to establish causal relationship. In order to be causative, one event must occur before another, and the shorter the duration between the two events, the higher the likelihood of a causative effect.
In June 2021, Scott McLachlan, Ph.D., at the University of London published an analysis7 of VAERS death reports concluding that 86% of post-jab deaths could be attributed to the shots. There was no other explanation for the deaths. McLachlan also looked at who’s getting killed by the shots and, sadly, it’s the same people the shots are intended to protect — our seniors.
In September 2021, Ronald Kostoff, Ph.D., published a report8 that also showed seniors were dying from the jab at far higher rates than other age groups. As noted by McCullough, this makes perfect sense because people die from COVID-19 due to the impact of the spike protein. Why would anyone assume they will survive having it produced in their own bodies?
Using the best-case scenario cost-benefit analysis, Kostoff estimates that people aged 65 and older are five times more likely to die of the COVID shot than from COVID-19 itself.
The reason for this is because if you take the shot, you’re guaranteed to be exposed to its risks, but you’re not guaranteed to get COVID-19 if you don’t take the shot. You may be exposed, or you may not. And not everyone develops a severe infection even when directly exposed.
COVID Jab-Associated Myocarditis in Children
In early September 2021, Tracy Beth Hoeg and colleagues posted an analysis9 of VAERS data on the preprint server medRxiv, showing that more than 86% of the children aged 12 to 17 who reported symptoms of myocarditis were severe enough to require hospitalization.
They also concluded that healthy boys have a “considerably higher” chance of being hospitalized with myocarditis post-jab than they are of requiring hospitalization for COVID-19.
According to McCullough, the FDA has heard these data twice in 2021 and never disputed them. Yet they’ve proceeded with recommendations to give the COVID jab to anyone with a pulse over the age of 5. It’s just shocking. Historically, as a rule, we’ve never given drugs to people when they’re more likely to harm than provide a benefit.
What Hoeg et. al.10 showed is that cases of myocarditis explode after the second shot, and disproportionally affect boys. A full 90% of post-jab myocarditis reports are males, and 85% of reports occurred after the second dose. According to Hoeg et. al.:11
“The estimated incidence of CAEs [cardiac adverse events] among boys aged 12-15 years following the second dose was 162 per million; the incidence among boys aged 16-17 years was 94 per million. The estimated incidence of CAEs among girls was 13 per million in both age groups.
The incidence of CAEs was considerably lower after the first dose across all age and sex groups. Median peak troponin was 5.2 ng/mL among boys aged 12-15 years, 11.6 ng/mL among boys aged 16-17 years, 0.8 ng/mL among girls aged 12-15 years, and 7.3 ng/mL among girls aged 16-17 years.”
Troponin Levels Reveal Massive Heart Damage
Troponin is a protein that helps regulate contractions of your heart and skeletal muscles. It’s a biomarker for heart damage, as your heart releases troponin in response to an injury. Elevated troponin is used to assess whether you’ve had a heart attack, for example.
Normal troponin levels are nearly undetectable, so even small increases can indicate heart damage. A level above 0.4 ng/mL is typically indicative of a heart attack and anything between 0.04 ng/mL and 0.4 ng/mL indicates there’s some kind of problem with the heart.12
So, the sky high post-jab troponin levels in these adolescent boys is anything but inconsequential. It can absolutely be life-threatening. Myocarditis can result in sudden death, as illustrated in an October 2021 case report13 from Korea, where the death of a 22-year-old man from acute myocarditis was causally linked to the Pfizer shot.
“Without a doubt, it will kill kids,” McCullough says. Even if not acutely lethal, myocarditis can significantly lower your life expectancy. Historically, the three- to five-year survival rate for myocarditis has ranged from 56% to 83%.14 That means a certain percentage don’t make it past five years because their heart is too damaged.
McCullough and Rose have also tried to publish an analysis on this topic. They submitted a paper15on myocarditis cases in VAERS following the COVID jabs to the journal Current Problems in Cardiology. But after initially accepting the paper, the journal suddenly changed its mind.
You can still find the pre-proof on Rose’s website though. What they show is that post-jab myocarditis is inversely correlated to age, so the risk gets higher the younger you are. They too found there’s a dose-dependent risk, with boys having a six-fold greater risk of myocarditis following the second dose.
Mortality in Adolescents Is Skyrocketing
McCullough’s assertion that the shot will kill some children is also starting to show in statistics. British data, for example, shows deaths among teenagers have spiked since that age group became eligible for the COVID shots.16
Between the week ending June 26 and the week ending September 18, 2020, 148 deaths were reported among 15- to 19-year-olds. During that same time period in 2021, 217 deaths occurred in that age group. That’s an increase of 47%, which has yet to be explained.
Deaths from COVID-19 also went up among 15- to 19-year-olds after the shots were rolled out. Significant concerns have been raised about the possibility that COVID jabs might worsen COVID-19 disease via antibody-dependent enhancement (ADE).17 Is that what’s going on here? As reported by The Exposé, which conducted the investigation:18
“Correlation does not equal causation, but it is extremely concerning to see that deaths have increased by 47% among teens over the age of 15, and COVID-19 deaths have also increased among this age group since they started receiving the COVID-19 vaccine, and it is perhaps one coincidence too far.”
COVID Jabs Double Risk of Acute Coronary Syndrome
Aside from troponin levels, researchers have also found Pfizer and Moderna mRNA COVID-19 shots dramatically increase other biomarkers associated with thrombosis, cardiomyopathy and other vascular events following injection.19
People who had received two doses of the mRNA jab more than doubled their five-year risk of acute coronary syndrome (ACS), the researchers found, driving it from an average of 11% to 25%. ACS is an umbrella term that includes not only heart attacks, but also a range of other conditions involving abruptly reduced blood flow to your heart.
In Months, the Jabs’ Effectiveness Wanes to Zero
As should be evident by now, there are significant risks to these COVID shots. But what about the benefit side of the equation? As noted by McCullough, while the shots reduce the risk of death from COVID-19, the benefit is vanishingly small.
A number of papers have been published calculating the absolute risk reduction of the shots, showing the four available COVID jabs in the U.S. provide an absolute risk reduction between just 0.7% and 1.3%.20,21
McCullough goes on to cite a December 1, 2021, New England Journal of Medicine study22 that compared the effectiveness of Pfizer’s and Moderna’s injections among hospitalized veterans. Here too, they found that the shots had an effectiveness of less than 1% against all COVID-19 events, over the course of six months.
As of the end of October 2021, we had 22 studies showing the shots’ efficacy against all variants rapidly wane over the course of three to six months, eventually hitting zero.
For example, a Swedish study23 published October 25, 2021, looked at data from 842,974 pairs, where each person who had received two COVID jabs was paired and compared against an unvaccinated individual, to see if the vaccinated had fewer symptomatic cases and hospitalizations.
Early on, the double-jabbed appeared to have decent protection, but that quickly changed. The Pfizer jab went from 92% effectiveness at Day 15 through 30, to 47% at Day 121 through 180, and zero from Day 201 onward. The Moderna shot had a similar trajectory, being estimated at 59% from Day 181 onward.
The AstraZeneca injection had a lower effectiveness out of the gate, waned faster than the mRNA shots, and had no detectable effectiveness as of Day 121. All the while, millions of Americans have already had COVID24 and have natural immunity that doesn’t wane in this manner.
“Vaccines aren’t viable if they can’t last a year!” McCullough exclaims. “The minimum criteria to accept a vaccine … is 50% coverage and it must last one year. These [COVID shots] aren’t cutting it. None of them are viable to be commercial products.”
The COVID-Jabbed Are Just as Infectious as the Unvaccinated
COVID jab mandates are even more irrational when you take into account the fact that they don’t prevent you from being infected, and studies have repeatedly shown that when you are infected, you have the same or higher viral load as unvaccinated individuals. What that means is you’re just as infectious as an unvaccinated person.
What’s more, as noted in a letter25 to the editor of The New England Journal of Medicine, the shots also have only minor influence on viral clearance. If you get the COVID shot and come down with COVID, you might be sick for a day or so less than someone who is unvaccinated.
We Must Treat COVID Patients Early
McCullough closes out his presentation going over the all-important issue of early treatment. You need to treat COVID early and aggressively. You also need to hit it from multiple sides. No single drug can effectively treat all aspects of this infection (although the Omicron variant does not appear to have any of the blood clotting and low oxygen issues associated with the earliest strains).
Very few people need die from COVID as long as they get appropriate treatment early enough. The fact that our health authorities are to this day refusing to acknowledge successful treatment protocols is nothing short of a crime.
If you want to live, and if you want your family and friends to live, you’d be wise to ignore the CDC’s and FDA’s recommendation to wait until you can’t breathe and then go to the hospital, where they’ll give you toxic remdesivir and lethal ventilation. Instead, arm yourself with one or more early treatment protocols and make sure you have the basics in your medicine cabinet. Protocols you can use include:
I reviewed all of these protocols and believe the FLCCC’s is the easiest and most effective. I’ve posted a summary of it below. However, I’ve altered some of the recommendations. Specifically, I recommend:
Decreasing zinc dose from 100 mg to 50 mg elemental zinc, but only for three days, then decrease to 15 mg elemental zinc.
Increasing quercetin from 250 mg to 500 mg.
Add NAC to 500 mg per day.
When using vitamin C, I recommend liposomal vitamin C, 1,000 to 2,000 mg, four to six times per day.
When using honey, make sure it’s raw, not normal honey from the grocery store. Raw honey can be obtained online or at a health food store.
Add fibrinolytic enzymes like lumbrokinase, serrapeptidase or nattokinase, two to four tablets, two to three times a day, on an empty stomach (one hour before or two hours after a meal). This will help break down any microclots and can be used in lieu of aspirin.
I’ve also added a couple of therapies that they have yet to include:
Nebulized hydrogen peroxide — Nebulize 5 ml of 0.1% peroxide dissolved in 0.9% normal saline every hour or two. It’s best to use a nebulizer that plugs into the wall, as these are more effective than battery operated ones.
Intravenous ozone administered by a trained ozone physician.
Founders of “The Corona Committee” are waging a legal battle to stop this global depopulation agenda of the Sociopaths and Psychopaths creating a massive trail of blood and death.
An independent non-profit alliance of doctors, nurses, healthcare professionals and staff around the world who have united in the wake of the Covid-19 response chapter to share experiences…
Since the beginning of the pandemic, experts have warned that the PCR test is not as a valid diagnostic and produces far too many false positives, as it can pick up on “dead,” nonreplicating viral debris
The U.S. Centers for Disease Control and Prevention now admits the PCR test can remain positive for up to 12 weeks after infection. For this reason, they say most people don’t need to retest negative before ending their quarantine
The CDC also admits the PCR cannot identify active infection or measure contagiousness
People who are double-jabbed or unvaccinated and test positive for SARS-CoV-2, or have known exposure, but remain asymptomatic, now only need to isolate for five days rather than 10, but should wear a mask for another five days when at work or in public. People who are triple-jabbed do not need to isolate after exposure, but should wear a mask for 10 days
Health care workers who test positive for COVID but remain asymptomatic can return to work after seven days with a negative test, but isolation time can be cut to five days if there are staffing shortages
From the earliest days of the COVID pandemic, the PCR test has been a source of unrelenting controversy, with experts repeatedly pointing out that it’s not a valid diagnostic and produces inordinate amounts of false positives.
Importantly, a PCR test cannot distinguish between “live” viruses and inactive (noninfectious) viral particles. This is why it cannot be used as a diagnostic tool. As explained by Dr. Lee Merritt in her August 2020 Doctors for Disaster Preparedness1 lecture, media and public health officials appear to have purposefully conflated “cases” or positive tests with the actual illness in order to create the appearance of a pandemic.
Furthermore, a PCR test cannot confirm that SARS-CoV-2 is the causative agent for clinical symptoms as the test cannot rule out diseases caused by other bacterial or viral pathogens. The inventor of the PCR test, Kary Mullis, who won a Nobel Prize for his work, explains this in the video above.
Almost universally, health authorities have also instructed labs to use excessively high cycle thresholds (CTs) — i.e., the number of amplification cycles used to detect RNA particles — thereby ensuring a maximum of false positives.
From the start, experts noted that a CT over 35 is scientifically unjustifiable,2,3,4 yet the U.S. Food and Drug Administration and the U.S. Centers for Disease Control and Prevention recommended running PCR tests at a CT of 40,5 and the World Health Organization recommended a CT of 45.
The pandemic of false positives was then used by world governments to implement pandemic countermeasures that have destroyed the global economy, ruined countless lives, decimated the education of an entire generation and stripped us of basic human rights and freedoms.
Time and again, the goal post for ending the pandemic theatre has been moved, and the justifications for continuing the life-destroying countermeasures have become increasingly laughable. The fearmongering over Omicron, for example, makes no rational sense based on the data available, which shows the variant is among the mildest so far, and far less likely to infect and damage the lungs.6
CDC Cuts Isolation Recommendation in Half
In the last days of December 2021, the U.S. Centers for Disease Control and Prevention issued yet another illogical protocol change.7 People who test positive for SARS-CoV-2, or have known exposure, but remain asymptomatic, now only need to isolate for five days rather than the previous 10, but should wear a mask for another five days when at work or in public. Also, they don’t need to get retested at the end of their quarantine. The stated reason? Because:
The majority of viral transmission (85% to 90%8) occurs in the first day or two before symptom onset, and two to three days after symptom onset9
The PCR test can remain positive for up to 12 weeks after you’ve recovered from the infection10,11
How is it that the CDC didn’t realize until now that the PCR test was picking up dead viral debris for three months after infection? The facts that the test, a) was far too sensitive, and b) couldn’t identify active infection, were criticisms from the start. What the CDC’s belated admission means is that, for the past two years, Americans have unnecessarily wasted time in self-isolation — perhaps weeks — waiting for a negative test.
In a December 30, 2021, appearance on MSNBC, Dr. Anthony Fauci responded to questions about the updated CDC guidance. CDC director Rochelle Walensky also tried to make sense of the new guidance in a December 29, 2021, ABC News interview (see videos above).12
Neither of them offered any explanation as for why the CDC didn’t change the rules sooner, and only now decided that keeping noninfectious people in isolation for days and weeks on end might not be so good after all.
Walensky did make a rather telling comment on CNN, though, when asked about the reasoning behind the shortened isolation guidance. “It really had a lot to do with what we thought people would be able to tolerate,” she said.13 Some have understandably translated that as “how much tyranny we thought people would be able to tolerate.”14
Differing Rules for Health Care Workers
The CDC has not given up on making the guidance as confusing as possible though. December 23, 2021, they also updated guidance for health care workers,15 stating that “Health care workers with COVID-19 who are asymptomatic can return to work after seven days with a negative test, and that isolation time can be cut further if there are staffing shortages.”16
In his MSNBC interview, Fauci was asked why health care workers are being treated differently, having to isolate for seven days rather than five, and still have to get a negative test, when the test can falsely remain positive for up to 12 weeks? What data supports this, and is it publicly available?
According to Fauci, the data to support this difference “is internal to the CDC,” but really, there’s “no specific data” to back it up, he adds. The CDC merely made “a judgment call.”
Double-Jabbed Treated the Same as Unvaccinated
The CDC’s updated guidance also puts those who have received two doses of the COVID shot in the same category as the unvaccinated, so when it comes to isolating after exposure, they have to follow the same rules, whereas those who have received a booster shot follow a different set of guidelines. As explained by the CDC:17
“For people who are unvaccinated or are more than six months out from their second mRNA dose (or more than 2 months after the J&J vaccine) and not yet boosted, CDC now recommends quarantine for 5 days followed by strict mask use for an additional 5 days.
Alternatively, if a 5-day quarantine is not feasible, it is imperative that an exposed person wear a well-fitting mask at all times when around others for 10 days after exposure. Individuals who have received their booster shot do not need to quarantine following an exposure, but should wear a mask for 10 days after the exposure.
For all those exposed, best practice would also include a test for SARS-CoV-2 at day 5 after exposure. If symptoms occur, individuals should immediately quarantine until a negative test confirms symptoms are not attributable to COVID-19.”
Fauci defended the decision to treat the double-jabbed as if they’re unvaccinated saying that those who have received a booster shot have far greater protection against the Omicron variant, compared to those who have only received one or two doses.
“When you’re infected, you’re infected,” Fauci said, and it doesn’t matter whether you’re vaccinated or not. The viral load is the same, so the risk of spreading the infection is the same. Those who have been boosted are less likely to be infected or carry a large viral load, hence they don’t need to isolate.
PCR Cannot Tell You Anything About Contagiousness
Fauci was also asked about how one can measure contagiousness. If the PCR can register positive for 12 weeks after an infection, it can’t be a reliable indicator of infectiousness. This was precisely the point that Mullis, inventor of the PCR test, attempted to make in the video at the top with respect to PCR and HIV.
So, how can we tell if we’re infectious or not? Fauci confirmed that the PCR can only tell you there’s a presence or absence of viral fragments, not whether it’s an active infection, or whether you’re actually infectious. He did not, however, provide an answer to the question as to how one can measure contagiousness.
Rapid Test Doesn’t Pick Up Omicron
Yet another confounding factor in this mess is that the rapid test apparently doesn’t pick up Omicron very well.18 Your viral load needs to be very high at the time of testing in order for the rapid test to recognize it.
This admission came within days of president Biden’s announcement that the federal government will distribute half a billion free rapid tests to homes around the country in 2022.19
It seems like a waste of resources, seeing how Omicron is starting to take over, but who knows, maybe it will pick up the common cold instead, allowing the “case” count to remain high enough to keep the charade going.
What’s the Real Death Count?
The CDC’s belated admission that the PCR test can’t identify active infection raises another question: What does this mean for those who died with a positive test? Did they actually have an active infection? If not, should they have been designated as COVID deaths?
The obvious answer to the last two questions is, of course, no. The vast majority were likely false positives, and the real death toll from COVID-19 considerably lower than we’re led to believe. The CDC undoubtedly knew this all along, seeing how they’ve been relentlessly criticized for their recommendation to run the PCR at a CT of 40. They’re trying to pretend that they just realized this, but that’s simply not believable.
Luc Montagnier, a French virologist and recipient of the 2008 Nobel Prize in Medicine for his discovery of the human immunodeficiency virus (HIV), has recently exposed the dangers of the COVID-19 vaccines. Montagnier discussed the issue in an interview with Pierre Barnérias of Hold-Up Media earlier this month, which was exclusively translated from French into English for RAIR Foundation USA.
The vaccines don’t stop the virus, argues the prominent virologist, they do the opposite — they “feed the virus,” and facilitate its development into stronger and more transmittable variants. These new virus variants will be more resistant to vaccination and may cause more health implications than their “original” versions.
During the interview, professor Montagnier referred to the vaccine program for the coronavirus as an “unacceptable mistake.” Mass vaccinations are a “scientific error as well as a medical error,” he said. “The history books will show that, because it is the vaccination that is creating the variants.” Montagnier explained that “there are antibodies, created by the vaccine,” forcing the virus to “find another solution” or die. This is where the variants are created. It is the variants that “are a production and result from the vaccination.”
Montagnier details that the mutation and strengthening of the virus occurs owing to the phenomenon known as Antibody Dependent Enhancement (ADE). ADE is a mechanism that increases the ability of a virus to enter cells and cause a worsening of the disease. ADE occurs when the antibodies generated during an immune response recognize and bind to a pathogen, but they are unable to prevent infection. Instead, these antibodies act as a “Trojan horse,” allowing the pathogen to get into cells and exacerbate the immune response.
In America, routinely recommended vaccines do not cause ADE. If they did, they would be removed from circulation. Phase III clinical trials of new vaccines are designed to uncover frequent or severe side effects before the vaccine is approved for use. Typically, it takes 2-4 years to assess whether a vaccine is safe, but with COVID-19 vaccines, manufacturers are spending around six months or less for testing.
According to the Cambridge University, ADE occurs in SARS-CoV-1, MERS, HIV, Zika, and Dengue virus infection and vaccination.
Data from around the world confirms ADE occurs in SARS-CoV-2, which causes COVID-19, says Montagnier. “You see it in each country, it’s the same: the curve of vaccination is followed by the curve of deaths. I’m following this closely and I am doing experiments at the Institute with patients who became sick with Corona after being vaccinated.”
In a medical documentary Hold Up: Return of the Chaos, released in France on November 11, 2020, Montagnier rejected the then-upcoming vaccine against COVID, saying he will not be vaccinated. “My conscience tells me not to,” he said. Montagnier also addressed his French colleagues, urging them “to uphold their [medical] titles as doctors, not as the sheep.”
The movie discusses the origins of the virus, criticizes harmful and irrational mask mandates as well as lockdowns, quarantines, abuses of government overreach, and explores effective COVID treatments such as hydroxychloroquine. The video was banned on YouTube, possibly because the creators imply the World Economic Forum used the pandemic to establish world dominance as a part of a global plan that is known as the Great Reset.
Montagnier has been a vocal critic of the mass vaccination campaign. In a letter to the President and Judges of the Supreme Court of the State of Israel, which unrolled the world’s speediest and the most massive vaccination campaign, Montagnier urged for its suspension:
“I would like to summarize the potential dangers of these vaccines in a mass vaccination policy.
1. Short-term side effects: these are not the normal local reactions found for any vaccination, but serious reactions involve the life of the recipient such as anaphylactic shock linked to a component of the vaccine mixture, or severe allergies or an autoimmune reaction up to cell aplasia.
2. Lack of vaccine protection:
2.1 Induction of facilitating antibodies – the induced antibodies do not neutralize a viral infection, but on the contrary facilitate it depending on the recipient. The latter may have already been exposed to the virus asymptomatically. A low level of naturally induced antibodies may compete with the antibodies induced by the vaccine.
2.2 The production of antibodies induced by vaccination in a population highly exposed to the virus will lead to the selection of variants resistant to these antibodies. These variants can be more virulent or more transmissible. This is what we are seeing now. An endless virus-vaccine race that will always turn to the advantage for the virus.
3. Long-term effects: Contrary to the claims of the manufacturers of messenger RNA vaccines, there is a risk of integration of viral RNA into the human genome. Indeed, each of our cells has endogenous retroviruses with the ability to reverse transcriptase from RNA into DNA. Although this is a rare event, its passage through the DNA of germ cells and its transmission to future generations cannot be excluded.
“Faced with an unpredictable future, it is better to abstain.”
Earlier last year, Montagnier presented a powerful case proving that SARS-CoV2 could only be a genetically engineered coronavirus, therefore the vaccine strategy should be based on that fact.
As reported by French Soir, in his television interview of April 17, 2020, Montagnier drew attention to the presence of at least half a dozen mini-sequences of the HIV virus grouped together in a short segment of the SARS-Cov2 genome. This observation was published by the mathematician Jean-Claude Perez in February 2020 under the title “Synthetic origin of Covid-19 and Evolution.” These mini-sequences, researchers believe, could be exogenous information elements (EIA), that is, they can have genetic significance. They assert that this unmistakable presence of concentrated EIAs, in relation to HIV but also with the Yoeli Plasmodium parasite, the agent responsible for malaria, would not be natural and therefore would require an adequate strategy to develop a safe and effective vaccine. Montagnier and Perez explain the scientific challenges and complexity to develop vaccines against HIV and malaria, both of which still have no vaccines to combat infection.
Montagnier argues the coronavirus had escaped in an “industrial accident,” while Chinese scientists at the Wuhan city laboratory were trying to develop a vaccine against HIV.
Back in April 2020, Montagnier urged people to refuse vaccines against COVID-19 when they become available, because “instead of preventing the infection, they [would] accelerate infection.” Today, the newly occurring variants of SARS-CoV-2 that affect vaccinated people prove his thesis. In this case, mass vaccination may cause a new, more deadly wave of pandemic.
The same thesis is shared by the Belgium virologist Vanden Bossche, who is also calling for a halt to the mass-vaccination programs. He believes that if the jabs are not halted, they could lead to the evolution of stronger and stronger variants of the virus until a “supervirus” takes hold and wipes out huge numbers of people.
(Natural News) Thanks to a bombshell new revelation via Project Veritas, we now have smoking gun proof that Fauci lied under oath and funded the gain-of-function research that led to the SARS-CoV-2 bioweapon being developed in Wuhan and unleashed upon the world.
The military documents acquired by Project Veritas confirm what we’ve been reporting for months: That EcoHealth Alliance approached DARPA and requested funding for an experiment involving the aerosolized release of skin penetrating toxic spike protein nanoparticles into wild bat caves in China. DARPA refuse the request, noting that such an experiment would be wildly dangerous and would violate restrictions on biological weapons research.
After DARPA rejected the funding, Fauci and others at the NIH and NIAID found a funding workaround and deliberately circumvented the gain-of-function research restrictions in order to funnel money to Wuhan and affect the open air release of this biological weapon. Since then, millions have died (so far) around the world, and many hundreds of millions will likely die from the vaccine mandates spurred by the covid plandemic.
That’s because the spike protein bioweapon is the key ingredient in covid vaccines, too. For mRNA vaccines, the mRNA instructions tell your body to manufacture spike protein toxic nanoparticles, the very same bioweapons that DARPA said would be too dangerous to release in bat caves.
These documents prove that Fauci is a mass murderer.
As Naomi Wolf recently explained on Steve Bannon’s “War Room” broadcast, these actions on the part of Fauci and his co-conspirators are, in every way, “premeditated manslaughter of millions of people, coordinated at the highest levels.”
Fauci is guilty of mass murder and treason
This is smoking gun proof that Fauci knew he was funding a biological weapon, and he circumvented government restrictions in order to make sure China’s military-run lab got the funding and technical knowledge it needed to build this bioweapon. China then released the bioweapon on the world as an act of war to target the US economy and civil liberties of western nations.
Fauci is not merely a mass murderer, he is guilty of treason against the United States of America.
For protecting Fauci, Big Tech, Big Media, Big Government and Big Pharma are complicit in fraud, murder and treason. They must all be prosecuted for crimes against humanity.
This is why Washington State — and soon, followed by other states — are activating their covid death camps. They will use them to target conservatives to be rounded up under “public health” authority (at gunpoint) and thrown into covid concentration camps which will soon be transformed into active death camps.
Power-hungry, tyrannical Democrats realize the only way they can hold on to power is to start committing genocide against their political opponents. I explain this in the following 18-minute podcast:
My full Situation Update podcast, below, delves into more detail about the covid death camps and why the Biden regime is so rushed to carry out mass genocide (and launch another deadly bioweapon) before the 2022 mid-terms.
There is a high chance that Fauci will oversee the release of a hemorrhagic fever pandemic to spread mass panic and kill even more people
The most likely candidate for what they’ll launch next is a hemorrhagic fever virus such as Marburg or weaponized Ebola. They will try to produce a very high fatality rate to leap to the next level of panic and hysteria, under which they will declare medical martial law and institute domestic travel checkpoints (show me your vaccine papers) and mandatory covid quarantines for the unvaccinated.
It won’t be long before Democrats start cranking up the incineration ovens and just start shoving conservatives, Christians, patriots, gun owners and Trump supporters into those ovens for as long as they are allowed to get away with it.
Naturally, they will have a fight on their hands, because conservative Americans aren’t simply going to walk blindly into death camps and surrender to tyrants. They are going to fight as if their lives depend on it… because they do.
The government has declared war on We the People, and their goal is now mass extermination. We have entered the death camp / incineration oven phase of the government’s betrayal of humanity.
The really crazy part is that once they eliminate as many conservatives as they can, these same government goons will turn their guns on the Democrats because global extermination is the real agenda, regardless of political affiliation.
In other words, all the Democrats going along with this will find themselves exterminated, too, unless armed conservatives manage to stop this holocaust. And yes, it’s Democrats who took most of the vaccines, so about a third of them have already been sentenced to death by lethal injection and will die off over the next decade from vaccine side effects.
If we stop all this today and halt vaccines this very minute, around 1.5 billion human beings will still be killed from the vaccines already administered. For each day that this vaccine holocaust continues, another 10 million are condemned to die.
Get full details in today’s Situation Update podcast:
Wow. A study of 260,000 unvaccinated people – newly published in the New England Journal of Medicine
NATURAL IMMUNITY
Confirming that natural immunity is vastly superior to vax. Natural immunity provided good protection against reinfection and also very robust protection against severe disease or death.
1. Reinfections were rare— only about 0.5%
2. 0ut of the 260,000 there were 1,304 patients with reinfection, only 4 were admitted to the hospital; none needed ICU treatment, and none died.
Senate Committee on State Affairs on Covid-19 Vaccine (Needs to be shared).
Senator Hall had 5 Simple Questions Regarding the Covid-19 mRNA Vaccines
1. Question: With your experience going back to 1999, has there been another vaccine that had the high incidence of hospitalizations and deaths that this vaccine is now showing?
A. Answer: Not to this extent. Not even close.
2. Question: Would any other vaccine had been pulled from the market?
A. Answer: Absolutely. It would have been pulled within the first few, just as we have seen from the past.
3 Question: Have you seen any other vaccine that was put out to the public that skipped the animal tests?
A. Answer: Never before. Especially for children.
4. Question: What I have read is that they actually started the animal studies and discontinued because the animals were all dying they stopped the test?
A. Answer: Right.
He says: “Folks I think it is important to understand that the American people are the Guinea Pigs, this is the test that is going on.” “They didn’t do the human testing and they stopped the animal tests because the animals were dying and then they turned it out to the public.” “Now we are looking at businesses that want to mandate that this experimental vaccine be given to people as a condition of their employment. Yet we have this death count that continues to rise and be completely ignored.”
5. Question: Do you agree with what I am saying?
A. Answer: Absolutely.
UPDATE: Thanks to your efforts with blowing up Mercy Hospital’s phone lines, we have established enough pressure on the would-be murders to stall for time until Monday while attorney’s fight for Scott Quiner’s right to live. His attorneys join us.
Keep up the pressure!
Mercy Hospital
4050 Coon Rapids Blvd
Coon Rapids MN 55433
Main line 763-236-6000
Scott Quiner is in the Heart and Vascular Center
Their number is 763-236-8800
Heather is the Care Coordinator
763-236-8321
Social confinement can lead to feelings of anxiety, stress and depressed mood and this can lead to other negative health consequences. Although people can exercise and seek counseling, nutrients can make a difference with the most important one being magnesium
A substantial percent of the population is likely magnesium deficient and may benefit by taking an additional 150 to 200 mg of magnesium through supplementation
Symptoms of magnesium deficiency can include many mental issues such as depression, confusion and agitation
Magnesium L-threonate has improved effectiveness for increasing cerebrospinal fluid magnesium levels
Only magnesium L-threonate, as opposed to magnesium chloride or magnesium gluconate, increases cerebrospinal fluid magnesium levels and improves cognition in animal models
This article was previously published June 4, 2020, and has been updated with new information.
The recent coronavirus pandemic has infected over 5 million people and has caused over 300,000 deaths. This pandemic has also caused school and business closings, social distancing, and has forced millions of people to be confined to their homes.
Social confinement can lead to feelings of anxiety, stress and depressed mood, and this can lead to other negative health consequences. Although people can exercise and seek counseling, nutrients can make a difference with the most important one being magnesium.
Approximately 50% of American adults are not getting the estimated average requirement for magnesium (around 400 mg of magnesium/day).1 Indeed, most Americans are only consuming around 250 mg of magnesium per day.2
Thus, a substantial percent of the population is likely magnesium deficient and may benefit by taking an additional 150 to 200 mg of magnesium through supplementation.
In fact, up to 30% of the population is magnesium deficient based on low serum magnesium levels, and up to 84% of certain patient populations are magnesium deficient when using the gold standard IV magnesium load test.3
Thus, subclinical magnesium deficiency is common and leads to numerous mental health issues. This brief review will cover the potential benefits of magnesium, particularly magnesium L-threonate, for mood and anxiety.
Magnesium L-Threonate to the Rescue
Symptoms of magnesium deficiency can include many mental issues such as depression, confusion and agitation.4 Individuals with depression are known to have
Lower magnesium levels in the blood5 and the brain.6
Low cerebral spinal fluid magnesium.7
Unfortunately, cerebral spinal fluid magnesium levels are tightly controlled, whereby boosting blood levels of magnesium by 300% only increases cerebrospinal fluid levels by approximately 10 to 19%.8 However:
Magnesium L-threonate has improved effectiveness for increasing cerebrospinal fluid magnesium levels.9
Only magnesium L-threonate, as opposed to magnesium chloride or magnesium gluconate, increases cerebrospinal fluid magnesium levels and improves cognition in animal models.10
The first report of magnesium for improving mood was published in 1921, showing success in 220 out of 250 cases.11 Since then, numerous case reports have found rapid improvements in mood with the use of magnesium supplementation without side effects.12 Additionally:
A randomized equivalent trial found that oral magnesium supplementation was just as effective as an antidepressant for improving mood.13
Thus, clinical studies in humans suggests that magnesium supplementation is beneficial for improving mood. Approximately 60% of individuals who have a depressed mood are considered treatment-resistant and this may be due to magnesium deficiency.14 Moreover:
Low magnesium levels correlate with poor outcomes in individuals with a depressed mood who do not respond to medications.15
Higher magnesium intakes are associated with better mood scores.16
All of this suggests a potential role for magnesium, especially magnesium L-threonate, for mental health.
In summary, depressed mood may simply be a sign of magnesium deficiency in the brain. Boosting brain magnesium levels, particularly with the use of magnesium L-threonate, may have profound benefits on mood.
Importantly, magnesium is needed to make the three primary neurotransmitters in the brain, i.e., serotonin, dopamine and noradrenaline and melatonin, which is important for sleep.
Magnesium L-Threonate for Anxiety Support
High levels of stress can lead to magnesium deficiency by increasing the amount of magnesium that is lost in the urine.17,18
Moreover, magnesium deficiency enhances the stress response.19
Magnesium deficiency increases stress-induced mortality in animals,20 whereas compensation for magnesium deficiency improves the ability of the nervous system to resist stress.21
In other words, stress leads to magnesium deficiency and magnesium deficiency leads to stress.
Animals receiving diets low in magnesium display increased anxiety-related behavior,22 and this may be due to hyper-excitability in the brain and increased cortisol production.23
Importantly, two studies have shown that supplementing animals with magnesium L-threonate reduces anxiety.24,25
Thus, magnesium L-threonate may have a central role in anxiety support. In summary, anxiety can cause magnesium deficiency and vice versa. Considering that most people in the United States are not consuming an adequate amount of magnesium from the diet, supplementation with magnesium L-threonate may have an important role for anxiety support.
While most well-known as a natural sleep regulator, melatonin also has many other important functions. It boosts immune function, helps recharge glutathione and may improve treatment of certain bacterial diseases; it has anticonvulsant and antiexcitotoxic properties, and is a potent antioxidant with the rare ability to enter your mitochondria
In viral infections, melatonin lowers the overreaction of the host cells to the pathogen, thereby raising the host’s tolerance to the virus. This gives the host time to develop the adaptive immune response and eradicate the invading pathogen
Melatonin attenuates several pathological features of COVID-19, including excessive oxidative stress and inflammation, exaggerated immune response resulting in a cytokine storm, acute lung injury and acute respiratory distress syndrome
An October 2021 study found melatonin significantly lowered mortality when given to severely infected COVID patients. In the standard care only group, 13 of the 76 patients died (17.1%), compared to just one of the 82 patients (1.2%) who received melatonin in addition to standard care — a reduction in mortality of 93%
During the second week of infection, a time when severely infected patients can take a drastic turn for the worse, the melatonin group fared much better than the standard care only group, with only two patients developing sepsis, compared to eight in the standard care only group
Melatonin is a hormone synthesized in your pineal gland and several other organs,1 indeed in most cells, including human lung monocytes and macrophages, as it is actually synthesized in your mitochondria.2
While most well-known as a natural sleep regulator, melatonin also has many other important functions.3 Notably, it plays an important role in cancer prevention4 and may prevent or improve certain autoimmune diseases, such as Type 1 diabetes.5
It also has anticonvulsant and antiexcitotoxic properties,6 and is a potent antioxidant7 with the rare ability to enter your mitochondria,8 where it helps prevent mitochondrial impairment, energy failure and the death of mitochondria damaged by oxidation.9 It also:
Boosts immune function
Helps recharge glutathione10 (and glutathione deficiency has been linked to COVID-19 severity)
May improve the treatment of certain bacterial diseases, including tuberculosis11
Helps regulate gene expression via a series of enzymes12
As noted in the Journal of Critical Care:13
“Melatonin is a versatile molecule … Melatonin plays an important physiologic role in sleep and circadian rhythm regulation, immunoregulation, antioxidant and mitochondrial-protective functions, reproductive control, and regulation of mood. Melatonin has also been reported as effective in combating various bacterial and viral infections.”
Melatonin Also Has Important Role in COVID-19 Treatment
Over the past two years, melatonin has emerged as a surprise weapon against COVID-19. It’s been shown to play a role in viral, bacterial and fungal infections14 and as early as June 2020, researchers suggested it might be an important adjunct to COVID-19 treatment.15,16,17 According to the authors of that paper, melatonin attenuates several pathological features of COVID-19, including:18
Excessive oxidative stress and inflammation
Exaggerated immune response resulting in a cytokine storm
Acute lung injury
Acute respiratory distress syndrome
In October 2020, a scientific review,19 “Melatonin Potentials Against Viral Infections Including COVID-19: Current Evidence and New Findings,” summarized the mechanisms by which melatonin can protect against and ameliorate viral infections such as respiratory syncytial virus, viral hepatitis, viral myocarditis, Ebola, West Nile virus and dengue virus.
Based on these collective findings, they hypothesized melatonin may offer similar protection against SARS-CoV-2. One mechanistic basis for this relates to melatonin’s effects on p21-activated kinases (PAKs), a family of serine and threonine kinases. The authors explain:20
“In the last decade, PAKs have acquired great attention in medicine due to their contribution to a diversity of cellular functions. Among them, PAK1 is considered as a pathogenic enzyme and its unusual activation could be responsible for a broad range of pathologic conditions such as aging, inflammation, malaria, cancers immunopathology, viral infections, etc …
Interestingly, melatonin exerts a spectrum of important anti-PAK1 properties … It has been proposed that coronaviruses could trigger CK2/RAS-PAK1-RAF-AP1 signaling pathway viabinding to ACE2 receptor.
Although it is not scientifically confirmed as yet, PAK1-inhibitors could theoretically exert as potential agents for the management of a recent outbreak of COVID-19 infection. Indeed, Russel Reiter, a leading pioneer in melatonin research, has recently emphasized that melatonin may be incorporated into the treatment of COVID-19 as an alternative or adjuvant.”
Melatonin Lowers COVID-19 Mortality
Then, on the last day of 2021, Melatonin Research published a research commentary21 discussing an October 2021 study22 by Hasan et. al., which found melatonin significantly lowered mortality when given to severely infected COVID patients. According to the authors:
“In a single-center, open-label, randomized clinical trial, it was observed that melatonin treatment lowered the mortality rate by 93% in severely-infected COVID-19 patients compared with the control group.
This is seemingly the first report to show such a huge mortality reduction in severe COVID-19 infected individuals with a simple treatment. If this observation is confirmed by more rigorous clinical trials, melatonin could become an important weapon to combat this pandemic.”
The commentators point out that, at less than $5 per course of treatment, melatonin is a cost-effective addition to any treatment plan. For comparison, Regeneron monoclonal antibodies cost about $2,100 per dose and remdesivir is $3,100 per treatment. Melatonin also has no serious side effects, so it can be universally used.
The Hasan trial23 included 158 hospitalized COVID patients between the ages of 18 and 80. All had confirmed severe SARS-CoV-2 infection.
Eighty-two of the patients were enrolled in the melatonin arm and received 10 milligrams (mg) of melatonin half an hour before bedtime for 14 days, in addition to standard therapeutic care, which included oxygen intubation, remdesivir, levofloxacin (an antibiotic for protection against secondary bacterial infections), dexamethasone (an anti-inflammatory) and enoxaparin (an anticoagulant).
In the standard care only group, 13 of the 76 patients died (17.1%), compared to just one of the 82 patients (1.2%) who received melatonin in addition to everything else. That’s a reduction in mortality of 93%, which is quite remarkable. Three mechanisms of action responsible for this success appears to be a combination of its antioxidant, anti-inflammatory and immunoregulatory activities.24
During the second week of infection, a time when severely infected patients can take a drastic turn for the worse, the melatonin group fared much better than the standard care only group, with only two patients developing sepsis, compared to eight in the standard care only group.25
The Hasan trial also supports findings from a clinical case series26 published in 2020, where patients diagnosed with COVID-19 pneumonia received 36 mg to 72 mg of melatonin intravenously per day, in four divided doses, as an adjunct therapy to standard of care.
All of the patients given melatonin improved within four to five days, and all survived. On average, those given melatonin were discharged from the hospital after 7.3 days, compared to 13 days for those who did not get melatonin.
How Melatonin Prevents Sepsis
This isn’t the first time melatonin has been highlighted for its ability to prevent and treat sepsis. A 2010 paper27 in The Journal of Critical Care noted that melatonin helps prevent and reverse septic shock symptoms by:28
Decreasing synthesis of proinflammatory cytokines
Preventing lipopolysaccharide (LPS)-induced oxidative damage, endotoxemia and metabolic alterations
Suppressing gene expression of the bad form of nitric oxide, inducible nitric oxide synthase (iNOS)
Preventing apoptosis (cell death)
Similarly, a 2014 study29 in the Journal of Pineal Research pointed out that melatonin accumulates in mitochondria, and has both antioxidant and anti-inflammatory activity that could be useful in the treatment of sepsis.
This was a Phase 1 dose escalation study in healthy volunteers to evaluate the tolerability and health effects of melatonin at various dosages. They also assessed the effect of melatonin in an ex vivo whole blood model mimicking sepsis.
No adverse effects were reported for dosages ranging from 20 mg to 100 mg, and the blood model testing revealed melatonin and its metabolite 6-hydroxymelatonin “had beneficial effects on sepsis-induced mitochondrial dysfunction, oxidative stress and cytokine responses …” The authors further explained:30
“Mitochondrial dysfunction initiated by oxidative stress drives inflammation and is generally accepted as playing a major role in sepsis-induced organ failure. It has been recognized that exogenous antioxidants may be useful in sepsis, and more recently, the potential for antioxidants acting specifically in mitochondria has been highlighted.
We showed previously that antioxidants targeted to mitochondria, including melatonin, reduced organ damage in a rat model of sepsis … In vitro models of sepsis show that melatonin and its major hydroxylated metabolite, 6-hydroxymelatonin, are both effective at reducing the levels of key inflammatory cytokines, oxidative stress, and mitochondrial dysfunction.
In rat models of sepsis, melatonin reduces oxidative damage and organ dysfunction and also decreases mortality.
The dose needed for antioxidant action is thought to be considerably higher than that given for modulation of the sleep–wake cycle, but the actual dose required in man is unclear, particularly because the major bioactive effects of oral melatonin in the context of inflammation are likely to be mediated primarily by metabolite levels.”
Melatonin Has Many Mechanisms of Action
When it comes to viral infections, melatonin doesn’t actually target the virus itself. It primarily aids the host, lowering the overreaction of the host cells to the pathogen, thereby raising the host’s tolerance to the virus. As explained in the featured Melatonin Research commentary,31 “This tolerance allows the host sufficient time to develop the adaptive immune response and finally eradicate the invading pathogens.”
By regulating your immune responses, melatonin also helps prevent cytokine storms,32 which is what ultimately kills some patients with serious SARS-CoV-2 infection. Melatonin is also a known cytoprotector with neuroprotective properties that can potentially reduce the neurological sequelae documented in patients infected with COVID-19.33
Part of melatonin’s benefit against COVID may also have to do with the fact that it enhances vitamin D signaling34 and, together, melatonin and vitamin D synergistically enhance your mitochondrial function. In fact, your mitochondria are the final common targets for both.35
I’ve written many articles detailing the importance of vitamin D optimization to prevent SARS-CoV-2 infection and more serious COVID-19 illness. The evidence for this is frankly overwhelming, and raising vitamin D levels among the general population may be one of the most important prevention strategies available to us. To learn more, download my vitamin D report, available for free on stopcovidcold.com. Melatonin may also combat SARS-CoV-2 infection by:36
Having an antibacterial effect on white blood cells called neutrophils37 (a high neutrophil count is an indicator for infection)
Suppressing oxidative stress38
Regulating blood pressure (a risk factor for severe COVID-19)
Improving metabolic defects associated with diabetes and insulin resistance (risk factors for severe COVID-19) via inhibition of the renin-angiotensin system (RAS)
Protecting mesenchymal stem cells (MSCs, which have been shown to ameliorate severe SARS-CoV-2 infection) against injuries and improving their biological activities
Promoting both cell-mediated and humoral immunity
Promoting synthesis of progenitor cells for macrophages and granulocytes, natural killer (NK) cells and T-helper cells, specifically CD4+ cells
Inhibiting NLRP3 inflammasomes39 — Inflammasomes are part of your natural immune response. When a pathogen is detected, inflammasomes are activated and start releasing proinflammatory cytokines. The inflammasome NLRP3, specifically, has been identified as a key culprit in acute respiratory distress syndrome (ARDS) and acute lung injury, both of which are potential outcomes of COVID-19 infection40
Melatonin Reduces Risk of Positive COVID-19 Test
Data41,42 from Cleveland Clinic also supports the use of melatonin. Here, the researchers analyzed patient data from the Cleveland Clinic’s COVID-19 registry using an artificial intelligence platform designed to identify drugs that may be repurposed.43,44
By identifying clinical manifestations and pathologies shared by COVID-19 and 64 other diseases, they were able to conclude that certain proteins associated with chronic diseases are highly connected with SARS-CoV-2 proteins. Put another way, a number of proteins appear to play a key role in the pathologies seen both in COVID-19 and other chronic diseases.
These connections suggest that drugs already in use for a chronic disease may be repurposed and used in the treatment of COVID-19, as it acts on one or more shared biological targets. Melatonin stood out in this regard. Patients who used melatonin as a supplement had, on average, a 28% lower risk of testing positive for SARS-CoV-2. Blacks who used melatonin were 52% less likely to test positive for the virus.
Unfortunately, two key data points missing from the analysis are the dosage used and the length of supplementation. These data were not included in the patient registry, so we don’t know how much melatonin is required, or how long you need to take it, to lower your risk of SARS-CoV-2 infection to the degree found in this study.
Melatonin Is an Integral Part of Front Line Protocol
Early in 2020, the Front Line COVID-19 Critical Care Alliance (FLCCC)45 developed preventive, outpatient treatment and inpatient protocols46 based on the insights of the founding critical care doctors. Dr. Paul Marik,47 a critical care doctor known for his life-saving vitamin C sepsis protocol,48 is one of those doctors.
Marik published a paper in the Journal of Thoracic Disease in February 202049 giving the scientific rationale for using melatonin to help regulate the oxidative imbalance and mitochondrial dysfunction that are commonly found in sepsis.
This was followed by a paper published in the Frontiers in Medicine in May 2020,50 in which he and a team of scientists presented a therapeutic algorithm for melatonin in the treatment of COVID-19 specifically. “Melatonin’s multiple actions as an anti-inflammatory, antioxidant and antiviral (against other viruses) make it a reasonable choice for use,” they wrote.
Based on its known mechanisms of action, the FLCCC has included melatonin in its early treatment and hospital treatment protocols from the start. You can download the latest protocols on the FLCCC’s website.51
As a supportive therapy, the FLCCC recommends taking 6 mg before bed if you’re treating early or mild symptomatic COVID-19. The hospital treatment protocol calls for anywhere from 6 mg to 12 mg of melatonin at night, until discharge.
For patients treating long-haul COVID-19 syndrome (LHCS), they recommend taking between 2 mg and 12 mg nightly. Begin with a low dose and work your way up as tolerated. If your sleep is disturbed, lower your dose. (Low doses of melatonin will help make you sleepy, while higher doses can trigger sleeplessness.)
General Guidance for Supplementation
While the doses suggested when used against COVID are significantly higher than what you’d normally take to improve your sleep, there does not appear to be any danger to these doses. Research has found no adverse effects for dosages ranging from 20 mg up to 100 mg.52
These dose ranges are up to 100 times more than what a typical conservative dose of 0.5 mg, but it is encouraging that no adverse effects were observed at these high doses. It would still be prudent however to only use doses this high for limited times when you might need them.
Whatever dose you take — and I recommend starting low, at 1 mg or less — be sure to take melatonin at night, before bed. Rising melatonin levels is the reason you feel sleepy in the evening, so it’s ill advised to take it in the morning or during the day, when your natural level is (and should be) low.
Melatonin is also best taken sublingually, either in the form of a spray or sublingual tablet. Sublingually, it can enter your blood stream directly and doesn’t have to go through the digestive tract. As a result, its effect will be felt more rapidly.
Updated: January 2021
Based on the available scientific evidence and current clinical experience, the SPR Collaboration recommends that physicians and authorities consider the following covid-19 treatment protocol for the prophylactic and early treatment of people at high risk or high exposure.
Numerous international studies have shown that prophylactic and early treatment can significantly reduce the risk of severe and fatal covid-19 (see scientific references below).
Note: Patients are asked to consult a doctor.
Treatment protocol
Prophylaxis
Goal: Supporting immune system, reducing viral load if infected.
The early treatment of patients as soon as the first typical symptoms appear and even without a PCR test is essential to prevent progression of the disease. In contrast, isolating infected high-risk patients at home and without early treatment until they develop serious respiratory problems, as often happened during lockdowns, may be counterproductive.
People at high risk living in an epidemically active area should consider prophylactic treatment together with their doctor. The reason for this is the long incubation period of covid (up to 10 days): when patients first notice that they contracted the disease, the viral load is already at a maximum and there are often only a few days left to react with an early treatment intervention.
Early treatment based on the above protocol is intended to avoid hospitalization. If hospitalization nevertheless becomes necessary, it is recommended to avoid invasive ventilation (intubation) whenever possible and to use oxygen therapy (HFNC) instead.
Treatment studies
Results of trials and studies on the early treatment of covid.
Ivermectin
Ivermectin (an antiparasitic drug) has anti-viral and anti-inflammatory properties.
Several controlled and observational studies on ivermectin found anti-viral and anti-inflammatory effects and a significant reduction in covid morbidity and mortality.
Once low-quality studies are excluded from the analysis, the benefit of ivermectin is no longer statistically significant, although a moderate benefit might still be possible.
Zinc inhibits RNA polymerase activity of coronaviruses and thus inhibits virus replication. Quercetin (a plant polyphenol) supports the cellular absorption of zinc and has additional anti-viral properties.
A Spanish study found that low plasma zinc levels (below 50mcg/dl) increased the risk of in-hospital death of covid patients by 130%.
US studies found an 84% decrease in hospitalizations and a 45% decrease in mortality based on risk-stratified early treatment with zinc and HCQ.
A US case study reported a rapid resolution of covid symptoms, such as shortness of breath, based on early outpatient treatment with high-dose zinc.
An Italian randomized trial found a significantly reduced hospitalization rate and mortality in covid patients receiving quercetin.
Bromhexine
Bromhexine (a mucolytic cough medication) inhibits the expression of cellular TMPRSS2 protease and thus the entry of the virus into the cell, as first described in 2017.
A randomized Iranian trial with 78 patients found a decrease in intensive care treatments of 82%, a decrease in intubations of 89%, and a decrease in deaths of 100%.
A Chinese trial found a 50% reduction in intubations in patients receiving bromhexine.
A Russian study found a faster recovery in hospitalized patients receiving bromhexine.
A Russian prophylaxis study found a reduction in symptomatic covid from 20% to 0%.
Vitamin D3
Vitamin D3 supports and improves the immune system response to infections.
A Spanish randomized controlled trial found a 96% reduction in the risk of requiring intensive care in patients receiving high-dose vitamin D (100,000 IU).
Another Spanish study with 930 hospitalized patients found a 87% reduction in ICU treatment and a 79% reduction in mortality in patients receiving high-dose vitamin D.
A study in a French nursing home found an 89% decrease in mortality in residents who had received high-dose vitamin D either shortly before or during covid-19 disease.
A retrospective British study of approximately 1000 hospitalized covid patients found an 80% reduction in mortality with high-dose vitamin D.
A large Israeli study found a strong link between vitamin D deficiency and covid-19 severity.
For an overview of all covid-19 vitamin D studies, see here.
A meta-study including 15,000 patients found a reduction in covid mortality of 53% in patients who were receiving aspirin as early or prophylactic treatment.
A study published in PLOS One found a reduction in covid mortality at 30 days from 10.5% (control group) to 4.3% (with aspirin) in 70,000 US veterans taking aspirin.
A retrospective US study with 400 patients found a reduction in ICU treatments by 43% and a reduction in mortality by 47% in the group of patients treated early with aspirin.
A Mexican randomized controlled trial found a 40% reduction in hospitalization in patients receiving sulodexide (a heparin combination).
Arginine
Arginine is an amino acid supporting endothelial function, immune regulation, and tissue repair.
A small randomized controlled trial, published in The Lancet E-Clinical Medicine, found that hospitalized covid patients receiving 3g of arginine per day had a significantly reduced need of respiratory support at 10 days and a significantly shorter length of hospitalization.
A metabolomic analysis in covid ICU patients, published in Critical Care Explorations, found that low levels of arginine very strongly predicted the risk of death.
A report published in PNAS found that plasma arginine and arginine bioavailability were significantly lower in adult and pediatric covid patients compared to controls.
An in vitro study by the German Max Planck Institute, published in Nature Scientific Reports, found artemisia annua to be effective against SARS-CoV-2at realistic doses.
An in vitro study by US researchers, published in the Journal of Ethnopharmacology, found artemisia annua hot-water extracts to be effective against SARS-CoV-2 replication.
In a small clinical trial, published in Antimicrobial Agents, the viral load decreased significantly faster in covid patients treated with artemisinin-piperaquine.
In a 2005 in vitro study, published in Antiviral Research, artemisia annua was already identified as effective against the original SARS-1 virus.
In Madagascar, the first country to apply artemisia annua extract against covid, covid mortality and excess mortality have remained very low, even for African standards.
In a simulation study by a Harvard research group, the anti-malaria drug amodiaquine was identified as most effective against SARS-CoV-2 replication.
Mouthwashes and nasal sprays
Mouthwashes and nasal sprays target the initial infection and viral replication.
Several small studies found that mouthwashes (gargling) based on povidone-iodine and nasal sprays based on povidone-iodine or nitric oxide may prevent a coronavirus infection or reduce its duration or symptoms (more about this).
The German Society for Hospital Hygiene (DGKH) recommends anti-viral mouthwashes and nasal sprays for prophylaxis and early treatment.
Some observers argued that traditional nasal rinsing and gargling practicesin South East Asia may have helped successfully limiting coronavirus infections in these countries.
Israel started mass production of nasal sprays based on nitric oxide in early 2021.
Anti-androgen treatment
Anti-androgen treatment inhibits the expression of the TMPRSS2 cellular protease used by SARS-CoV-2, which is driven by androgen hormones (i.e. male sexual hormones).
A first randomized, double-blinded and placebo-controlled trial in Brazil found that proxalutamide reduced hospitalization rates in male patients by 91%.
Another randomized, double-blinded and placebo-controlled trial in Brazil found that proxalutamide reduced mortality in hospitalized patients (male and female) by 78%.
Previous studies found that men receiving anti-androgens – typically used against prostate cancer or hair loss – were at a much lower risk of severe covid.
Fluvoxamine and Cyproheptadine
These drugs inhibit serotonin-induced pulmonary vasoconstriction.
The TOGETHER trial found that fluvoxamine outpatient treatment of covid patients reduced disease progression (hospitalizations or ER visits) significantly by 32%.
The results of two preliminary US trials indicate that early treatment with fluvoxamine may strongly reduce the risk of severe covid, hospitalization and death.
In a small US case study, cyproheptadine rapidly improved the condition of hospitalized covid patients
Fluvoxamine and cyproheptadine target serotonin metabolism and serotonin-induced pulmonary vasoconstriction, which according to emerging evidence may be a key mechanism driving severe covid and covid-related respiratory failure.
Fluvoxamine is a selective serotonin reuptake inhibitor (SSRI) and reducesplatelet serotonin concentration; cyproheptadine is a direct serotonin receptor antagonist. In addition, fluvoxamine is a sigma-1 receptor antagonist and has an anti-inflammatory effect.
A study by the University of Oxford, published in the Lancet, found a significant reduction in urgent care visits and hospitalizations in patients receiving budesonide (an asthma drug).
The British PRINCIPLE trial found that budesonide accelerated recovery by 3 days and reduced hospitalizations and deaths from 10.3% to 8.5%.
The early outpatient treatment protocol developed by McCullough et al. recommends the use of prednisone if (and only if) covid-related respiratory symptoms develop.
Amantadine
Amantadine is a medication used against influenza and some neurological conditions.
A Danish study, published in December 2021 in Nature communications biology, showed that amantadine inhibits two of the four ion channels of SARS-CoV-2.
A study by the German Robert Koch Institute (RKI), published in March 2021 in Viruses, showed that amantadine inhibits SARS-CoV-2 replication in cell culture. However, according to the RKI the required dose can only be achieved via inhalation.
A small Polish observational study, published in December 2021 by Medpress, found that covid patients receiving amantadine had a low hospitalization rate.
A small Polish study, published in July 2020, found that patients receiving amantadine against neurological conditions had mostly asymptomatic covid.
Monoclonal antibodies, Molnupiravir, Paxlovid
These novel drugs have direct anti-viral properties.
Monoclonal antibodies have been shown to be effective in early treatment but ineffective in the treatment of already hospitalized patients (post-viral phase). In addition, monoclonal antibodies rapidly lose efficacy against new viral variants.
Plasma from convalescents has been shown to be ineffective in both early and late treatment of covid patients.
Paxlovid (Pfizer) directly inhibits viral replication and, according to initial data, has been shown to be very effective in early treatment (reducing hospitalizations and deaths in at-risk groups by nearly 90%). Paxlovid, however, will not be available until mid-2022.
In a tell-all video, Project Veritas shows evidence that the U.S. government, with Dr. Anthony Fauci, the NIAID, the NIH and EcoHealth Alliance, secretly discussed avenues on how to conduct dangerous gain-of-function research.
According to a Veritas summary, ”Dr. Fauci has repeatedly maintained, under oath, that the NIH and NAIAD have not been involved in gain-of-function research with the EcoHealth Alliance program. But according to the documents obtained by Project Veritas which outline why EcoHealth Alliance’s proposal was rejected, DARPA certainly classified the research as gain of function.”
The documents also show “the concealment of documents, the suppression of potential curatives, like ivermectin and hydroxychloroquine, and the mRNA vaccines,” the summary says.
The COVID-19 vaccine rollout was supposed to signal the beginning of the end of the pandemic but, instead, a massive study indicates a sharp increase in COVID cases and deaths erupted in the wake of the jabs.
In the U.S. alone, cases jumped by 38% and deaths by 31%. In total, researchers found that 89.4% of 145 countries experienced this surprising, negative effect.
Remdesivir: An Epidemic Failure – Swiss Policy Research
SPR and ther independent experts warned early on that the very expensive “anti-viral” drug remdesivir, produced by Gilead and promoted by the media, is a failure. Dr. Paul Marik, author of the EVMS Covid-19 Critical Care Protocol, called remdesivir a “particularly useless drug” and Gilead’s aggressive marketing campaign “Wall Street centered, not patient-centered”.
The newly published results of the global WHO Solidarity trial now confirm that remdesivir reduces neither hospital stay (time to recovery) nor mortality. But remdesivir is not just a “useless drug”, it may in fact be a dangerous one, as its liver and kidney toxicity in covid patients has been widely documented and is currently being investigated by the European Medicines Agency (EMA).
Investigative journalist Dilyana Gaytandzhieva recently revealed how Gilead paid more than $200 million to US doctors and hospitals to promote its drugs despite several hundred drug-related deaths (this is referring to Gilead’s hepatitis C drug, in particular).
Moreover, several of the fraudulent anti-HCQ studies were published by researchers linked to or paid by remdesivir producer Gilead. The WHO trial itself used toxic overdoses of HCQ, as first revealed by US doctor and biohazard expert Meryl Nass in June (the WHO trial was halted thereafter).
(Update: As the Guardian reports, Gilead knew about the negative WHO trial results since September 23, but nevertheless signed a $1 billion deal for 500,000 doses of remdesivir with the European Commission, which did not yet know about the results, on October 8.)
Based on current scientific and clinical evidence, it is best to treat high-risk covid patients as early as possible to avoid disease progression and hospitalization. For more information, see the recent video presentation on ambulatory treatment of covid by Dr. Peter McCullough.
OneAmerica, a national life insurance company based in Indianapolis, reports working age people (18 to 64) are dying at a rate that is 40% higher than prepandemic rates
There’s also been an uptick in disability claims. Initially, there was a rise in short-term disability claims, but now most claims are for long-term disabilities
Hospitalizations in Indiana are also higher than before the COVID shots were rolled out in in 2021, and the highest they’ve been in five years
The Insurance Regulatory and Development Authority of India also reports a 41% rise in death claims in 2021
COVID-19 deaths were significantly lower in 2021 than 2020, so COVID-19 can be ruled out as the cause for this historical rise in excess deaths and disabilities. Right now, the most probable cause is the experimental COVID jabs
As we’ve seen over the past two years, data and statistics can be manipulated and skewed in a wide variety of ways. COVID cases, for example, have clearly been overinflated by including people with no symptoms (likely false positives) and diagnosing anyone entering the hospital for an unrelated issue as a COVID patient if they test positive (again, falsely) for SARS-CoV-2.
One of the most reliable data points we have is all-cause mortality. It’s very hard to massage that statistic, as people are either dead or they’re not. Their inclusion in the national death index database is based on one primary criteria — they’ve died — regardless of the cause.
From there, their cause of death, as identified on their death certificate, is added in to more granular statistics, such as the number of people who died from cancer and heart disease in any given year, for example. But while the cause of any given death can be manipulated and altered, the fact that there was a death is more certain. What’s more, death rates tend to be very stable.
As noted in a (not peer-reviewed) study led by scientist Denis Rancourt, who looked at U.S. mortality between March 2020 and October 2021,1 “All-cause mortality by time is the most reliable data for detecting true catastrophic events causing death, and for gauging the population-level impact of any surge in deaths from any cause.”
40% Rise in Deaths Among Working Americans
With that in mind, OneAmerica’s announcement that the death rate of working-age Americans (18 to 64), in the third quarter of 2021, was 40% higher than prepandemic levels is rather stunning. OneAmerica is a national mutual life insurance company based in Indianapolis. During an early January 2022 press conference, CEO Scott Davidson said:2
“We are seeing, right now, the highest death rates we have seen in the history of this business — not just at OneAmerica. The data is consistent across every player in that business.
And what we saw just in third quarter, we’re seeing it continue into fourth quarter, is that death rates are up 40% over what they were pre-pandemic. Just to give you an idea of how bad that is, a three-sigma or a one-in-200-year catastrophe would be 10% increase over pre-pandemic. So, 40% is just unheard of.”
According to Davidson, a majority of the death claims filed are not classified as COVID-19 deaths, so something else is driving up the death rate. As reported by The Center Square:3
“The CDC weekly death counts, which reflect the information on death certificates and so have a lag of up to eight weeks or longer, show that for the week ending Nov. 6, there were far fewer deaths from COVID-19 in Indiana compared to a year ago — 195 verses 336 — but more deaths from other causes — 1,350 versus 1,319.”
Disability Claims Have Also Risen
At the same time, OneAmerica has also noticed an uptick in disability claims. Initially, there was a rise in short-term disability claims, but now most claims are for long-term disabilities. The company expects the rise in claims will cost them “well over $100 million,” an unexpected expense that will be passed on to employers buying group life insurance policies.
During that press conference, Brian Tabor, president of the Indiana Hospital Association, confirmed Indiana hospitals are seeing a dramatic increase in both deaths and hospitalizations for a wide variety of conditions.4
Not only are the number of hospitalizations in Indiana higher than it was before the COVID shots were rolled out in in 2021, it’s the highest it’s been in five years.5 Meanwhile, the daily deaths from COVID-19 are less than half that of 2020.
What’s Killing Younger Healthy Americans?
Since COVID-19 isn’t killing younger, healthy Americans, what is? What changed in 2021 that might have such a devastating effect on people’s health? Well, the most obvious change is that more than 100 million Americans got the experimental COVID shots, and doctors and scientists have elucidated several mechanisms by which these gene transfer technologies might injure or kill. As reported by vaccine safety blogger Steve Kirsch:6
“Normally death rates don’t change at all. They are very stable. It would take something REALLY BIG to have an effect this big. The effect size is 12-sigma.7 That is an event that would happen by pure chance every 2.832 years. That’s very rare. It’s basically never.
The universe is only 14 billion years old which is 1.413. In other words, the event that happened is not a statistical ‘fluke.’ Something caused a very big change … Whatever it is that is causing this, it is bigger and deadlier than COVID and it’s affecting nearly everyone.”
Kirsch lists 14 clues as to what this deadly “something” might be, including the following:8
The rise in deaths began after the rollout of the COVID shots
It’s primarily working age people (18 to 64) who are dying
There are more excess deaths than any time in history, which suggests they’re caused by a novel threat
COVID deaths have significantly diminished, so COVID-19 can be ruled out
People are dying from a wide variety of causes, so most pathogens can be ruled out
To get an effect size this high, the lethal agent must affect massive numbers of people. “It is something new affecting at least half the population,” Kirsch writes, “like a new mandated vaccine for example”
Indiana Gov. Eric Holcomb has been, and continues to, push to get everyone injected
Since other life insurance companies are seeing the same trend, the causative factor is national in scope
The dramatic rise in disabilities suggests that many who aren’t killed by this novel threat are seriously injured, often long-term. As mentioned, doctors and scientists have detailed several mechanisms of action by which the COVID shots can maim or kill
Adverse Events May Be More Underreported Than Calculated
Kirsch continues:9
“We know that about 3M people die a year in the U.S.10 75% are over 65 years old, so that leaves us with 750K deaths per year for under 65. If that jumped by 40% from pre-pandemic levels in Q3 and Q4, we should assume that Q2 was the ramp up period (we’ll assume a linear ramp up in Q2).
So that is 75K deaths per quarter for Q3 and Q4 and half of that, 37K deaths in Q2. So that means roughly 187K excess deaths are probably happening for ages 18-64 due to some new cause.”
He then goes on to compare that rough estimate of 187,000 excess deaths to the U.S. Vaccine Adverse Events Reporting System (VAERS) which, as of the December 24, 2021, data release, included 2,156 deaths between the ages of 17 and 65.
Subtracting the background death rate of 40 from 2,156, multiplied by Kirsch’s calculated underreporting factor (URF) of 4111 gives us 87,000 deaths. In other words, assuming vaccine injuries are underreported by a factor of 41, the real death toll from the COVID jab would be 87,000. However, that’s 100,000 short of the 187,000 excess death rate calculated above.
This means “either there is another effect at play which is actually killing more people 18 to 64 than the vaccine is, (unlikely but possible),” Kirsch writes, or “my URF of 41 is underestimating deaths by a factor of 2.15.” Kirsch is not alone in suspecting the novel COVID shots are the causative factor for this dramatic rise in excess deaths.
A Government Imposed Health Disaster Looms Large
Dr. Robert Malone addressed OneAmerica’s finding in a Substack article, stating:12
“AT A MINIMUM, based on my reading, one has to conclude that if this report holds and is confirmed by others in the dry world of life insurance actuaries, we have both a huge human tragedy and a profound public policy failure of the U.S. Government and U.S. HHS system to serve and protect the citizens that pay for this ‘service.’
IF this holds true, then the genetic vaccines so aggressively promoted have failed, and the clear federal campaign to prevent early treatment with lifesaving drugs has contributed to a massive, avoidable loss of life.
AT WORST, this report implies that the federal workplace vaccine mandates have driven what appears to be a true crime against humanity. Massive loss of life in (presumably) workers that have been forced to accept a toxic vaccine at higher frequency relative to the general population of Indiana.”
Jessica Rose, Ph.D., a research fellow at the Institute for Pure and Applied Knowledge in Israel, also weighed in on the new data:13
“So what does this tell us? It tells us that we are potentially in a huge steaming pile of shit. To be frank. These indications from our friend at the insurance company are simply that — indications.
If what we are seeing in VAERS, and the other adverse event reporting systems, is the mere reflection of what is actually going on with regards to injuries, which I presume it is, then we ain’t seen nothing yet.
And if what is being reported with regards to immune deficiencies associated with these injections is not simply anecdotal or representative of a small sub-cohort of individuals, we could be looking at a government-imposed complete health disaster.”
The Defender also reported other studies and data suggesting the COVID shots are causing massive harm:14
“In a September study15 described as ‘narrative-shattering,’ Harvard, Tufts and Veterans Affairs researchers reported that approximately half of hospitalized patients ‘showing up on COVID-data dashboards in 2021’ had likely been admitted ‘for another reason entirely.’
In Ventura County, California, which is witnessing a startling spike in non-COVID-related hospitalizations,16 nurse whistleblowers argue the vaccines should be one of the first explanations considered. Why else, they ask, would otherwise healthy adults be showing up in droves with brain bleeds, heart attacks, autoimmune issues and lung abnormalities?
Autopsies17 of individuals who died following COVID vaccination reveal shocking pathological alterations most frequently affecting the heart and lungs but also the brain and other organs …
Far from being willing to contemplate the elephant in the room, the Indiana insurance executive indicated he plans to require all OneAmerica employees to get vaccinated. Somewhat counterintuitively, the industry’s ability to pass along costs for elevated claims activity by raising premiums now has analysts rosily predicting the insurance industry is ‘buckled up to accelerate growth in 2022’ …
On the consumer side of the fence, the picture is far less rosy — for both the unvaccinated and vaccinated. For example, New York State Assemblyman Patrick Burke (D-Buffalo) proposed punitive legislation that would permit insurers to deny COVID-related treatment coverage for individuals who choose not to get vaccinated.
Adding insult to injury, there are also reports of insurance companies imposing premium increases on employers in counties with low vaccination rates. Meanwhile, many of those injured by COVID vaccines report18 denials of health and disability insurance coverage.”
Same Trend Seen in Many Other States and Countries
As noted by Davidson, OneAmerica is not alone in seeing an unprecedented spike in excess deaths. It’s also not limited to the United States. The Insurance Regulatory and Development Authority of India, for example, also reports a 41% rise in death claims in 2021.19 That’s near-identical to the 40% increase reported by OneAmerica.
According to Kirsch, Phoenix, Arizona, is reporting a 100% rise in the death rate among city employees. In 2021, it was double that of the 10-year average.20 “There is clearly something going on that is not unique to Indiana,” he writes, adding:
“Excess mortality figures in Europe21 and the UK seem to show younger people are dying faster than the elderly, and that people 0-14 are dying faster in the second half of 2021 as compared to the first. More evidence showing that the vaccines are killing kids.”
You may recall that at the end of October 2021, the U.S. Centers for Disease Control and Prevention published a ridiculous “study”22 that would have even failed a seventh-grade science experiment that claimed to show the COVID shot reduced the risk of death from all causes, including accidents, by 34%.
The CDC can lie up and down all day long and attempt to confuse people with fraudulent studies, but what they are simply unable to do at this point is to manipulate the death rates. Independent third-party insurance carriers are now validating the depth of the CDC cover-up and fraud. The real-world excess deaths we’re now seeing clearly refute the CDC’s attempt to prop up the COVID jab narrative with manipulated data.
Safety Signal Is Indisputable
As cardiologist Dr. Peter McCullough has repeatedly stated, we had a clear safety signal all the way back in February 2021, and it’s only gotten more pronounced over time. Despite that, not a single safety review has been conducted, and our health authorities refuse to address the astronomical death toll.
At this point, anyone who says the COVID shots are “safe and effective,” full stop, immediately loses all credibility. There’s not a shred of data to suggest either is true. Everything we have points to these injections being the most lethal drugs ever used in modern medical history.
Perhaps the saddest part of it all is that they’re completely unnecessary. Doctors have identified several effective treatment options that can slash the COVID death rate by 85% or more. There’s no medical reason to include the global population in a novel drug experiment. We could have avoided all these excess deaths by making sure early treatment was given, rather than exclusively relying on an experimental “vaccine.”
Early Treatment Options
While the overall risk of COVID-19 has been grossly exaggerated, early treatment is key, both for preventing severe infection and preventing “long-haul COVID.” Here are a few suggestions:
• Oral-nasal decontamination — The virus, especially the Delta variant, replicates rapidly in the nasal cavity and mouth for three to five days before spreading to the rest of the body, so you want to strike where it’s most likely to be found right from the start.
Research23 has demonstrated that irrigating your nasal passages with 2.5 milliliters of 10% povidone-iodine (an antimicrobial) and standard saline, twice a day, is an effective remedy.
Another option that was slightly less effective was using a mixture of saline with half a teaspoon of sodium bicarbonate (an alkalizer). You can also gargle with these to kill viruses in your mouth and throat. When done routinely, it can be a very effective preventive strategy. You can find printable treatment guides on TruthForHealth.org.
• Nebulized peroxide — A similar strategy is to use nebulized hydrogen peroxide, diluted with saline to a 0.1% solution. Both hydrogen peroxide and saline24,25 have antiviral effects. You can view my previous videos on this on BitChute.
In a May 10, 2021, Orthomolecular Medicine press release,26 Dr. Thomas E. Levy — board-certified in internal medicine and cardiology — discussed the use of this treatment for COVID-19 specifically. Levy has in fact written an entire book on peroxide nebulization called “Rapid Virus Recovery,” which you can download for free from MedFox Publishing.
• Vitamin D optimization — Research has shown having a vitamin D level above 50 ng/mL brings the risk of COVID mortality down to near-zero.27
• Other key nutraceuticals — Vitamin C, zinc, quercetin and NAC all have scientific backing.
• Key drugs — For acute infection, ivermectin, hydroxychloroquine or monoclonal antibodies can be used. While monoclonal antibodies and hydroxychloroquine must be used early on in the disease process, ivermectin has been shown to be effective in all stages of the infection.
Doxycycline or azithromycin are typically added as well, to address any secondary bacterial infection, as well as inhaled budesonide (a steroid). Oral steroids are used on and after the fifth day for pulmonary weakness and aspirin or NAC can be added to reduce the risk of clotting.
Full-strength aspirin is also typically recommended, but I believe lumbrokinase and serrapeptase may be a better, at least safer, alternative, as they help break down and prevent blood clots naturally.
Life expectancy for the U.S. fell in 2020 from 78.8 in 2019 to “just” 77 in 2020, and major media are having a field day talking about the precipitous “cliff” of death that the pandemic has created.
It’s a drop of 2.3%. But is it really as bad as it sounds? Ryan McMaken of the Mises Institute explains it in terms of relativity, i.e., what the drop means relative to what the life expectancy has been in the past 20 years.
And his conclusion is that, first, “life expectancy in the U.S. had already all but screeched to a halt in the decade leading up to 2020,” and second, that when taken in context and “even considering recent data on life expectancy and mortality, it remains extremely unclear why 2020’s changes in these metrics would justify the extreme panic and human rights violations that resulted from stay-at-home edicts and coerced medication.”
One reason the CDC has changed its rules to not require retesting for COVID-19 infection after quarantine is that the PCR tests used to determine infectivity can stay positive for up to 12 weeks.
The rapid antigen tests also may be less sensitive to the Omicron variant, according to CDC director Dr. Rochelle Walensky, but even so, if you test negative on the rapid test and you have symptoms, you need to get the PCR test anyway.
Then, if you have symptoms and test positive on the PCR test, you just don’t have to retest after you’ve quarantined, as the long positivity rates for the PCR tests “would have people in isolation for a very long time if we were relying on PCRs,” she told ABC News.
Death rates among working-age adults in the U.S. went up a “stunning” 40% compared to prepandemic levels.
Scott Davison, CEO of life insurance company OneAmerica, told The Center Square, “We are seeing, right now, the highest death rates we have seen in the history of this business — not just at OneAmerica. The data is consistent across every player in that business.”
He added that “40% is just unheard of.” Curiously, the death certificates aren’t reflecting COVID as a cause of death, he said. Also interesting is there is an uptick in disability claims.
Pregnant and postpartum women are dying in record numbers from chronic high blood pressure, MedicineNet reports.
Specifically, blood pressure-related causes of death multiplied by a factor of 15 over a 39-year period. Black women were affected three to four times as much, the study found.
While deaths due to preeclampsia actually fell during that same time period, study authors explained that deaths due to chronic high blood pressure increased, with one-third occurring before delivery, a third the day of delivery or the week following and one-third occurring one week to a year after.
December 30, 2021, Joe Rogan interviewed Dr. Robert Malone, the inventor of the mRNA gene transfer technology. YouTube and Twitter promptly deleted the interview
Google has also been caught red-handed manipulating search results such that Malone’s Rogan interview won’t show up when searching for “mass formation psychosis”
Malone was permanently banned from Twitter December 29, 2021, likely triggered by a post that included a video by the Canadian COVID Care Alliance, which reviewed Pfizer data showing the COVID jab causes more illness than it prevents, and that the Pfizer trial was flawed both in design and construction
Alternatively, Malone may have been banned due to a post showing how the World Economic Forum controls the global media narrative
A Physicians Declaration by the International Alliance of Physicians and Medical Scientists, signed by more than 16,000 doctors and scientists, states that “healthy children shall not be subjected to forced vaccination” as their clinical risk from SARS-CoV-2 infection is negligible and long term safety of the shots cannot be determined prior to such policies being enacted
December 30, 2021, Joe Rogan interviewed Dr. Robert Malone, the inventor of the mRNA gene transfer technology. YouTube and Twitter promptly deleted the interview and mainstream media published a rash of articles attacking Malone and Rogan in the most disparaging terms possible.1
In addition to censoring Malone, Google has also been caught red-handed manipulating search results such that Malone’s Rogan interview won’t show up when searching for “mass formation psychosis.”2 That search term also won’t give you any of the interviews given by psychologist Mattias Desmet, who was the first to use that term as a diagnosis for why so many are buying an obviously flawed, if not ridiculous, COVID narrative.
In response to the obvious Big Tech censorship, Congressman Troy Nehls, R-Texas, entered the transcript of the podcast (the Joe Rogan Experience #17573) into the Congressional Record with the following statement:4
“By deplatforming Dr. Robert Malone for voicing opposition and removing the interview, Twitter and YouTube are once again proving that they don’t work for their users but for big Pharma, big media, and the elites.
When we stray away from our core principles of freedom of speech, freedom of expression, and freedom of debate, democracy is lost. Today, I entered the transcript of the Joe Rogan Experience #1757 into the Congressional Record to preserve the podcast forever. Big Tech may be able to censor information on their own platforms, but they cannot censor the Congressional Record.”
Malone Permanently Banned From Twitter
Malone had been permanently banned from Twitter the day before, December 29, 2021. He suspects his ban was triggered by one of the two last posts he made. One was a link to the Canadian COVID Care Alliance’s website,5 with the comment:6
“Pfizer 6 month data which shows that Pfizer’s Covid-19 inoculations cause more illness than they prevent. Plus, an overview of the Pfizer trial flaws in both design and execution.”
The video, featured on the Canadian COVID Care Alliance’s website, reviews that Pfizer data. We will feature this excellent video later and go into far more details of how they exposed the fraud of Pfizer’s clinical COVID jab trial.
The other tweet that might have triggered the ban was a post about how the World Economic Forum manages global media in a lockstep fashion. Either way, Malone was permanently banned from the social media platform either for highlighting Pfizer’s own science — the very science we’re told to “trust” — or highlighting the WEF’s central role in the global censorship campaign.
Mainstream Media Are Losing the Information War
Interestingly, Rogan has become something of a key workaround to the universal mainstream media censorship. While Malone lost 512,000 followers on Twitter when they suspended his account, it’s rumored his interview with Rogan has garnered some 50 MILLION views across alternative free-speech platforms.7 As noted in a January 3, 2022, ZeroHedge article:8
“… nowadays when you make it on JRE, you’ve officially ‘made it.’ Putting aside the obvious irony of Twitter attempting to ban somebody and the person in question going viral as a result, I also thought about how, despite the fact that Malone’s opinions put him at odds with the mainstream media … Joe Rogan launched him past the usual media suspects and into the real ‘mainstream’ …
[In] 2022, the mainstream media as we know it today (CNN, MSNBC, ABC, CBS, etc.) is going to be forced to change its narrative on COVID. The idea of the media being forced to change its tune on Covid is something I touched upon a couple of days ago when I wrote about the Omicron variant and how the media is creating a mass hysteria mountain out of a mole hill.
But after listening to Dr. Robert Malone‘s well reasoned arguments, delivered for three straight hours, concisely and calmly, it became clear to me that the entire mainstream media machine could wind up falling at the hands of content creators like Joe Rogan.
Rogan generates so many views and has grown so quickly — strictly because he allows open dialogue, civil discourse and approaches things with honest intent … One issue for media and political elites to consider is the fact that Rogan has supporters on both sides of the aisle.
These supporters watch him because he routinely touches on topics that are considered faux pas or irreverent … Rogan has thrived, whether intentionally (bringing on people specifically because they are being censored) or unintentionally (shooting the shit with people he finds interesting), from the start, by shining light in the dark areas that the mainstream media refuses to discuss.”
Many Rogan fans agree that Malone’s interview is among the best interviews Rogan has ever done. I know, many of you are saying to yourself, I don’t have three hours to watch this interview. Well, let me encourage you to find the time. If 50 million people have watched this video, it is likely you could find the time.
Trust me on this one. You won’t regret it. It is such a pure joy and pleasure to listen to Malone’s relaxed, eloquent, masterfully precise language as he destroys the mainstream COVID narrative. You can watch it in bits and pieces, but this is clearly the best interview Malone has done and is on par with the Peter McCullough interview with Rogan a few weeks ago.
As explained by Malone, he has been involved in vaccine development and distribution for more than three decades, and played a crucial role in the development of the very technology that the Pfizer and Moderna COVID shots are based upon, so “If it’s not OK for me to be part of the conversation … who can be allowed?” Malone asked.
Indeed, as noted by Rogan, with its ban of Malone, Twitter basically banned “one of the most qualified people in the world to talk about vaccines.” Malone said he has attorneys looking at potentially filing some sort of lawsuit over the ban.
Of course, mainstream media and “fact checkers” (now legally defined by recent Facebook litigation as opinion promoters) call him a liar for saying he invented the mRNA technology currently used, but his name on 10 patents proves otherwise.
“No one can dispute that I played a major role in this tech,” Malone said. “And virtually all other voices that have that background have financial conflicts of interest. I think I’m the only one that doesn’t. I’m not getting any money out of this.”
Some of the cliff notes from Malone’s interview include the following:11
Government responses — Malone believes the U.S. government is “out of control” and “lawless” in their COVID response and that their actions have resulted in, probably, half a million excess deaths. COVID jab mandates are “explicitly illegal” as the shots are experimental. What’s more, people are not getting the information they need to be able to make an informed decision about the risks they’re taking by participating in this experiment.
Social psychology of the times — Malone believes the irrational behavior we’re witnessing is the result of “mass formation psychosis,” a societal diagnosis first presented by Desmet at the end of 2021.
Natural immunity — Natural immunity is more robust than “vaccine” induced immunity, and people with natural immunity also have a higher risk of adverse events from the COVID jab.
COVID jab risks — Malone actually took the Moderna shot, thinking it might help with some long-COVID symptoms he was having after getting seriously ill with COVID-19 in February 2020. He says he suffered some side effects from the shot, but that those effects have since resolved.
Malone expresses concern about post-jab myocarditis rates and the possibility of fertility problems. When it comes to reproductive health, he warns that the lipid nanoparticles in the COVID shots can have adverse effects on the ovaries.
He also reviews how the SARS-CoV-2 spike protein can cause blood clots, regardless of whether they come from natural infection or the COVID jab, and how the spike protein can disrupt the blood-brain-barrier.
Malone believes the reason some experience no or few adverse effects from the COVID shot has to do with phenotypic or genetic differences. He points out that diabetics and those with high blood sugar levels tend to be more affected by spike protein effects, for example.
Suppression of early treatment — Early treatment with drugs such as hydroxychloroquine or ivermectin is very effective and both drugs have also been safely administered for several decades. The Chinese anti-COVID protocol, obtained by Malone in February 2020, actually included hydroxychloroquine. When he got COVID-19, Malone also self-treated with femotadine (Pepsid). He’s now leading a clinical trial to assess its usefulness in the treatment of COVID.
Narrative management and global coordination of censorship — The Trusted News Initiative led by the BBC is central to the censorship campaign, according to Malone. It labels anyone who disagrees with the official narrative on vaccines as an “anti-vaxxer,” and suppresses anything that goes against “approved” sources such as Dr. Anthony Fauci and the World Health Organization.
He also points out that Thomson-Reuters, which has ties to Pfizer, is a primary fact checker of Twitter. Since they in part decide what’s allowed to be discussed on Twitter, Pfizer has this hidden influence as well (not to mention that James C. Smith, chairman of the Thomson Reuters Foundation, also has been a director at Pfizer and chair of their compensation committee since 201412).
COVID jab efficacy — Malone notes the window of effectiveness is ever shrinking, with some studies, such as one from Denmark,13 showing negative effectiveness against Omicron.
According to Malone, we’re administering a “mismatched vaccine” and driving the B and T memory cells toward a virus that is no longer in circulation. His hypothesis for why the shots stop working so quickly is because of this original antigenic sin. He explains:
“We’ve got a new pathogen [Omicron] but it’s got a series of overlaps with the old ones that we’ve seen before, and our immune system is biased to respond as if it’s the old one.
Now, to make matters worse, we’re taking the spike protein — only one of the proteins the dominant immunologically dominant protein — and we’re jabbing everybody multiple times, and driving memory cells and effector cells to a virus that is not the one we’re encountering.
So it could very well be that as you’re taking more jabs, you’re further skewing your immune response in a way that’s dysfunctional for infection to Omicron … When you see a signal this strong, it’s saying something’s going on you ought to pay attention to it in my opinion.”
Malone also sat down with InfoWars reporter Kristi Leigh within days of his Twitter ban.14 A highlight reel15 from the 80-minute interview is embedded above. In it, Malone described being “multidimensionally red-pilled” by the current censorship. He also discusses his journey of “coming to terms with what the World Economic Forum represents.”
Initially he resisted the idea that there was a global agenda underway aimed at stripping us of our rights and freedoms. He thought The Great Reset was fantasy — until he started looking into claims for himself and found this supposed “conspiracy theory” is fully documented and laid out for the world to see on the WEF’s own website. “And then you see [the plan] deployed,” he says.
Malone’s Warning to Parents
In another recent interview with the WND,16 Malone discussed two grassroots projects that he’s gotten involved with. The first is the Unity Project, which opposes vaccine mandates, and the second is the International Alliance of Physicians and Medical Scientists, launched by the Global COVID Summit.17
Malone also highlighted the second Physicians Declaration18 by the International Alliance of Physicians and Medical Scientists, dated October 29, 2021, in an article for The Defender.19
The declaration has been signed by more than 16,000 doctors and scientists, and states that “healthy children shall not be subjected to forced vaccination” as their clinical risk from SARS-CoV-2 infection is negligible and long term safety of the shots cannot be determined prior to such policies being enacted.
Not only are children at high risk for severe adverse events, but having healthy, unvaccinated children in the population is crucial to achieving herd immunity. The declaration also demands that health agencies and institutions “cease interfering with physicians treating individual patients.”
In the article, Malone also warned parents that the decision to inject their children is “irreversible,” and that they need to be aware of “the scientific facts about this genetic vaccine, which is based on the mRNA vaccine technology I created.” Here’s an excerpt from that written warning:20
“Before you inject your child — a decision that is irreversible — I wanted to let you know the scientific facts about this genetic vaccine, which is based on the mRNA vaccine technology I created.
There are three issues parents need to understand: The first is that a viral gene will be injected into your children’s cells. This gene forces your child’s body to make toxic spike proteins. These proteins often cause permanent damage in children’s critical organs, including:
Their brain and nervous system.
Their heart and blood vessels, including blood clots.
Their reproductive system.
This vaccine can trigger fundamental changes to their immune system.
The most alarming point about this is that once these damages have occurred, they are irreparable:
You can’t fix the lesions within their brain.
You can’t repair heart tissue scarring.
You can’t repair a genetically reset immune system.
This vaccine can cause reproductive damage that could affect future generations of your family.
The second thing you need to know about is the fact that this novel technology has not been adequately tested. We need at least 5 years of testing/research before we can really understand the risks. Harms and risks from new medicines often become revealed many years later.”
Again, I urge you to listen to Malone’s interview with Rogan, embedded at the top of this article, in its entirety. He covers a lot of ground, and does so in his calm and well-reasoned way. I can confidently assure you that you won’t have any regrets for making the time investment.
Make Americans Free Again, led by Pam Popper, is fighting to preserve American freedoms and has a proven strategy that ensures we can win
They are launching strategic legal challenges across the U.S. Rather than arguing the unconstitutionality of mandates, they challenge the legal basis of the emergency declaration that allowed the mandates to be rolled out in the first place
They also teach Americans everywhere how to start and build their own local parallel societies where members take care of each other and work toward the same goal
The short-, medium- and long-term goals of Make Americans Free Again are to free Americans from government tyranny, address all medical mandates and, ultimately, design and launch a superior medical system
Even if you don’t start your own freedom group, consider making a donation to Make Americans Free Again’s legal fund
Pam Popper is the president of Wellness Forum Health and cofounder of Make Americans Free Again, which plays a significant role in the fight to help preserve American freedoms. An important part of that task is building a powerful community and, as noted by Popper, “COVID has brought some people together who probably should know each other better,” and that includes us.
Popper and I are aligned with respect to our desire to educate the public about fundamental health principles, including foundational basics for preventing and treating COVID-19.
We are also in agreement that the COVID pandemic is a cover for something else entirely — a global takeover by powerful and profit-hungry interests. And finally, we both agree that participating in protest marches and signing petitions doesn’t really achieve much, and that there are far more effective strategies, as she has demonstrated.
“The background on the situation is my company, Wellness Forum Health, is about 27 years old, and our niche is informed medical decision making. In other words, we don’t tell people what to do. [We teach people] how to make decisions about health the way they make decisions about cars and houses and retirement accounts and other things that are important to them …
Now, the medical profession has become the Wild West. Medical journals are filled with inaccurate information. So, we added … rules for filtering evidence, and we teach people the rules. The rules are things like: Conflicts of interest have to be considered.
We have to understand the difference between a correlation, and a cause and effect relationship, [and] something that is statistically significant but clinically meaningless. You get the idea.
If you’re looking at a lot of information, you have to filter it based on rules, just like you have to play football based on rules … So, for 27 years, I’ve been talking about the problems in health care, which is [that] nobody abides by any rules. There isn’t any informed decision making. Doctors tell people to do things and they say, ‘OK, that’s called consenting.’
But that’s not consenting at all, in my opinion. And so, a lot of my research really was based on [that], and the books I wrote revealed the incompetence of big medicine, big food, big pharma, some of the criminal intentions, and that this [the COVID scam] isn’t new, it’s just a bigger version of it.
The second week in March of 2020, I knew what this was because I had covered fake pandemics in the past. There was one in the 1950s, there was one in the 1970s, another one in 2009. These are just the big ones that got a lot of attention. So, I knew what this was. I do some business in China; I knew what they were up to.
So, I put out this very controversial
. I didn’t think it was going to be controversial. I was just reporting the news, which I had done on video twice a week for [years].
Instead of the usual few dozen responses, I got 3,500 responses to this video and they included death threats and hysteria — ‘You’re going to be responsible for killing people’ — the whole 9 yards. And I thought, wow, this is just something else. So that’s how this all started.
If you go back and watch that original video, I said that this took place in China, they did it deliberately, that they had reasons and motivations for doing this, that this was a fake pandemic and the end game was forced vaccination. It was a 15-minute video, but that was the bottom line. And unfortunately, it turned out to all be true. I wish I’d been wrong about it.
As [the pandemic] went on, I just kept doing more and more research, posting more and more videos. And at some point, probably late spring or early summer, I realized the breadth and depth of this whole thing and knew that they were never going to stop, and we had to do something about it. That’s when we formed Make Americans Free Again.”
Litigation Efforts
One of the primary ways in which Make Americans Free Again is fighting the tyranny is by filing lawsuits against mask and COVID jab mandates. She explains:
“We have three branches of government, and the executive branch — with very few exceptions, for example, Ron DeSantis in Florida — has gone completely rogue. They now operate as emperors and empresses, rulers over their people. So, you can’t deal with those people. The legislatures up until recently have been fairly useless.
The only reason they’re doing anything now is really to protect themselves, in my opinion, not because they’re looking out for people. So, you have one branch of government left, which is the courts. We [knew] we were going to have to use that in order to a) get our freedoms back and b) go after these people for what they did, which is committing fraud and hurting and killing people.”
By early summer 2020, a slew of lawsuits had been filed across the U.S. Unfortunately, it was highly uncoordinated. People weren’t thinking things through. There was no cohesive strategy, and that was their downfall, Popper says. She estimates some 6,000 lawsuits have failed in court, causing many to give up on the judicial system as well. Not Popper, though.
“We’ve been winning in court and I’ll tell you how in a minute. But it is better to stop, think and [then] do something. Less activity, more deliberately performed, is a better idea.
Interestingly enough, I heard from this lawyer in Florida who had made the same observation as me. This hurry up and file strategy isn’t working, so why don’t we look at these lawsuits and figure out what they’re doing wrong? And this is very, very important for anybody listening to this who just wants to hurry up and file.
What people were doing was filing the lawsuit against the government saying, ‘You are violating our constitutional rights.’ And you know what the government would say? ‘Oh, we know we are, but we don’t have any choice because it’s an emergency.’ And then the judge would rule in the government’s favor.
We filed the very first lawsuit challenging the emergency declaration itself in Ohio, accusing our governor of fraud. We said, ‘There is no emergency. You declared this fraudulently, and therefore all the actions that you’ve taken are not warranted.’ And the thing that I think people don’t realize, not living in Ohio, is that we were the model state.
People think it’s California [or] New York, but we were the first to shut down, first to close the schools, first to cancel events, first to close bars and restaurants. Why is that? Because the criminals behind this needed a very popular conservative governor who could do well on Fox and CNBC and MSNBC. Every Sunday, our little criminal was the toast of the Washington shows. He was so responsible, taking care of his people.
By the time we filed our lawsuit on August 31 [2020], we knew a second shutdown was coming. By this point in time, we had some intelligence coming from government employees and that sort of thing. We never got locked down a second time.
We won when we filed, because we avoided the second lockdown. I think that the people behind this told the emperor, DeWine, ‘Let this alone, don’t do something that would make this judge just snap his fingers and order discovery.’ So, we didn’t get a shutdown.
The other thing that happened is there was virtually no enforcement of the restrictions that were left in terms of gathering limits and that sort of thing … Because of that, we thought, OK, this is a good strategy. So, we started doing more of it and we filed several lawsuits in several states.
For those people who don’t have confidence in the court, first of all, look at some of the lawsuits that have been filed. They’re bad ones. If I was the judge, I would throw them out too, because the judge can’t make law. The judge has to go with what the law says.
The second thing is that there are bad judges and bad courts, but our strategy has been to file with a coordinated legal team, because the most important thing they want to avoid, and we’ve seen this in every lawsuit, is discovery, because discovery is where we get to depose Mr. Fauci; discovery is where the CDC has to give us the documents. I don’t need them 36 times. I need them one time and then the whole legal team gets them.
One judge in the United States of America someplace is going to give us discovery. I can’t talk about where, but we think that’s in the process of happening right now in one of the court cases, and then everybody will [have that information].”
Progress Report
Cases Make Americans Free Again have won include one in which they represented the New York City police. They won an injunction until trial on the COVID jab mandate for the police force. In Florida, their attorney won a lawsuit against the City of Gainesville, which was implementing a “vaccinate or terminate” policy.
They’ve also seen general changes in behavior as a result of these and other lawsuits. “We’ve put the criminals on notice that now judges are watching, so everything you do is subject to being hauled back into court and saying, ‘Look at what these people are doing.’” Popper says.
Across the U.S., they’re challenging the emergency orders, demanding the state prove there’s an actual emergency afoot. So far, none has been able to provide any evidence that COVID-19 is a public health emergency. Instead of proving an emergency exists, state defense lawyers have spent all their energy on motions to have the cases thrown out.
In Ohio, Popper feels they have been successful by applying pressure on the governor through the courts. DeWine converted the Ohio State Fair to a virtual event, and it appeared that he was planning to restrict or cancel big summer events. But in what many people considered a surprise, he lifted the emergency declaration and made Ohio a free state. We’ll never know, but it might have been because our case was still pending in court. We then withdrew it because we got our way.
Popper is also planning to make some still yet unrevealed announcements. “We’re getting ready for some really wonderful first of the year surprises for the criminals in charge,” she says, “so stay tuned.”
Rampant Lawlessness
Of course, they’re now trying to convince everyone that Omicron is a lethal threat, hence the emergency powers must remain in place, but even in the absence of a clear threat — as many now see through the fearmongering — they’re likely to keep pushing for more restrictions, vaccine passports, mask mandates and everything else. As noted by Popper:
“They don’t seem to require any justification for anything, they just do what they want. We’ve degenerated to living in a completely lawless society where people get up every morning and decide what they’re going to do, much the way that communist leaders and totalitarian dictators do.
I mean, our government resembles more the government of China or North Korea than it does what we used to have. So, I don’t think that they really need to justify the emergency use authorization. If they decide they’re going to do it, they’ll just do it, and they’ve stopped giving reasons.
To that point, I thought it was very interesting when Rochelle Walensky, the head of the CDC, said, ‘We’re going to cut the quarantine back to five days because that’s about all we can get people to do.’ So, in other words, our new policy is as much tyranny as the public will swallow.
She also made a stunning admission that their research showed that the compliance with quarantine was less than 30%. That goes to what I’ve been saying all along, which is that the resistance is much bigger than most people realize.
This is certainly what I’m experiencing building our organization. They do a great job of making it look like everybody’s on board, but everybody’s not on board. And I still contend that the vaccination rate is very, very low. I think they can’t even get to 60%. It was under 50% last summer. I was able to prove it with their data …
The compliance rate has been exaggerated and it was all a mirage to try and get people to say, ‘Well, if everybody else is doing it, I’ll do it too. It must be OK,’ because at that point in time, last summer, people didn’t know a lot of people who’d been injured or died. I think everybody knows somebody who’s been injured or died from this now.”
The number of parents refusing to jab their children is also a clear majority. According to Popper, parents have taken their children out of schools that mandate the COVID jabs, and some schools have had to reverse course as a result. Case in point: The Los Angeles school system dropped the COVID jab requirement when they realized they had 30,000 unvaccinated students and if they all left, the whole school system would cease to exist.
“Even The New York Times covered a school in Brooklyn that had eight teachers with nobody to teach,” Popper says. “That’s the level of resistance.” Meanwhile, media are trying their best to make it seem as though compliance is high across the board. She recounts one example, where a local paper claimed compliance with the mask mandate was nearly 100%, when wherever you went, the vast majority were maskless.
“So that is the level of propaganda. All you have to do is walk into a store and know that there is no compliance. And then the newspaper, obviously, that was a preprint sent to them a long time ago, [telling them that] at such and such a time, you’re supposed to publish this. It’s just laughable.”
Building Community and Parallel Societies
Popper has also made great strides in community building, which I believe is a crucial strategy for safeguarding our freedoms in the long term. This was a natural outgrowth of the legal work. They realized they needed a lot of people to contribute funds, so they needed to connect with people who were willing to pitch in to save our freedoms.
“We had the first meeting in my office last summer and there were five people there — me and two people who I work with, and two guests. And so, we agreed to do it next week, and those two people brought people. And something happened that I did not plan. I’m going to be very honest about this. I’d love to tell you that I preconceived all of this and then acted on it.
But people would come into the meeting and they would have that shell-shocked look — like my church is closed, my neighbor’s not speaking to me, I’m realizing what’s going on with my kids, it’s ridiculous. The organizations I used to be involved with, they don’t exist anymore.
And so now they’re starting to make friends, and people who have their kids at home are starting to connect with each other, and all this kind of stuff. And I had this epiphany one night. The No. 1 thing these people don’t want us to do is congregate, which means the most important thing for us to do is congregate.
So, that was the beginning of building not only the body of people it would take to fund what we need to do, but what I call the Make Americans Free Again parallel society. A year and a half later, we now start a new group every three or four hours in the United States. I’m not kidding. They’re all over all 50 states. They’re everywhere.
Here’s the way this works. It is a parallel society, so, the first thing is, everything you need, you can get your group. People found out that there were churches that didn’t close, because none of this gets advertised. You try to stay under the radar screen. So, churches that were not closed, you could go there and you didn’t have to wear a mask.
People found doctors, dentists that didn’t make you wear a mask … So, we lived a parallel life. During the worst of everything in Ohio, our people lived a pretty normal life. We had a fundraiser with 400 people when the gathering limits were 10, because we knew where to do it. One of the members of our group owned a place where we could do it.
People have also found new jobs … It is a very much cloistered society where we do business with one another. We homeschool our kids together, we pool our resources to fund these lawsuits, our social life is together.
We did this program called Small Business Rescue where we would support businesses in our community. The government doesn’t have any plan for these people, so we buy local, we support them. So, it is a parallel society.”
Make Americans Free Again societies are also looking for and finding doctors who are operating cash practices (so they’re not reporting to or taking orders from anybody) and who will provide early treatment for COVID.
“So, everything you need, you get from your group … and I can tell you right now, I can say this with a great deal of confidence, if I needed something, a place to live, if I didn’t have any food, if I needed money, if I needed medical care, if I needed a job, you know where I get that?
From my Thursday Group and the Thursday Group network. [Editor’s note: It’s called Thursday Group because the group meets on Thursdays.] This is what is missing. If this had all been in place [before the pandemic], they could never have done this to us. They took advantage of the fact that society’s quite fractured, that you don’t have these local connections.
People beat me up sometimes a little bit. ‘Why won’t you let people have Zoom meetings?’ Here’s why. If we need to save a business in Worthington, Ohio, somebody in Portland, Oregon can’t help us do that. You can’t eat at this restaurant every week and support them. It has to be local, local, and it has to be in person.”
2022 Prognosis
In the interview, Popper describes the many homeschooling benefits and successes members are reporting, which is profoundly encouraging. Overall, the community building, the parallel structures being created across the U.S. give her an optimistic outlook on the future. They’re proof positive that the whole takeover agenda is backfiring on the technocratic deep state.
“I’m optimistic with a qualifier,” she says. “I always want people to understand that I understand the gravity of the situation. If you have a spouse in the hospital right now who’s being slaughtered with ventilators and remdesivir, my rosy prognosis might strike you like nails on a chalkboard.
I want people to know the reason I get up every morning — the reason I invest so much of my own money and time, and I’ve risked my own life to do this — is to make that right.
Having said that, with that disclaimer, my outlook for this year is really positive and optimistic. The reason I say that is [because] we have a quantifiable enemy. We know what they’re up to. I am watching them scramble and fail. There is only one reason why they would be issuing all these edicts and Biden would say something like, ‘I’m losing patience’ … is because they’re not getting their way.
I think the best example of that is the CDC walking back the recommendations on the quarantine, because we just can’t get people to do it. It’s a stunning admission really to the public. So, I think this is going to be a year when this goes away.
Even the Israeli government is saying we’re going to make everybody get a fourth shot, but maybe we’re just going to have to let everybody go out and mingle and get some herd immunity. There is an awakening of the government that they need to change course …
I like an enemy that’s on the defensive. It’s gone from the offensive to the defensive. That means, and I’ll give you another caveat, that there are probably more horrifying things in store as they flail about and try to hang onto their power.
A couple things I’ll recommend. Scott Atlas was a speaker at our conference this last year and he’s the former adviser to President Trump. He wrote a book called ‘A Plague Upon Our House.’ It’s a horrifying book, mainly because he reveals the stupidity and ineptitude of people like Fauci and Birx.
Atlas told us that Fauci can’t even pronounce medical terms properly and Birx doesn’t understand statistics. Most eighth graders have a better grasp of math than she does. What people like that do is they flail about when they are failing because they don’t have the skill set to do anything else … So we’re going to see some of that kind of behavior, but at the end of the day, this time next year, I think we will be in an entirely different situation.
A lot of our freedoms will be restored and a lot of the nonsense will go away. Then it just is a matter of spending the rest of our lives, just like we’ve done with the Nazis, tracking these people down and making them pay for what they did. And believe it or not, last fall, they were trying a 100-year-old Nazi in Berlin for what he did. So, it’ll be the same thing. We’ll be looking for them in South America, in China and every place else to bring them to justice.”
How to Start Your Own ‘Thursday Group’
For liability and other reasons, Make Americans Free Again cannot connect you with already existing groups. You have to start your own, which is what they teach you. Popper explains:
“It’s easy. We provide everything you need. My email address is [email protected]. You can email me. I hold conference calls every week during which I share our entire strategy and tell people how to get started working with us … Get engaged with us, donate money if you can.
Do what you need to do to keep yourself in a positive frame of mind, and starting a group and gathering a group of like-minded people is important …We can go from having felt quite powerless to being the most powerful people in the country, if we’re smart about it.
You start with one other person. People forget, I’m leading a group with hundreds of thousands of people, but it started with two guests. So, you just start with somebody who sees things the way you do. We give you a meeting format. We have training programs for our meeting leaders.
We have meeting leader conference calls every other week. We have a meeting leader coordinator in the office … Every Thursday, we send out the update, what the agenda is going to be, here’s the video you’re going to show, so nobody has to spend all day researching what am I going to talk about. We follow the same format every week, so we make it as easy as possible. And that’s how you start.
I heard a lot from people when this all began, ‘I don’t know anybody and it’s too hard, this is outside of my comfort zone.’ The longer this has gone on, the more people have said, ‘What’s going on is so far outside of my comfort zone that starting this group seems like it’s easy by comparison.’ So, I promise you, if you do this, we’ll support you in every way possible, and you can’t mess it up if you just follow our format.
We have a strategy that means we win at stuff. We don’t take on things that don’t result in winning. For example, I don’t have any particular objection to petitions and declarations, but I haven’t seen them solve this.
The Great Barrington Declaration got half a million signatures and tens of thousands were doctors and well-respected health professionals. It did nothing. Great statement, but it doesn’t change anything.
The biggest protests in the world are in Germany and Australia. Take a look over there, that doesn’t change anything. Protests are great for people to get together, but when you promise people that it’s going to make a difference and it doesn’t, it demoralizes them.
We have people who are demoralized. They need to feel like they’re winning, and when people come to our groups, what they see is winning. You save a business, you win. You get a kid out of school, you win. You raise money and file a lawsuit, you win. Winning is what we need for people to feel good. Getting them involved in more stuff that results in failure, not so good. So, we’re really focused and disciplined.”
More Information
I really encourage you to consider creating your own Thursday Group. To do that, send an email to Popper at [email protected] and ask to be added to her weekly conference call.
Nebulized hydrogen peroxide is a safe, inexpensive and incredibly effective way to prevent and treat viral illnesses of all kinds
While hydrogen peroxide kills viruses, it also kills other pathogens that can contribute to an unhealthy gut and/or oral microbiome. As such, it may also improve your microbiome and help resolve a wide variety of other chronic ailments, including gut problems and periodontitis
Hydrogen peroxide is part of your body’s natural defense against pathogens. So, when you nebulize hydrogen peroxide, you’re really just augmenting your body’s natural defense system
Being able to treat yourself at home at the Lrst signs of COVID-19 symptoms will also virtually eliminate your risk of long-haul syndrome. So far, medical doctors who have treated COVID-19 patients agree that if treatment begins early enough, patients almost always fully recover and have no longstanding side effects from the infection
Buy the required supplies before you need them, so you have everything and can treat yourself at the rst signs of symptoms. Most of the time, after two or three treatments, the infection will be stopped in its tracks
Levy has suffered with lifelong sinus problems and about a year and a half ago, while doing research for his book on magnesium, he came across nebulization with magnesium chloride, which sparked his interest.
As a result of his research, he began nebulizing with hydrogen peroxide and noticed “incredible changes in my health” almost immediately, including the reversal of his chronic sinus problems. So, after nishing his magnesium book, he took a deep dive into nebulization. “Rapid Virus Recovery” is the result of that journey.
“Just about the time the pandemic hit was when I really had my most compelling compilation of evidence for what nebulization with hydrogen peroxide can do,” he says. “And as I point out in the book, this is not just for common cold. It is for any respiratory virus.
I make the assertion — and I don’t generally make assertions that I can’t back up — that nobody needs to suffer with a cold or the u again, unless you wait too long before nebulizing. Nevertheless, you’ll still recover much quicker after you do this.”
Levy also points out that if you can easily prevent or cure a viral infection, then vaccination becomes irrelevant. “Why vaccinate for a disease that you can prevent or easily cure after you have it?” he asks.
As for why he’s giving the book away for free, the answer is simple. “I want to stop this pandemic,” he says, “and nebulized hydrogen peroxide is not only simple to administer by yourself and universally effective, but it’s also inexpensive and readily available around the entire world, including in areas where other remedies such as vitamin C or ozone can be hard to come by.”
Early Treatment Virtually Eliminates Complications
Being able to treat yourself at home at the Lrst signs of COVID-19 symptoms will also virtually eliminate your risk of long-haul syndrome. So far, medical doctors who have treated COVID-19 patients agree that if treatment begins early enough, patients almost always fully recover and have no longstanding side effects from the infection.
The reason for this is because the virus replicates wildly during the first few days of infection, and this is the time during which it can cause longstanding damage. So, it’s important to be prepared.
Buy the required supplies before you need them, so you have everything and can treat yourself at the rst signs of symptoms. Most of the time, after two or three treatments, the infection will be stopped in its tracks. As noted by Levy, you get same-day resolution, which is almost unheard of in clinical medicine.
My personal experience with friends and family also mirrors these type of dramatic results. In all my years of practicing medicine, I have never seen such an effective intervention for the nearly immediate resolution of viral illnesses, so long as it’s implemented shortly after the symptoms start.
If you miss that early window and start developing more pronounced symptoms of in uenza or COVID-19, nebulized peroxide is still an excellent adjunct to any other treatment you may be doing.
“I want to emphasize that because to the best of my knowledge, and I’ve done quite a bit of research on this, I see no circumstance in which hydrogen peroxide nebulization interferes with or lessens the impact of any other positive intervention,” Levy says.
One such intervention is vitamin C, which Levy describes as “the perfect physiological partner” with hydrogen peroxide, as they have powerful synergistic effects that facilitate rapid resolution of the infection.
Hydrogen Peroxide Is Part of Your Body’s Natural Defenses
Hydrogen peroxide is part of your body’s natural defense against pathogens and is found in virtually all cells. Your body requires it. It’s a powerful signaling molecule, and there are organelles in your cells that use it to kill pathogens directly. So, when you nebulize hydrogen peroxide, you’re really just augmenting your body’s natural defense system.
“Hydrogen peroxide serves as an incredible storage form for oxygen to your body. That’s actually what sort of happens once you activate hydrogen peroxide, and there’s nothing in your body, pathological speaking, that oxygen is not good for. ~ Dr. Thomas Levy”
Levy explains:
“One of the interesting things I found in the course of this research is that up to 5% of the oxygen you inhale gets incorporated into producing new hydrogen peroxide inside your body. Also, contrary to much scienti c thought, except in the wrong microenvironment, hydrogen peroxide is very stable. It doesn’t do a lot of spontaneous breaking down or spontaneous oxidation.
So, it serves as an incredible storage form for oxygen to your body. That’s actually what sort of happens once you activate hydrogen peroxide, and there’s nothing in your body, pathological speaking, that oxygen is not good for.
This is what makes peroxide a perfect therapeutic agent. It not only kills pathogens extremely ePciently — virus, fungus, protozoa, bacteria, you name it — but it also leaves behind, as metabolic byproducts, water and oxygen.”
Once the infection is resolved, the water and oxygen will both help heal any tissue damage caused by the pathogen. The water will also help dilute the acidity introduced
by the infection. “So, it’s very clear, at least to me, that the best way to refer to hydrogen peroxide is as nature’s naturally designed antibiotic,” Levy says.
How Hydrogen Peroxide Works
Hydrogen peroxide can impact a variety of bene cial pathways in your body, but in terms of pathogens, one of the most prominent ones appear to be through the Fenton reaction inside the pathogens and the infected host cells. As explained by Levy:
“The Fenton reaction1 is a way of getting hydrogen peroxide to break down into a hydroxyl radical, which is the most potent oxidizing agent known to science … In a nutshell, oxidation is disease, and limiting and reducing oxidation brings you back to health.
That might sound like an oversimpli cation, but not so much … When you want to kill a pathogen or kill an infected cell, you want to continue the inYux and the power of that oxidative action until there’s so much oxidative stress that the cell ruptures and dies, or the pathogen ruptures.
So, you need unlimited supplies of vitamin C, unlimited supplies of iron, and unlimited supplies of peroxide. That’s the only way to keep the Fenton reaction going inde nitely until it does the task … This is why high-dose vitamin C given intravenously is so powerful …
It powerfully promotes the production of new hydrogen peroxide, which because of its small ionic nature is able to diffuse into the cell. At the same time, the vitamin C goes into the cell. It produces more peroxide that goes into the cell with it.
The third part of the equation [is that] the hydrogen peroxide works to mobilize iron from the storage forms inside the cell … Furthermore, the pathogens self-target themselves by actively accumulating iron in order to proliferate and make themselves iron-rich.
So, there you have all three components: electron donor, electron transfer, electron receiver … and this proceeds until you get complete resolution of the infection.”
Your primary pathogen-killing immune cells, macrophages, polymorphonuclear leukocytes and monocytes, also bring vitamin C and hydrogen peroxide in massive amounts to the site of in ammation or infection.
How to Prepare Your Nebulizing Solution
One of the most important parts of the treatment, however, is to make sure you have the equipment BEFORE you need it. So, if you haven’t already purchased your nebulizer supplies, please put that on your to-do list now. To be prepared for any eventuality, you’ll want to buy the following items so that you have them on hand:
An electric, plug-in tabletop jet nebulizer (small battery-driven hand-held devices tend to be ineffective due to their reduced power)
Food-grade hydrogen peroxide (which does not contain any harmful stabilizers)
Normal saline (0.9%) solution (alternatively, you can easily make your own at home)
The peroxide needs to be diluted with saline, not tap water or distilled water, as this could potentially in ame the mucosal cells. You need the salt in there. As noted by Levy, “The literature shows that water by itself does aggravate, or can cause, an irritating cough if you nebulize it by itself.”
I recommend diluting the peroxide down to 0.1%. Brownstein recommends using an ultralow dilution of 0.04% while Levy recommends 3% or less, depending on individual patient tolerance and how sick the patient already is.
If you don’t have access to saline, you could make your own by mixing one teaspoon of unprocessed salt (such as Himalayan salt, Celtic salt or Redmond’s real salt) into a pint of distilled water. This will give you a 0.9% saline solution, which is about the concentration found in body fluids. Using that saline, you will then dilute the hydrogen peroxide as described in this chart.
With regard to the dilution, Levy offers the following commentary:
“I don’t think there’s any evidence really that 0.04% nebulization as a monotherapy is going to get the job done. I want something that anybody on the planet can use to resolve [their infection] without having to add vitamin C, without having to add iodine, without having availability of ozone.
And when you start taking the concentration down, you’re going to get less antipathogenic impact by de nition. That, combined with the fact that for a year now, I’ve been getting an incredible amount of positive feedback. I’ve had no negative feedback. Most people use 3%. Some get too much tingling in the nose and they’ll go down to 1.5% or even 1%.
I think it’s a whole different thing as to what concentration you might want to use for the maintenance therapy that we’re talking about. But I think there’s no good reason at all not to take your rst shot at 3% when you’re already having symptoms, or if you have a COVID-positive test.
I see no reason to dance lightly, especially in the fact that we have no negative feedback. Also, a recent article showed that people who routinely gargle with 3% peroxide show zero microscopic abnormalities in the tissue after a six-month period …
I never advise somebody to tolerate symptoms that they nd uncomfortable. I always say, nd a concentration of whatever you’re nebulizing that’s comfortable. But that said, I still think when you clearly have an infection, hit it hard the first few times, I don’t think you’re going to do any damage.”
“I’ve had a lot of feedback from chronic lung patients that are pretty much ecstatic that they were able to incorporate this into their long-term medical treatment protocols,” Levy says.
Another interesting beneKt of this therapy is its ability to improve your gut microbiome.
Levy appears to have been the Rrst one to discover and discuss this benefit:
“The Lrst time I nebulized with, at that time, regular over-the-counter 3% peroxide, the next morning I had the most incredibly normal, well-formed bowel movement of my life. I said, ‘Good grief. What is going on here?’ The only thing I did different was the peroxide nebulization the day before, and that got me to thinking about how all disease is oxidation versus reduction.”
As noted by Levy, chronic infection is a primary source of toxins in the body for most people, be it from infected tonsils, teeth, gums or anything else, and this also affects your microbiome.
Nebulized hydrogen peroxide, by addressing these chronic infections, may therefore also help reestablish a healthier bacterial balance in your gut. Levy recounts how patients with chronic irritable bowel syndrome were able to reverse their condition in as little as one week of nebulization.
“I don’t want to oversimplify what’s going on in the gut,” he says. “I know it’s a very complex process, but bottom line is that what keeps any tissue in a state of ‘disease’ is increased pro-oxidant factors coming in and the degree to which you can stop those pro-oxidant factors.
With my bowel habits changing in less than 12 hours, that really tells me, intuitively, how readily a leaky gut can heal if you stop the 24/7 onslaught of new toxins and pathogens getting dumped into the gut …
I don’t think nebulization is directly putting a clinically signi cant amount of peroxide in and around the gut. Its primary role is killing the pathogens that chronically grow there in the nose and throat, preventing a continual swallowing of pro-oxidant pathogens and their associated toxins.
There’s a concept in my book called chronic pathogen colonization, where those bugs are covered with bioXlms, and … peroxide destroys the bio lm quickly and then kills the pathogens underneath …
I think peroxide nebulization should be a routine part of any treatment protocol for any medical condition because of the positive impact it has on the microbiome and leaky gut, which makes any chronic disease you have worse.”
Hydrogen Peroxide for Periodontitis
A third benefit is its ability to address gum disease (periodontitis) and all the various health conditions associated with or worsened by it. As just one example, if you have severe asthma and advanced periodontitis, when your periodontitis ares, so will your asthma. Once you start to resolve the periodontitis, your asthma will typically improve as well.
“What’s unique about periodontitis is the nature of the pathogens,” Levy explains. “Often it’s caused by a bug called Porphyromonas gingivalis. They’renow finding this pathogen by advanced PCR testing to be present in many different tissues in the body, and to be present in tissues that are diseased.
They’ve identified it in Alzheimer’s tissue, in different neurological tissues. It’s been identiMed in the coronary artery linings of patients that have coronary artery disease …
That’s all coronary artery disease is — a chronic immune response that’s never extinguished because the seeding of bugs from the mouth is never extinguished … The reason smokers have such a high incidence of heart disease is because all of them have induced periodontitis that has the type of pathogen that metastasizes to the coronary artery lining.”
On a personal note, last year during a health checkup at SanoViv in Mexico, I learned I had periodontitis, which surprised me considering I don’t smoke and have a very healthy lifestyle. It goes to show how easily it can happen and, according to Levy, one of the reasons for this is depleted vitamin C stores. I was able to completely reverse it using ozone therapy, but as noted by Levy, the depleted vitamin C also needs to be addressed. He says:
“One main de ciency of things like ozone and other bio-oxidative therapies is they’re highly effective at killing the pathogen, but they’ve got nothing to do with restoring the antioxidant vitamin C status that resulted from the pathogen being present. All these viruses that we get acutely rapidly destroy our vitamin C stores.
Things like Ebola, where people die of hemorrhage, that’s really acute scurvy. In fact, it’s my opinion that long-haul COVID-19 is simply because of the fact that you so effectively nuked a large amount of your nutrients, especially vitamin C, that unless you undergo an accelerated plan of restitution, not a maintenance plan, but an accelerated plan of restitution, you’re never going to get back to baseline.
Same thing with periodontitis. Any dentist will tell you, they’ve never seen a smoker with normal gums. It just doesn’t occur. But the point is that smoke is metabolizing the vitamin C rapidly in the gums themselves.”
While you would get some bene t by nebulizing hydrogen peroxide through your mouth (i.e., breathing through your mouth rather than your nose), Levy recommends using a water irrigation (Waterpik™) device for this. Use warm water or warmed saline and add one-half to 1 or even 2 tablespoons of 3% food-grade hydrogen peroxide to the water tank.
“Those pathogens get knocked out quick. When you have advanced periodontitis, you no longer have the little peaks of gum tissue between the teeth. They’ve just resorbed completely.
But even in that type of gum, I’ve seen new gum grow in quite nicely in a couple of weeks. So basically, when you take the ongoing infective presence out of there, they will regenerate rapidly, especially if you’re not smoking while maintaining a good vitamin C intake.”
More Information
If you don’t have any chronic medical condition, Levy suggests nebulizing hydrogen peroxide two to three times a week for one to three minutes. If you have a chronic health condition, you’ll want to do it more frequently. For acute symptoms, you’ll typically want to nebulize for 10 to 15 minutes at a time.
For more details, be sure to download Levy’s book, “Rapid Virus Recovery.” It’s a free download. Also be sure to share it with your friends, family and social networks. Nebulized hydrogen peroxide is a simple, inexpensive way to improve your health and safeguard against viral infections of all kinds, and anyone can use it.
“Send the link to as many people as possible,” Levy says. “That’s the whole reason for this book. I can’t imagine anybody being offended by the offer of a free book.”
Meditation is the habitual process of training your mind to focus and redirect your thoughts. The popularity of meditation is increasing as more people discover its many health benefits. You can use it to increase awareness of yourself and your surroundings. Many people think of it as a way to reduce stress and develop concentration. People also use the practice to develop other beneficial habits and feelings, such as a positive mood and outlook, self-discipline, healthy sleep patterns, and even increased pain tolerance.
1. Reduces stress Many styles of meditation can help reduce stress. Meditation can likewise reduce symptoms in people with stress-triggered medical conditions.
2. Controls anxiety Meditation can reduce stress levels, which translates to less anxiety. Habitual meditation can help reduce anxiety and improve stress reactivity and coping skills.
3. Promotes emotional health Meditation can improve depression and reduce negative thoughts. It may also decrease levels of inflammatory cytokines, which could contribute to depression.
4. Enhances self-awareness Meditation may help you develop a stronger understanding of yourself, helping you grow into your best self. Self-inquiry and related styles of meditation can help you “know yourself.” This can be a starting point for making other positive changes.
5. Lengthens attention span Focused-attention meditation is like weight lifting for your attention span. It helps increase the strength and endurance of your attention. Meditation may build your ability to redirect and maintain attention.
6. May reduce age-related memory loss. Improvements in attention and clarity of thinking may help keep your mind young. The improved focus you can gain through regular meditation may boost your memory and mental clarity. These benefits can help fight age-related memory loss and dementia.
7. Can generate kindness. Metta, or loving-kindness meditation, is a practice of developing positive feelings, first toward yourself and then toward others. Metta increases positivity, empathy, and compassionate behavior toward others.
8. May help fight addictions. The mental discipline you can develop through meditation may help you break dependencies by increasing your self-control and awareness of triggers for addictive behaviors. Meditation develops mental awareness and can help you manage triggers for unwanted impulses. This can help you recover from addiction, manage unhealthy eating, and redirect other unwanted habits.
9. Improves sleep. Nearly half of the population will struggle with insomnia at some point. A variety of meditation techniques can help you relax and control runaway thoughts that can interfere with sleep. This can shorten the time it takes to fall asleep and increase sleep quality.
10. Helps control pain Your perception of pain is connected to your state of mind, and it can be elevated in stressful conditions. Meditation can diminish the perception of pain in the brain. This may help treat chronic pain when used to supplement medical care or physical therapy.
11. Can decrease blood pressure Meditation can also improve physical health by reducing strain on the heart. Blood pressure decreases not only during meditation but also over time in individuals who meditate regularly. This can reduce strain on the heart and arteries, helping prevent heart disease.
12. Accessible anywhere People practice many different forms of meditation, most of which don’t require specialized equipment or space. You can practice with just a few minutes daily.
There are many styles of meditation. We are going to focus on Centering Prayer.
The Guidelines 1. Choose A Sacred Word As The Symbol Of Your Intention To Consent To God’s Presence And Action Within.
2. Sitting Comfortably And With Eyes Closed, Settle Briefly, And Silently Introduce The Sacred Word As The Symbol Of Your Consent To God’s Presence And Action Within.
3. When You Become Aware Of Thoughts, Return Ever-So-Gently To The Sacred Word.
4. At The End Of The Prayer Period, Remain In Silence With Eyes Closed For A Couple Of Minutes.
The bottom line Meditation is something everyone can do to improve their mental and emotional health. You can do it anywhere, without special equipment or memberships. Alternatively, meditation courses and support groups are widely available.
Low vitamin B12 and vitamin D levels, along with increased homocysteine, may play a role in depression among children and adolescents
While there was no significant difference in folate levels between the depression and control groups, 11.23% of those with depression had low levels of folate
Both vitamin B12 and folate have previously been described as antidepressant nutrients; folate is found in dark leafy greens like spinach and avocados while vitamin B12 is found only in animal foods such as grass fed meat, eggs, dairy and wild-caught seafood
Vitamin B12 also helps regulate homocysteine levels, and increased homocysteine is linked to B12 deficiency as well as depression
Ensuring youth are eating healthy diets rich in folate and vitamin B12, as well as optimizing their vitamin D levels, may go a long way toward bolstering mental health and avoiding conditions like depression
This article was previously published July 2, 2020, and has been updated with new information.
Up to 2.5% of children and 8.3% of adolescents suffer from depression, a condition that’s associated with significant complications later in life, including an increased risk of suicide, substance abuse, physical diseases and problems with work, academic and psychosocial functioning.1
It’s believed that both genetic and environmental factors play a role in why some children develop depression, and increasing attention has been placed on the role of dietary factors and nutrients such as vitamin D, which is ideally obtained via sun exposure.
Further, one-carbon metabolism, which includes vitamin B12, folate and homocysteine and which plays a role in many biological processes and maintaining cellular homeostasis, has been investigated for its role in psychiatric disorders, including depression in adults.2
After exploring the link further, researchers from Ordu University in Turkey revealed that low vitamin B12 and vitamin D levels, along with increased homocysteine, may play a role in depression among children and adolescents.3
Childhood Depression Linked to Low Vitamin B12, Maybe Folate
The study involved 89 children and adolescents with depression, along with 43 subjects without depression to serve as controls. The volunteers completed testing for childhood depression and anxiety and had their levels of folate, vitamin B12, homocysteine and vitamin D measured.
While there was no significant difference in folate levels between the groups, 11.23% of those with depression had low levels of folate. Further, among the depression group vitamin B12 and vitamin D levels were “clearly low.” As for how this might contribute to depression, the researchers explained:4
“One-carbon metabolism has a basic role in methylation processes of neurotransmitters, proteins, and membrane phospholipids. Additionally, it is necessary for DNA synthesis.
With vitamin B12 and folate deficiency, methylation processes are hindered and neurotransmitter levels fall. Also linked to vitamin B12 and folate deficiency, there is an increase in the levels of the extremely neurotoxic metabolite of homocysteine.”
Both vitamin B12 and folate have previously been described as antidepressant nutrients.5 Folate, found in dark leafy greens like spinach, avocados and other fresh vegetables, is involved in your body’s production of mood-regulating neurotransmitters. In one study, people who consumed the most folate had a lower risk of depression than those who ate the least.6
Vitamin B12 is found only in animal foods such as grass fed meat, eggs, dairy and wild-caught seafood. As such, vegetarians and vegans are especially susceptible to B12 deficiency, and this is one likely reason why vegetarianism may be nearly twice as likely to suffer from depression as meat eaters, even after adjusting for variables like job status, family history and number of children.7
It’s widely known that people with a vitamin B12 deficiency are at an increased risk of depression,8which could be, in part, due to resulting alterations in the level of DNA methylation in the brain, leading to neurologic impairment.9 Vitamin B12 also helps regulate homocysteine levels, and increased homocysteine is linked to B12 deficiency as well as depression.
Folate, Vitamin B12 Suggested for Treatment of Depression
Considering the extensive research linking depression with low levels of vitamin B12 and folate, researchers with the MRC Neuropsychiatric Research Laboratory in Epsom, Surrey, U.K., suggested that folate and vitamin B12 should be considered in the treatment of depression.
“On the basis of current data, we suggest that oral doses of both folic acid (800 mcg daily) and vitamin B12 (1,000 mcg daily) should be tried to improve treatment outcome in depression,” they noted.10
Folic acid is the synthetic version of folate, or vitamin B9, and while it may have a place in depression treatment, the best way to increase your levels is to eat foods rich in folate, such as asparagus, avocados, Brussels sprouts, broccoli and spinach. As for why folate and vitamin B12 are so important for mental health, they explained:11
“Folate and vitamin B12 are major determinants of one-carbon metabolism, in which S-adenosylmethionine (SAM) is formed. SAM donates methyl groups that are crucial for neurological function. Increased plasma homocysteine is a functional marker of both folate and vitamin B12 deficiency. Increased homocysteine levels are found in depressive patients.”
Depressed Children Had ‘Remarkably High’ Homocysteine Levels
The connection between low vitamin B12 and increased homocysteine levels is notable, as the featured study found “remarkably high” homocysteine levels in the children and adolescents with depression.
“Increased homocysteine increases the flow of calcium within cells through the NMDA [N-methyl D-aspartic acid] receptor activation pathway. Within the cell, oxidative stress increases and apoptotic signals are activated. Increased homocysteine causes DNA damage, mitochondrial dysfunction, and endoplasmic reticulum stress,” the researchers noted, suggesting that this is likely one mechanism behind homocysteine’s depression connection.12
Separate research has also linked higher homocysteine levels with increased rates of depression and anxiety among 12- and 13-year-old boys in Taiwan.13 Higher levels of homocysteine, along with significantly lower levels of vitamin B12 and vitamin D, are also associated with other mental health conditions, including obsessive compulsive disorder, in which it’s believed to play a causative role.14
Homocysteine is an amino acid in your body and blood obtained primarily from meat consumption. Vitamins B6, B9 and B12 help convert homocysteine into methionine — a building block for proteins. If you don’t get enough of these B vitamins, this conversion process is impaired and results in higher homocysteine. Conversely, when you increase intake of B6, folate and B12, your homocysteine level decreases.
As such, checking your homocysteine level is a great way to identify a vitamin B6, folate and B12 deficiency. The researchers also noted that “vitamin deficiencies and elevated homocysteine should be investigated in terms of cause-effect relationships” in terms of depression in youth, especially since depression may contribute to poor appetite and irregular eating habits.
Vitamin D Levels Also Low Among Depressed Youth
The Ordu University researchers also found vitamin D levels to be low among the children and adolescents with depression, a connection that’s been revealed in the past. In the study, the depressed group had a median vitamin D level of 11 ng/ml, compared to 24.85 ng/ml in the control group. Both of these values are low, but 11 ng/ml is dangerously low and will radically increase the risk of rickets.
It’s important to note that for optimal health and disease prevention, a level between 60 and 80 ng/mL (150 to 200 nm/L) appears to be ideal, so all of the study participants were very low by this measure. Vitamin D receptors exist in the human brain,15 hinting at the importance of this vitamin in mental and emotional health.
It’s believed that vitamin D regulates more than 200 different genes by binding to vitamin D receptors that are responsible for driving a number of biological processes.16 Low levels of vitamin D have, in fact, been linked to a number of psychological disorders, including anxiety, depression and schizophrenia.
It likely influences psychological health in a number of ways, including by modulating inflammation, regulating proteins that fight free radicals and increasing the synthesis of brain-derived neurotrophic factor, which may play a role in schizophrenia.
Writing in the journal Children, Dr. Joy Weydert of the department of pediatrics at the University of Kansas Medical Center explained, “Vitamin D deficiency decreases the expression of the enzyme catechol-O-methyl transferase (COMT), required for dopamine and serotonin metabolism.”17 Further, adolescents with low levels of vitamin D had improved depressive symptoms after vitamin D supplementation.18
Vitamin D deficiency in children is “very common,”19 and children, like adults, should obtain regular sun exposure or take vitamin D3 supplements to ensure their levels are in the optimal range. It’s important to note that vitamin D supplementation must be balanced with other nutrients, namely vitamin K2 (to avoid complications associated with excessive calcification in your arteries), calcium and magnesium.
The best way to gauge whether you might need to supplement, and how much, is to get your level tested, ideally twice a year, in the early spring and early fall when your level is at its low point and peak. Optimizing vitamin D levels may be a simple way to significantly improve mental health. As noted in Issues in Mental Health Nursing:20
“Effective detection and treatment of inadequate vitamin D levels in persons with depression and other mental disorders may be an easy and cost-effective therapy which could improve patients’ long-term health outcomes as well as their quality of life.”
Once you have your vitamin D level tested you can use the Vitamin D Calculator developed by GrassRootsHealth to determine your ideal vitamin D dose.
Poor Diet Linked to Depression; Healthy Diet Fixes It
It’s been proven time and again that what you eat influences mental health, and this is certainly true among teenagers. Researchers at the University of Alabama at Birmingham looked into the role two dietary factors play in symptoms of depression among adolescents, in this case African-American teens who may be at an increased risk of both unhealthy diet and depression.
They analyzed the excretion of sodium and potassium in the urine in 84 urban, low‐income adolescents. Higher levels of sodium in the urine can be an indication of a diet high in sodium, such as processed fast foods and salty snacks. A low level of potassium, meanwhile, is indicative of a diet lacking in fruits, vegetables and other healthy potassium-rich foods.
As might be expected, higher sodium and lower potassium excretion rates were associated with more frequent symptoms of depression at follow up 1.5 years later.21 Past studies have also confirmed the diet-depression link among children and teens.
When researchers systematically reviewed 12 studies involving children and adolescents, an association was revealed between unhealthy diet and poorer mental health, as well as between a good-quality diet and better mental health.22
Likewise, researchers from Macquarie University, Australia, studied 76 students between the ages of 17 and 35 who followed a poor diet and had moderate to high levels of depression symptoms.23One group of the participants was asked to improve their diets by cutting back on refined carbohydrates, sugar, processed meats and soft drinks, while eating more vegetables, fruits, dairy products, nuts seeds, healthy fats and anti-inflammatory spices such as turmeric and cinnamon.24
After only three weeks of healthier eating, those in the healthy diet group had significant improvements in mood and their depression scores even went into the normal range. While teens and young adults aren’t always known for their healthy food choices, this is a crucial period in which lifelong healthy eating patterns are established.
Ensuring youth are eating healthy diets rich in folate and vitamin B12, as well as optimizing their vitamin D levels, may go a long way toward bolstering mental health and avoiding conditions like depression.
If a child or teen is already struggling with depression, eating real food is equally important. In addition to limiting the intake of processed foods, fast foods and sweets, including sugary beverages, increasing consumption of foods rich in omega-3 fats, such as sardines and wild-caught salmon, should be encouraged.
One pre-published study found a mismatch between the current flu vaccine and the main circulating strain, which may explain a recent flu outbreak on a college campus where the data suggested the vaccine was not effective
The argument to take the vaccine is that it may help reduce the severity of the illness. Yet, studies have demonstrated that seniors are not better protected, and the shot may only reduce the initial headache from flu
People who received the vaccine in 2008-2009 had a higher likelihood of contracting pandemic H1N1 in 2009; health experts believe this may repeat during the COVID pandemic as some have already found a positive association between COVID death and flu vaccination rates in the elderly
Experts believe, and data confirm, the research on flu vaccination is weak. Moderna and others are chasing larger returns as they plow ahead in human trials for an mRNA flu vaccine despite mounting adverse events
A search of the Vaccine Adverse Events Reporting System (VAERS) for 2019 using “flu” as the vax type and “influenza” as the vax name, recorded 12,061 adverse events following the influenza vaccine. In 2018, that number was 12,970.1
Despite what was considered a high number of adverse events in 2019, the effectiveness of the vaccine has been questionable. According to the Centers for Disease Control and Prevention:2
“While vaccine effectiveness (VE) can vary, recent studies show that flu vaccination reduces the risk of flu illness by between 40% and 60% among the overall population during seasons when most circulating flu viruses are well-matched to those used to make flu vaccines.”
In other words, only in years when the vaccine is well-matched to most circulating viruses will the shot afford protection for 40% to 60% of the overall population. This flu season doesn’t meet the criteria and so we can expect a low rate of protection in the overall population and possibly even lower in the elderly.
According to the National Foundation for Infectious Diseases,3 this is the very population that requires the best protection. Older adults are at higher risk of related complications and other flu-related risks, such as heart attack and stroke, which increase in the first two weeks after infection.4
This Year’s Flu Vaccine Doesn’t Match the Circulating Virus
Headlines in the news are calling this year’s flu shot a “mismatch” for the dominant strain,5 but continue to encourage adults and children to get a shot without also encouraging healthy behaviors. The information comes from a study6 co-written by Scott Hensley, professor of microbiology at the Perelman School of Medicine at the University of Pennsylvania.
The researchers wrote that although there may be a mismatch between the flu vaccine and the circulating H3N2 subtype of the influenza virus, “Studies have clearly shown that seasonal influenza vaccines consistently prevent hospitalizations and deaths even in years where there are large antigenic mismatches.”7
Hensley spoke with a reporter from CNN,8 sharing that they have been monitoring the H3N2 strain of flu for months, which is the main circulating strain. He believes this strain will evade the antibodies your body produces in response to the current vaccine.
In November 2021, there was an outbreak of flu at the University of Michigan, in which 700 people were affected and more than 26% who tested positive for flu had been vaccinated.9 Interestingly, this was the same percentage as those who tested negative, indicating the vaccine was not effective.
Hensley’s argument for taking the vaccine despite the mismatch is that while the vaccine does not generate the right antibodies for the new version of H3N2, the mismatch does not affect the second line of defense: your T cells. These are designed to help protect against severe disease.
One paper in 201610 outlined the importance of memory T-cells against the influenza virus and suggested the need for addressing this shortcoming in the flu vaccines. Two new approaches being researched at the time were infection permissive and recombinant T-cell inducing vaccines.
According to the CDC,11 82% of the 2021-2022 flu vaccine will be produced using egg-based manufacturing technology and the remaining 18% using recombinant and cell-based technology.
Mismatched Vaccine May Do Seniors More Harm Than Good
Despite assurances from the CDC that an annual flu shot is the best protection for seniors, there is a dismal history of effectiveness. After studies showed that protection in the elderly against mortality was low,12 the Flucelvax vaccine was introduced.13
It was promoted as an improved flu shot that would protect more people and yet, FDA research14showed no significant difference between this vaccine and a conventional flu shot in seniors. The overall effectiveness in preventing hospitalizations for flu shots in the study was 24% in people 65 and older, while the Flucelvax shot had an effectiveness rate of 26.5% in the same population.15
Health officials also frequently encourage flu vaccines to lessen the severity of disease, but a 2017 study found these claims were also not true.16 Analyzing data from vaccinated and unvaccinated seniors diagnosed with influenza, the researchers found only a reduction in initial headache complaints in those who had been vaccinated.
And yet the same researchers implausibly suggest that this very slight improvement in initial flu symptoms was enough to warrant the suggestion to “reinforce the need for influenza vaccines providing better protection.”17
Another systematic review and meta-analysis published in The Lancet Infectious Diseases similarly found “Evidence for protection [from influenza vaccines] in adults aged 65 years or older is lacking.”18
Will the Flu Vaccine Raise COVID-Related Deaths?
Questions arose after the 2009 mass vaccination campaign against H1N1 swine flu about whether seasonal influenza vaccinations may make pandemic infections worse or more prevalent.19 This same question has arisen during the COVID-19 pandemic.
A review of four studies published in 201020,21 showed that people who received the trivalent influenza vaccine during the 2008-2009 flu season were between 1.4 and 2.5 times more likely to get infected with pandemic H1N1 in the spring and summer of 2009 than those who did not get the seasonal flu vaccine.
In the early months of the COVID pandemic, Dr. Michael Murray, naturopath and author, agreed with what Judy Mikovitz, Ph.D., spoke with me about during one of our interviews22 — seasonal influenza vaccinations may have contributed to the dramatically elevated mortality from COVID-19 seen in Italy. In a blog post, Murray pointed out that Italy had introduced a new, more potent type of flu vaccine, called VIQCC, in September 2019:23
“Most available influenza vaccines are produced in embryonated chicken eggs. VIQCC, however, is produced from cultured animal cells rather than eggs and has more of a “boost” to the immune system as a result. VIQCC also contains four types of viruses – 2 type A viruses (H1N1 and H3N2) and 2 type B viruses.24
It looks like this “super” vaccine impacted the immune system in such a way to increase coronavirus infection through virus interference that set the stage for what happened in Italy.”
Cell-based technology flu vaccines, which are included in the 18% of vaccines distributed in the 2021-2022 season in the U.S., are cultured in animal cells.25 One study published in early 2020 in the journal Vaccine showed people were more likely to get some form of coronavirus infection if they had been vaccinated against influenza. The scientists wrote:26
“Receiving influenza vaccination may increase the risk of other respiratory viruses, a phenomenon known as virus interference … Examining virus interference by specific respiratory viruses showed mixed results. Vaccine derived virus interference was significantly associated with coronavirus and human metapneumovirus.”
October 1, 2020, Christian Wehenkel, an academic editor for PeerJ, published a data analysis27 in which he reported finding a “positive association between COVID-19 deaths and influenza vaccination rates in elderly people worldwide.” In other words, areas with the highest flu vaccination rates among elderly people also had the highest COVID-19 death rates. To be fair, the publisher noted that correlation does not necessarily equal causation.
That said, one of the reasons for the analysis was to double-check whether the data would support claims that seasonal influenza vaccination was negatively correlated with COVID-19 mortality — including one that found regions in Italy with higher vaccination rates among elders had lower COVID-19 death rates.28 “A negative association was expected,” Wehenkel writes in PeerJ. But that’s not what he found:29
“Contrary to expectations, the present worldwide analysis and European sub-analysis do not support the previously reported negative association between COVID-19 deaths (DPMI) [COVID-19 deaths per million inhabitants] and IVR [influenza vaccination rate] in elderly people, observed in studies in Brazil and Italy …
The results showed a positive association between COVID-19 deaths and IVR of people ≥65 years-old. There is a significant increase in COVID-19 deaths from eastern to western regions in the world. Further exploration is needed to explain these findings, and additional work on this line of research may lead to prevention of deaths associated with COVID-19.”
Co-Founder of Cochrane Finds Flu Research Weak
Professor Peter Gøtzsche is a Danish physician-researcher who co-founded the Cochrane Collaboration in 1993 and later launched the Nordic Cochrane Centre. He has been an outspoken critic of conflicts of interest and bias in research.
In a February 9, 2020, tweet,30 Gøtzsche wrote: “Cochrane corruption. A Cochrane review did not find that flu shots reduce deaths … ‘After invitation from Cochrane,’ a financially conflicted person ‘re-arranged’ the data and vaccines reduced deaths. They don’t …”
Indeed, in past years, Cochrane has repeatedly found flu vaccinations are ineffective and have no appreciable effect on influenza-related hospitalizations and mortality. For example:
• A 2006 systematic review31 of 51 studies analyzing the effectiveness of the shot in children found a 33% effectiveness in children using live vaccines and 36% using inactivated vaccines.
• A 2010 Cochrane review32 of 50 influenza studies found “In the relatively uncommon circumstance of vaccine matching the viral circulating strain and high circulation, 4% of unvaccinated people versus 1% of vaccinated people developed influenza symptoms … Vaccination had a modest effect on time off work and had no effect on hospital admissions …”
• A 2010 Cochrane review33 of 75 studies analyzing the effectiveness of preventing influenza in the elderly found the studies were generally of low quality and there was a “likely presence of biases” making any firm conclusions possibly misleading.
• In a 2018 Cochrane review34 of 41 clinical trials on live and inactivated flu vaccines in children they found for live attenuated vaccines, “Seven children would need to be vaccinated to prevent one case of influenza, and 20 children would need to be vaccinated to prevent one child experiencing an ILI [influenza-like illness] …”
Children vaccinated with inactivated vaccines showed “Five children would need to be vaccinated to prevent one case of influenza, and 12 children would need to be vaccinated to avoid one case of ILI.”
Moderna Racing for mRNA Flu Vaccine
Despite not knowing the long-term effects of mRNA vaccines and the mounting evidence of adverse events occurring within the first six months of the COVID mRNA injection, there are several genetic therapy shots in the pipeline. One of those is a seasonal flu vaccine produced by Moderna, which has already entered Phase 1 human trials. July 7, 2021, The Verge reported:35
“Moderna gave its mRNA-based seasonal flu vaccine to the first set of volunteers in a clinical trial. … Moderna is the second group to start testing its mRNA flu shot in human trials — Sanofi and Translate Bio kicked off a trial this summer. Pfizer and BioNTech have been interested in mRNA flu shots for a few years, and they’re pushing forward with those plans as well.”
Six months later, Moderna has announced the initial data from the Phase I trials are showing positive results and boosting “the immune response against all targeted flu strains 29 days after administration.”36
In true warp-speed action, Moderna announced they have already fully enrolled their Phase II human clinical trial for this mRNA flu vaccine before the Phase I trial has been completed. In addition, they are preparing for a Phase III study, assuming the data — produced by the pharmaceutical company that owns the rights to the flu vaccine — will be positive.
Human clinical trials are split into three phases to protect the participants as much as possible.37Phase I is primarily aimed at establishing the safety and dose range using a small number of healthy volunteers. These studies often involve risk as they are the first time the drug has been administered to a human.
Phase II studies look at the effectiveness of the drug against a particular condition and can last up to two years. The secondary objective is to determine the therapeutic dose level and frequency. According to the University of Cincinnati College of Medicine,38 roughly 33% of drugs that pass Phase I and Phase II will go on to Phase III.
Phase III studies should occur over multiple centers and enroll up to several thousand patients. In this phase, the drug can be studied for several years and roughly 25 to 30% of these drugs may pass Phase III trials. Moderna is confident the data from the trial they are sponsoring will sail over these hurdles.
Big Pharma and vaccine stakeholders advise you to take every shot possible without concern for your health and safety. Despite a growing number of adverse events being reported39 — including death — from a new technology genetic therapy injection, pharmaceutical companies are plowing ahead in human trials to create yet another mRNA vaccine as they chase larger quarterly returns.
In a horrifying altercation, a German police officer denounced the humanity of the unvaccinated. This is but one sign that mass formation psychosis is at work
“Mass formation psychosis” is the explanation for how the Germans accepted the atrocities by the Nazi party in the 1930s, and it’s the explanation for why so many around the world support medical apartheid and the dehumanization of the unvaccinated now
The stigmatization of the unvaxxed is all the more irrational when you consider that the COVID shot doesn’t prevent infection or spread of the virus. “Fully vaxxed” individuals are just as infectious and “dangerous” as the unjabbed
While high-level officials continue to use the term “pandemic of the unvaccinated,” suggesting the COVID-jabbed play no role in the epidemiology of COVID-19, there’s ample evidence that the “fully vaccinated” have a relevant role in transmission and outbreaks
For example, in Massachusetts, 469 new COVID-19 cases were identified during July 2021. Of those, 346 (74%) were either fully or partially jabbed, and 274 (79%) were symptomatic. This proves the COVID jabs cannot end the pandemic, and may in fact be preventing it from dying out naturally
GERMAN HATE AND STUPIDITY
GERMANY 2021: A police officer calls unvaccinated people indirect killers and says they are not human.
You know you’ve entered a twilight zone of insanity when a police officer tells you you’re a criminal simply because you’re unvaccinated. That’s exactly what happened the other day in Germany. The police officer insisted the unvaccinated man was “a murderer” because he “might infect someone,” and that he’s “not a human.”
The bizarre altercation was posted on Twitter December 12, 2021, (see above). In response, the unvaccinated man tells the cop he’s the one who has “lost all humanity.” Indeed. Who thought we’d ever see the day when individuals are marked as “murderers” and “not human” based on vaccination status alone?
It’s beyond irrational. But then again, insanity does not obey reason, and according to professor Mattias Desmet, a Belgian psychologist, the world has indeed been hypnotized into a state of mass psychosis.1
“Mass formation psychosis” is the explanation for how the Germans accepted the atrocities by the Nazi party in the 1930s, and it’s the explanation for why so many around the world support medical apartheid and the dehumanization of the unvaccinated now.
You Cannot Comply Your Way Out of Tyranny
The stigmatization and dehumanization of the unvaxxed is all the more irrational when you consider that the COVID shot doesn’t prevent infection or spread of the virus. Those who have received one, two or even three doses are STILL contracting the infection, and at ever-increasing rates, and are spreading it to vaxxed and unvaxxed alike.
Outbreaks among “fully vaccinated” populations, isolated on cruise ships, for example, have occurred on several occasions, proving the shots fail to prevent outbreaks. The COVID-jabbed are clearly just as “dangerous” and likely to “kill” their fellow man as those who are unjabbed.
When either decision — the decision to get the jab or decline it — results in you posing the exact same level of risk to others, how can anyone say that one is more dangerous than the other? Anyone still capable of clear, level-headed thinking will see that it doesn’t add up.
Unfortunately, most countries are experiencing a mass delusional psychosis. They have been manipulated into believing highly irrational absurdities. The same psychological operation was at work in the 1930s, when Jews, the old and infirm, and the mentally and physically handicapped were dehumanized and blamed as carriers of disease and other social ills.
In the short video above, Auschwitz survivor Marian Turski, now 94 years old, describes the incremental dehumanization and ostracizing that took place in Nazi Germany, ultimately ending in the Holocaust. Now, we stand before the same fork in the road yet again. Many, like the German police officer, are choosing the well-trodden road of repeated history.
Stigmatizing Unvaccinated Is Unjustified
November 20, 2021, The Lancet published a letter by Gunter Kampf, titled “COVID-19: Stigmatizing the Unvaccinated Is Not Justified.”2 “In the USA and Germany, high-level officials have used the term pandemic of the unvaccinated, suggesting that people who have been vaccinated are not relevant in the epidemiology of COVID-19,” Kampf writes.
However, he adds, “There is increasing evidence that vaccinated individuals continue to have a relevant role in transmission.” He goes on to cite statistics from Massachusetts, where 469 new COVID-19 cases were identified during July 2021. Of those, 346 (74%) were either fully or partially jabbed, and 274 (79%) were symptomatic.
The cycle threshold values used during PCR testing were also similarly low regardless of COVID jab status (median 22.8 cycles, which minimizes the risk of false positive results), “indicating a high viral load even among people who were fully vaccinated,” Kampf notes. These data are clear evidence that the COVID jabs cannot end the pandemic, and may in fact be preventing it from dying out naturally. Kampf continues:3
“In the USA, a total of 10,262 COVID-19 cases were reported in vaccinated people by April 30, 2021, of whom 2725 (26.6%) were asymptomatic, 995 (9.7%) were hospitalized, and 160 (1.6%) died. In Germany, 55.4% of symptomatic COVID-19 cases in patients aged 60 years or older were in fully vaccinated individuals, and this proportion is increasing each week.
In Münster, Germany, new cases of COVID-19 occurred in at least 85 (22%) of 380 people who were fully vaccinated or who had recovered from COVID-19 and who attended a nightclub.
People who are vaccinated have a lower risk of severe disease but are still a relevant part of the pandemic. It is therefore wrong and dangerous to speak of a pandemic of the unvaccinated.
Historically, both the USA and Germany have engendered negative experiences by stigmatizing parts of the population for their skin color or religion.
I call on high-level officials and scientists to stop the inappropriate stigmatization of unvaccinated people, who include our patients, colleagues, and other fellow citizens, and to put extra effort into bringing society together.”
Human Today, Not Human Tomorrow
It’s important to realize you cannot comply your way out of this tyranny. If you choose to get the COVID shot because you don’t want to be stigmatized, there can be no end to your compliance to future boosters, no matter what the cost to you or your family.
In short order — a handful of months at most — you will suddenly and arbitrarily be deemed an unvaccinated menace to society again, even though you’ve already had one, two or three kill shots.
None of that will matter. You get no brownie points for past compliance. At six months past your second or third dose, your status will go from green to red, from human to not human, literally overnight. You’re “unvaccinated” again, until or unless you get another booster. This cycle will continue until you’re dead. Are you game? Is that how you want to spend the rest of your life?
COVID Shots Keep the ‘Pandemic’ Going
More than 80 studies have confirmed that natural immunity to COVID-19 is equal or superior to what you get from the jab.4 This conforms to well-established medical science, so it’s no surprise. It’s as it should be.
But for the first time in modern medical history, natural immunity is being portrayed as having no benefit whatsoever. Even worse, those with natural immunity are being labeled as dangerous and are shunned and even fired from their jobs for failing to get a shot.
Only the jabbed are protected and can protect others, health authorities now claim — even though it’s those with natural immunity who are most protected and don’t pose a risk to others.
The reality and truth, though, is that natural immunity is long-lasting, protects against all variants and will not contribute to the creation of variants. The same cannot be said for the COVID jab. We now have clear evidence the shots offer, at most, six months’ worth of protection, after which the relative risk reduction drops to zero.
As just one example among many, a Swedish study5 published October 25, 2021, found that while the jabs initially lowered the risk of hospitalization, their effectiveness rapidly waned.
The Pfizer jab went from 92% effectiveness at Day 15 through 30, to 47% at Day 121 through 180, and zero from Day 201 onward.
The Moderna shot had a similar trajectory, being estimated at 59% from Day 181 onward.
The AstraZeneca injection had a lower effectiveness out of the gate, waned faster than the mRNA shots, and had no detectable effectiveness as of Day 121.
This and other studies showing waning immunity were discussed in a December 9, 2021, New England Journal of Medicine interview.6 As noted in that interview, the Delta variant, which is significantly different from the initial SARS-CoV-2 strain, can infect fully jabbed individuals, and its ability to do so increases over time, as the effectiveness of the shot rapidly wanes.
Aside from waning efficacy, the fact that the virus is mutating within “vaccinated” populations also forces it to develop the capacity to circumvent the COVID jab. In short, the deck is stacked against those who rely on the COVID shot to protect them. In the long term, it’s a hopeless situation, as we cannot inoculate our way out of an endemic with a product that doesn’t prevent infection and spread!
Sadly, NEJM, rather than promoting science, toes the line of the official mainstream narrative and suggest boosters are the answer. They should know better, which raises suspicions that conflicts of interest likely impact their clinical judgment.7
Lindsey Baden, one of the interviewees, has received grants from the National Institutes of Health, the Gates Foundation and the Wellcome Trust — three institutions that more or less openly support medical tyranny and totalitarian rule by a biosecurity-based police state.
The Gravity of Our Situation
Auschwitz survivor Marian Turski, 94: "And that's how it is done, step by step, slowly." pic.twitter.com/ewla4GCjeu
Natural News) The U.S. Centers for Disease Control and IMG_4544Prevention (CDC) is finally admitting that PCR tests have no place in trying to detect the presence of the Wuhan coronavirus (Covid-19) inside a person’s body.
Rochelle Walensky, the fake federal agency’s top dog, told ABC News in a recent interview that the “new science” shows that PCR tests do not work, and the government is no longer using them.
“With all of that science together, we moved forward with isolation recommendations of five days of isolation followed by five days in a mask,” Walensky explained about the new guidelines (watch the interview below).
“Now the question of why we didn’t include a test there is simply because we know that PCRs can stay positive for up to 12 weeks. So we would have people in isolation for a very long time if we were relying on PCRs.”
Does Rochelle Walensky ever tell the truth?
It was already revealed previously in documents straight from the U.S. Food and Drug Administration (FDA) that PCR tests were developed without any isolated Fauci Flu samples because none exist.
Instead, the FDA used ordinary influenza to “calibrate” the tests, which we now know produce an exceptional number of false positives.
It took the CDC a very long time to catch up with the latest science, though. Walensky herself has been pushing lies for many months now about how the “data” (based on false PCR test results) suggests that people need to get “vaccinated” and “boosted” in haste in order to stop the plandemic.
100% organic essential oil sets now available for your home and personal care, including Rosemary, Oregano, Eucalyptus, Tea Tree, Clary Sage and more, all 100% organic and laboratory tested for safety. A multitude of uses, from stress reduction to topical first aid. See the complete listing here, and help support this news site.
Back in September, Walensky actually admitted that her guidance on getting boosted is based on “hope” rather than data.
“So, there’s actually hope – we don’t have data yet,” Walensky told “TODAY” host Savannah Guthrie.
“We do know that the higher levels of protection certainly in the alpha variant resulted in less transmission and we have not yet seen the data, but we are hopeful that the booster will not only protect you, give you a higher level of protection, not just against the delta variant but against a broad range of variants. It might also decrease the level of virus that you have and make it less transmissible.”
Now, a full year-and-a-half after the rest of world figured out that PCR tests are fraudulent, Walensky is finally fessing up to the truth about that as well. The question is: Will the Branch Covidians listen or will they continue to get “tested” in perpetual panic while wearing a mask and getting boosted every time Walensky tells them to?
“And yet companies and government agencies still roll right along saying jab or weekly test, don’t they?” asked one upset commenter about how PCR testing will probably continue regardless of this latest admission by Walensky.
“When do the trials for treason begin?” asked another.
“No wonder covid is on the rise,” wrote another, suggesting that the only reason we still have “cases” is because of fraudulent PCR test results. “And the government plans on sending out tests to everyone? We will lock down again for sure. Follow the science? Yeah right.”
Another wrote that the silver lining in all of this is that it might finally become widely known through all of this that the “clot shots” do not work and are only fueling the plandemic, preventing it from ever ending.
The latest news about Chinese Germs can be found at Pandemic.news.
Over 1000 scientific studies and/or reports on the dangers associated with COVID injections related to blood clotting, myocarditis, pericarditis, thrombosis, thrombocytopenia, anaphylaxis, Bell’s palsy, Guillain-Barre, deaths, etc. and 100+ References at the bottom.
US case reports of cerebral venous sinus thrombosis with thrombocytopenia after vaccination with Ad26.COV2.S (against covid-19), March 2 to April 21, 2020: https://pubmed.ncbi.nlm.nih.gov/33929487/
Management of cerebral and splanchnic vein thrombosis associated with thrombocytopenia in subjects previously vaccinated with Vaxzevria (AstraZeneca): position statement of the Italian Society for the Study of Hemostasis and Thrombosis (SISET): https://pubmed.ncbi.nlm.nih.gov/33871350/
Myocarditis after immunization with COVID-19 mRNA vaccines in members of the US military. This article reports that in “23 male patients, including 22 previously healthy military members, myocarditis was identified within 4 days after receipt of the vaccine”: https://jamanetwork.com/journals/jamacardiology/fullarticle/2781601
Pathological antibodies against platelet factor 4 after vaccination with ChAdOx1 nCoV-19. This article states: “In the absence of previous prothrombotic medical conditions, 22 patients had acute thrombocytopenia and thrombosis, mainly cerebral venous thrombosis, and 1 patient had isolated thrombocytopenia and a hemorrhagic phenotype”: https://www.nejm.org/doi/full/10.1056/NEJMoa2105385?query=TOC&fbclid=IwA R2ifm2TQjetAMb42YRRUlKEeqCQe-lDasIWvjMgzHHaItbuPbu6n7NlG3cic.
Cerebral venous sinus thrombosis negative for anti-PF4 antibody without thrombocytopenia after immunization with COVID-19 vaccine in a non-comorbid elderly Indian male treated with conventional heparin-warfarin based anticoagulation: https://www.sciencedirect.com/science/article/pii/S1871402121002046
Acute myocardial injury after COVID-19 vaccination: a case report and review of current evidence from the Vaccine Adverse Event Reporting System database: https://pubmed.ncbi.nlm.nih.gov/34219532/
Occurrence of acute infarct-like myocarditis after COVID-19 vaccination: just an accidental coincidence or rather a vaccination-associated autoimmune myocarditis?: https://pubmed.ncbi.nlm.nih.gov/34333695/
Self-limited myocarditis presenting with chest pain and ST-segment elevation in adolescents after vaccination with the BNT162b2 mRNA vaccine: https://pubmed.ncbi.nlm.nih.gov/34180390/
Insights from a murine model of COVID-19 mRNA vaccine-induced myopericarditis: could accidental intravenous injection of a vaccine induce myopericarditis?
Bell’s palsy after the second dose of the Pfizer COVID-19 vaccine in a patient with a history of recurrent Bell’s palsy: bhttps://www.sciencedirect.com/science/article/pii/S266635462100020X
Cerebral venous sinus thrombosis negative for anti-PF4 antibody without thrombocytopenia after immunization with COVID-19 vaccine in an elderly, non-comorbid Indian male treated with conventional heparin-warfarin-based anticoagulation:. https://www.sciencedirect.com/science/article/pii/S1871402121002046.
Allergic reactions, including anaphylaxis, after receiving the first dose of Pfizer-BioNTech COVID-19 vaccine – United States, December 14-23, 2020: https://pubmed.ncbi.nlm.nih.gov/33444297/
Allergic reactions, including anaphylaxis, after receiving first dose of Modern COVID-19 vaccine – United States, December 21, 2020-January 10, 2021: https://pubmed.ncbi.nlm.nih.gov/33507892/
Severe Allergic Reactions after COVID-19 Vaccination with the Pfizer / BioNTech Vaccine in Great Britain and the USA: Position Statement of the German Allergy Societies: German Medical Association of Allergologists (AeDA), German Society for Allergology and Clinical Immunology (DGAKI) and Society for Pediatric Allergology and Environmental Medicine (GPA): https://pubmed.ncbi.nlm.nih.gov/33643776/
Cumulative adverse event report of anaphylaxis following injections of COVID-19 mRNA vaccine (Pfizer-BioNTech) in Japan: the first month report: https://pubmed.ncbi.nlm.nih.gov/34347278/
Allergenic components of the mRNA-1273 vaccine for COVID-19: possible involvement of polyethylene glycol and IgG-mediated complement activation: https://pubmed.ncbi.nlm.nih.gov/33657648/
Polyethylene glycole allergy of the SARS CoV2 vaccine recipient: case report of a young adult recipient and management of future exposure to SARS-CoV2: https://pubmed.ncbi.nlm.nih.gov/33919151/
Elevated rates of anaphylaxis after vaccination with Pfizer BNT162b2 mRNA vaccine against COVID-19 in Japanese healthcare workers; a secondary analysis of initial post-approval safety data: https://pubmed.ncbi.nlm.nih.gov/34128049/
Risk of severe allergic reactions to COVID-19 vaccines among patients with allergic skin disease: practical recommendations. An ETFAD position statement with external experts: https://pubmed.ncbi.nlm.nih.gov/33752263/
Varicella zoster virus and herpes simplex virus reactivation after vaccination with COVID-19: review of 40 cases in an international dermatologic registry: https://pubmed.ncbi.nlm.nih.gov/34487581/
Immune thrombosis and thrombocytopenia (VITT) associated with the COVID-19 vaccine: diagnostic and therapeutic recommendations for a new syndrome: https://pubmed.ncbi.nlm.nih.gov/33987882/
Intracerebral hemorrhage due to thrombosis with thrombocytopenia syndrome after COVID-19 vaccination: the first fatal case in Korea: https://pubmed.ncbi.nlm.nih.gov/34402235/
Risk of thrombocytopenia and thromboembolism after covid-19 vaccination and positive SARS-CoV-2 tests: self-controlled case series study: https://pubmed.ncbi.nlm.nih.gov/34446426/
Vaccine-induced immune thrombotic thrombocytopenia and cerebral venous sinus thrombosis after covid-19 vaccination; a systematic review: https://pubmed.ncbi.nlm.nih.gov/34365148/.
Nerve and muscle adverse events after vaccination with COVID-19: a systematic review and meta-analysis of clinical trials: https://pubmed.ncbi.nlm.nih.gov/34452064/.
A rare case of cerebral venous thrombosis and disseminated intravascular coagulation temporally associated with administration of COVID-19 vaccine: https://pubmed.ncbi.nlm.nih.gov/33917902/
Primary adrenal insufficiency associated with thrombotic immune thrombocytopenia induced by Oxford-AstraZeneca ChAdOx1 nCoV-19 vaccine (VITT): https://pubmed.ncbi.nlm.nih.gov/34256983/
Thromboaspiration infusion and fibrinolysis for portomesenteric thrombosis after administration of AstraZeneca COVID-19 vaccine: https://pubmed.ncbi.nlm.nih.gov/34132839/
59-year-old woman with extensive deep venous thrombosis and pulmonary thromboembolism 7 days after a first dose of Pfizer-BioNTech BNT162b2 mRNA vaccine COVID-19: https://pubmed.ncbi.nlm.nih.gov/34117206/
Cerebral venous thrombosis and vaccine-induced thrombocytopenia.
Insights from a murine model of myopericarditis induced by COVID-19 mRNA vaccine: could accidental intravenous injection of a vaccine induce myopericarditis: https://pubmed.ncbi.nlm.nih.gov/34453510/
Thrombosis with thrombocytopenia syndrome (TTS) following AstraZeneca ChAdOx1 nCoV-19 (AZD1222) COVID-19 vaccination: risk-benefit analysis for persons <60 years in Australia: https://pubmed.ncbi.nlm.nih.gov/34272095/
Transient oculomotor paralysis after administration of RNA-1273 messenger vaccine for SARS-CoV-2 diplopia after COVID-19 vaccine: https://pubmed.ncbi.nlm.nih.gov/34369471/
Parsonage-Turner syndrome associated with SARS-CoV-2 or SARS-CoV-2 vaccination. Comment on: “Neuralgic amyotrophy and COVID-19 infection: 2 cases of accessory spinal nerve palsy” by Coll et al. Articular Spine 2021; 88: 10519: https://pubmed.ncbi.nlm.nih.gov/34139321/.
Acute autoimmune-like hepatitis with atypical antimitochondrial antibody after vaccination with COVID-19 mRNA: a new clinical entity: https://pubmed.ncbi.nlm.nih.gov/34293683/.
Bilateral superior ophthalmic vein thrombosis, ischemic stroke and immune thrombocytopenia after vaccination with ChAdOx1 nCoV-19: https://pubmed.ncbi.nlm.nih.gov/33864750/
Diagnosis and treatment of cerebral venous sinus thrombosis with vaccine-induced immune-immune thrombotic thrombocytopenia: https://pubmed.ncbi.nlm.nih.gov/33914590/
Cerebral venous sinus thrombosis following vaccination against SARS-CoV-2: an analysis of cases reported to the European Medicines Agency: https://pubmed.ncbi.nlm.nih.gov/34293217/
Risk of thrombocytopenia and thromboembolism after covid-19 vaccination and positive SARS-CoV-2 tests: self-controlled case series study: https://pubmed.ncbi.nlm.nih.gov/34446426/
Arterial events, venous thromboembolism, thrombocytopenia and bleeding after vaccination with Oxford-AstraZeneca ChAdOx1-S in Denmark and Norway: population-based cohort study: https://pubmed.ncbi.nlm.nih.gov/33952445/
First dose of ChAdOx1 and BNT162b2 COVID-19 vaccines and thrombocytopenic, thromboembolic and hemorrhagic events in Scotland: https://pubmed.ncbi.nlm.nih.gov/34108714/
Malignant cerebral infarction after vaccination with ChAdOx1 nCov-19: a catastrophic variant of vaccine-induced immune-mediated thrombotic thrombocytopenia: https://pubmed.ncbi.nlm.nih.gov/34341358/
celiac artery and splenic artery thrombosis complicated by splenic infarction 7 days after the first dose of Oxford vaccine, causal relationship or coincidence: https://pubmed.ncbi.nlm.nih.gov/34261633/.
central venous sinus thrombosis with subarachnoid hemorrhage after COVID-19 mRNA vaccination: are these reports merely coincidental: https://pubmed.ncbi.nlm.nih.gov/34478433/
Intracerebral hemorrhage due to thrombosis with thrombocytopenia syndrome after COVID-19 vaccination: the first fatal case in Korea: https://pubmed.ncbi.nlm.nih.gov/34402235/
Cerebral venous sinus thrombosis negative for anti-PF4 antibody without thrombocytopenia after immunization with COVID-19 vaccine in a non-comorbid elderly Indian male treated with conventional heparin-warfarin-based anticoagulation: https://pubmed.ncbi.nlm.nih.gov/34186376/ 263.
Vaccine-induced thrombotic thrombocytopenia: the elusive link between thrombosis and adenovirus-based SARS-CoV-2 vaccines: https://pubmed.ncbi.nlm.nih.gov/34191218/ 266.
Acute ischemic stroke revealing immune thrombotic thrombocytopenia induced by ChAdOx1 nCov-19 vaccine: impact on recanalization strategy: https://pubmed.ncbi.nlm.nih.gov/34175640/
Thromboaspiration infusion and fibrinolysis for portomesenteric thrombosis after administration of the AstraZeneca COVID-19 vaccine: https://pubmed.ncbi.nlm.nih.gov/34132839/.
Spontaneous HIT syndrome: knee replacement, infection, and parallels with vaccine-induced immune thrombotic thrombocytopenia: https://pubmed.ncbi.nlm.nih.gov/34144250/
Procoagulant antibody-mediated procoagulant platelets in immune thrombotic thrombocytopenia associated with SARS-CoV-2 vaccination: https://pubmed.ncbi.nlm.nih.gov/34011137/.
Vaccine-induced immune thrombotic thrombocytopenia causing a severe form of cerebral venous thrombosis with high mortality rate: a case series: https://pubmed.ncbi.nlm.nih.gov/34393988/.
Procoagulant microparticles: a possible link between vaccine-induced immune thrombocytopenia (VITT) and cerebral sinus venous thrombosis: https://pubmed.ncbi.nlm.nih.gov/34129181/.
Atypical thrombosis associated with the vaccine VaxZevria® (AstraZeneca): data from the French network of regional pharmacovigilance centers: https://pubmed.ncbi.nlm.nih.gov/34083026/.
Comparison of adverse drug reactions among four COVID-19 vaccines in Europe using the EudraVigilance database: Thrombosis in unusual sites: https://pubmed.ncbi.nlm.nih.gov/34375510/
Severe vaccine-induced thrombotic thrombocytopenia following vaccination with COVID-19: an autopsy case report and review of the literature: https://pubmed.ncbi.nlm.nih.gov/34355379/.
fulminant myocarditis and systemic hyperinflammation temporally associated with BNT162b2 COVID-19 mRNA vaccination in two patients: https://pubmed.ncbi.nlm.nih.gov/34416319/.
Adverse effects reported after COVID-19 vaccination in a tertiary care hospital, centered on cerebral venous sinus thrombosis (CVST): https://pubmed.ncbi.nlm.nih.gov/34092166/
Induction and exacerbation of subacute cutaneous lupus erythematosus erythematosus after mRNA- or adenoviral vector-based SARS-CoV-2 vaccination: https://pubmed.ncbi.nlm.nih.gov/34291477/
Platelet activation and modulation in thrombosis with thrombocytopenia syndrome associated with the ChAdO × 1 nCov-19 vaccine: https://pubmed.ncbi.nlm.nih.gov/34474550/
Acute relapse and impaired immunization after COVID-19 vaccination in a patient with multiple sclerosis treated with rituximab: https://pubmed.ncbi.nlm.nih.gov/34015240/
Transient thrombocytopenia with glycoprotein-specific platelet autoantibodies after vaccination with Ad26.COV2.S: case report: https://pubmed.ncbi.nlm.nih.gov/34516272/.
Acute hyperactive encephalopathy following COVID-19 vaccination with dramatic response to methylprednisolone: case report: https://pubmed.ncbi.nlm.nih.gov/34512961/
Onset / outbreak of psoriasis after Corona virus ChAdOx1 nCoV-19 vaccine (Oxford-AstraZeneca / Covishield): report of two cases: https://pubmed.ncbi.nlm.nih.gov/34350668/
COVID-19 vaccine, immune thrombotic thrombocytopenia, jaundice, hyperviscosity: concern in cases with underlying hepatic problems: https://pubmed.ncbi.nlm.nih.gov/34509271/.
Report of the International Cerebral Venous Thrombosis Consortium on cerebral venous thrombosis after SARS-CoV-2 vaccination: https://pubmed.ncbi.nlm.nih.gov/34462996/
COVID-19: lessons from the Norwegian tragedy should be taken into account in planning for vaccine launch in less developed/developing countries: https://pubmed.ncbi.nlm.nih.gov/34435142/
Cerebral venous sinus thrombosis and thrombocytopenia after COVID-19 vaccination: report of two cases in the United Kingdom: https://pubmed.ncbi.nlm.nih.gov/33857630/.
Cerebral venous thrombosis after COVID-19 vaccination: is the risk of thrombosis increased by intravascular administration of the vaccine: https://pubmed.ncbi.nlm.nih.gov/34286453/.
Central venous sinus thrombosis with subarachnoid hemorrhage after COVID-19 mRNA vaccination: are these reports merely coincidental: https://pubmed.ncbi.nlm.nih.gov/34478433/
Early results of bivalirudin treatment for thrombotic thrombocytopenia and cerebral venous sinus thrombosis after vaccination with Ad26.COV2.S: https://pubmed.ncbi.nlm.nih.gov/34226070/
Vaccine-induced immune thrombotic thrombocytopenia causing a severe form of cerebral venous thrombosis with a high mortality rate: a case series: https://pubmed.ncbi.nlm.nih.gov/34393988/.
Adenovirus interactions with platelets and coagulation and vaccine-associated autoimmune thrombocytopenia thrombosis syndrome: https://pubmed.ncbi.nlm.nih.gov/34407607/.
Headache attributed to COVID-19 (SARS-CoV-2 coronavirus) vaccination with the ChAdOx1 nCoV-19 (AZD1222) vaccine: a multicenter observational cohort study: https://pubmed.ncbi.nlm.nih.gov/34313952/
Adverse effects reported after COVID-19 vaccination in a tertiary care hospital, focus on cerebral venous sinus thrombosis (CVST): https://pubmed.ncbi.nlm.nih.gov/34092166/
Cerebral venous sinus thrombosis following vaccination against SARS-CoV-2: an analysis of cases reported to the European Medicines Agency: https://pubmed.ncbi.nlm.nih.gov/34293217/
Cerebral venous sinus thrombosis negative for anti-PF4 antibody without thrombocytopenia after immunization with COVID-19 vaccine in a non-comorbid elderly Indian male treated with conventional heparin-warfarin-based anticoagulation: https://pubmed.ncbi.nlm.nih.gov/34186376/
Arterial events, venous thromboembolism, thrombocytopenia and bleeding after vaccination with Oxford-AstraZeneca ChAdOx1-S in Denmark and Norway: population-based cohort study: https://pubmed.ncbi.nlm.nih.gov/33952445/
Procoagulant microparticles: a possible link between vaccine-induced immune thrombocytopenia (VITT) and cerebral sinus venous thrombosis: https://pubmed.ncbi.nlm.nih.gov/34129181/
U.S. case reports of cerebral venous sinus thrombosis with thrombocytopenia after vaccination with Ad26.COV2.S, March 2-April 21, 2021: https://pubmed.ncbi.nlm.nih.gov/33929487/.
Malignant cerebral infarction after vaccination with ChAdOx1 nCov-19: a catastrophic variant of vaccine-induced immune-mediated thrombotic thrombocytopenia: https://pubmed.ncbi.nlm.nih.gov/34341358/
Acute ischemic stroke revealing immune thrombotic thrombocytopenia induced by ChAdOx1 nCov-19 vaccine: impact on recanalization strategy: https://pubmed.ncbi.nlm.nih.gov/34175640/
Vaccine-induced immune thrombotic immune thrombocytopenia (VITT): a new clinicopathologic entity with heterogeneous clinical presentations: https://pubmed.ncbi.nlm.nih.gov/34159588/.
Australian and New Zealand approach to the diagnosis and treatment of vaccine-induced immune thrombosis and immune thrombocytopenia: https://pubmed.ncbi.nlm.nih.gov/34490632/
An observational study to identify the prevalence of thrombocytopenia and anti-PF4 / polyanion antibodies in Norwegian health care workers after COVID-19 vaccination: https://pubmed.ncbi.nlm.nih.gov/33909350/
Acute transverse myelitis (ATM): clinical review of 43 patients with COVID-19-associated ATM and 3 serious adverse events of post-vaccination ATM with ChAdOx1 nCoV-19 (AZD1222) vaccine: https://pubmed.ncbi.nlm.nih.gov/33981305/.
Thrombocytopenia with acute ischemic stroke and hemorrhage in a patient recently vaccinated with an adenoviral vector-based COVID-19 vaccine:. https://pubmed.ncbi.nlm.nih.gov/33877737/
First dose of ChAdOx1 and BNT162b2 COVID-19 vaccines and thrombocytopenic, thromboembolic, and hemorrhagic events in Scotland: https://pubmed.ncbi.nlm.nih.gov/34108714/
ChAdOx1 nCoV-19 vaccine-associated thrombocytopenia: three cases of immune thrombocytopenia after 107,720 doses of ChAdOx1 vaccination in Thailand: https://pubmed.ncbi.nlm.nih.gov/34483267/.
Neurosurgical considerations with respect to decompressive craniectomy for intracerebral hemorrhage after SARS-CoV-2 vaccination in vaccine-induced thrombotic thrombocytopenia-VITT: https://pubmed.ncbi.nlm.nih.gov/34202817/
A rare case of thrombosis and thrombocytopenia of the superior ophthalmic vein after ChAdOx1 nCoV-19 vaccination against SARS-CoV-2: https://pubmed.ncbi.nlm.nih.gov/34276917/
Thrombosis and severe acute respiratory syndrome Coronavirus 2 vaccines: vaccine-induced immune thrombotic thrombocytopenia: https://pubmed.ncbi.nlm.nih.gov/34237213/.
Limb ischemia and pulmonary artery thrombosis after ChAdOx1 nCoV-19 vaccine (Oxford-AstraZeneca): a case of vaccine-induced immune thrombotic thrombocytopenia: https://pubmed.ncbi.nlm.nih.gov/33990339/.
Secondary thrombocytopenia after SARS-CoV-2 vaccination: case report of hemorrhage and hematoma after minor oral surgery: https://pubmed.ncbi.nlm.nih.gov/34314875/.
Fatal exacerbation of ChadOx1-nCoV-19-induced thrombotic thrombocytopenia syndrome after successful initial therapy with intravenous immunoglobulins: a rationale for monitoring immunoglobulin G levels: https://pubmed.ncbi.nlm.nih.gov/34382387/
Intracerebral hemorrhage associated with vaccine-induced thrombotic thrombocytopenia after ChAdOx1 nCOVID-19 vaccination in a pregnant woman: https://pubmed.ncbi.nlm.nih.gov/34261297/
Intravenous injection of coronavirus disease 2019 (COVID-19) mRNA vaccine can induce acute myopericarditis in a mouse model: https://t.co/j0IEM8cMXI
A report of myocarditis adverse events in the U.S. Vaccine Adverse Event Reporting System. (VAERS) in association with COVID-19 injectable biologics: https://pubmed.ncbi.nlm.nih.gov/34601006/
This study concludes that: “The vaccine was associated with an excess risk of myocarditis (1 to 5 events per 100,000 persons). The risk of this potentially serious adverse event and of many other serious adverse events increased substantially after SARS-CoV-2 infection”: https://www.nejm.org/doi/full/10.1056/NEJMoa2110475?query=featured_home
Lethal vaccine-induced immune thrombotic immune thrombocytopenia (VITT) following announcement 26.COV2.S: first documented case outside the U.S.: https://pubmed.ncbi.nlm.nih.gov/34626338/
Vaccine-induced immune thrombotic thrombocytopenia (VITT): a new clinicopathologic entity with heterogeneous clinical presentations: https://pubmed.ncbi.nlm.nih.gov/34159588/
Portal vein thrombosis due to vaccine-induced immune thrombotic immune thrombocytopenia (VITT) after Covid vaccination with ChAdOx1 nCoV-19: https://pubmed.ncbi.nlm.nih.gov/34598301/
Humoral response induced by Prime-Boost vaccination with ChAdOx1 nCoV-19 and BNT162b2 mRNA vaccines in a patient with multiple sclerosis treated with teriflunomide: https://pubmed.ncbi.nlm.nih.gov/34696248/
Endovascular treatment for vaccine-induced cerebral venous sinus thrombosis and thrombocytopenia after vaccination with ChAdOx1 nCoV-19: report of three cases: https://pubmed.ncbi.nlm.nih.gov/34782400/
Cardiovascular, neurological, and pulmonary events after vaccination with BNT162b2, ChAdOx1 nCoV-19, and Ad26.COV2.S vaccines: an analysis of European data: https://pubmed.ncbi.nlm.nih.gov/34710832/
Cerebral venous thrombosis developing after vaccination.
Multiple sites of arterial thrombosis in a 35-year-old patient after vaccination with ChAdOx1 (AstraZeneca), which required emergency femoral and carotid surgical thrombectomy: https://pubmed.ncbi.nlm.nih.gov/34644642/
Intracerebral hemorrhage associated with vaccine-induced thrombotic thrombocytopenia after ChAdOx1 nCOVID-19 vaccination in a pregnant woman: https://pubmed.ncbi.nlm.nih.gov/34261297/
COVID-19 vaccine-induced immune thrombosis with thrombocytopenia thrombosis (VITT) and shades of gray in thrombus formation: https://pubmed.ncbi.nlm.nih.gov/34624910/
Acute ST-segment elevation myocardial infarction secondary to vaccine-induced immune thrombosis with thrombocytopenia (VITT): https://pubmed.ncbi.nlm.nih.gov/34580132/.
A rare case of COVID-19 vaccine-induced thrombotic thrombocytopenia (VITT) affecting the venosplanchnic and pulmonary arterial circulation from a UK district general hospital: https://pubmed.ncbi.nlm.nih.gov/34535492/
Thrombosis with thrombocytopenia syndrome (TTS) after vaccination with AstraZeneca ChAdOx1 nCoV-19 (AZD1222) COVID-19: a risk-benefit analysis for persons <60%.
Cerebral venous sinus thrombosis following vaccination with ChAdOx1: the first case of definite thrombosis with thrombocytopenia syndrome in India: https://pubmed.ncbi.nlm.nih.gov/34706921/
Thrombocytopenia with acute ischemic stroke and hemorrhage in a patient recently vaccinated with an adenoviral vector-based COVID-19 vaccine: https://pubmed.ncbi.nlm.nih.gov/33877737/
Intracerebral hemorrhage and thrombocytopenia after AstraZeneca COVID-19 vaccine: clinical and diagnostic challenges of vaccine-induced thrombotic thrombocytopenia: https://pubmed.ncbi.nlm.nih.gov/34646685/
Thrombocytopenia, including immune thrombocytopenia after receiving COVID-19 mRNA vaccines reported to the Vaccine Adverse Event Reporting System (VAERS): https://pubmed.ncbi.nlm.nih.gov/34006408/
Vaccine-induced immune thrombosis and thrombocytopenia syndrome after adenovirus-vectored severe acute respiratory syndrome coronavirus 2 vaccination: a new hypothesis on mechanisms and implications for future vaccine development: https://pubmed.ncbi.nlm.nih.gov/34664303/.
Prevalence of serious adverse events among health care professionals after receiving the first dose of ChAdOx1 nCoV-19 coronavirus vaccine (Covishield) in Togo, March 2021: https://pubmed.ncbi.nlm.nih.gov/34819146/.
Recurrent ANCA-associated vasculitis after Oxford AstraZeneca ChAdOx1-S COVID-19 vaccination: a case series of two patients: https://pubmed.ncbi.nlm.nih.gov/34755433/
Rare case of contralateral supraclavicular lymphadenopathy after vaccination with COVID-19: computed tomography and ultrasound findings: https://pubmed.ncbi.nlm.nih.gov/34667486/
Cutaneous lymphocytic vasculitis after administration of the second dose of AZD1222 (Oxford-AstraZeneca) Severe acute respiratory syndrome Coronavirus 2 vaccine: chance or causality: https://pubmed.ncbi.nlm.nih.gov/34726187/.
Cutaneous adverse reactions of 35,229 doses of COVID-19 Sinovac and AstraZeneca vaccine COVID-19: a prospective cohort study in health care workers: https://pubmed.ncbi.nlm.nih.gov/34661934/
Comments on thrombosis after vaccination: spike protein leader sequence could be responsible for thrombosis and antibody-mediated thrombocytopenia: https://pubmed.ncbi.nlm.nih.gov/34788138/
A look at the role of postmortem immunohistochemistry in understanding the inflammatory pathophysiology of COVID-19 disease and vaccine-related thrombotic adverse events: a narrative review: https://pubmed.ncbi.nlm.nih.gov/34769454/
Vaccine-associated thrombocytopenia and thrombosis: venous endotheliopathy leading to combined venous micro-macrothrombosis: https://pubmed.ncbi.nlm.nih.gov/34833382/
Thrombosis and thrombocytopenia syndrome causing isolated symptomatic carotid occlusion after COVID-19 Ad26.COV2.S vaccine (Janssen): https://pubmed.ncbi.nlm.nih.gov/34670287/
Immediate high-dose intravenous immunoglobulins followed by direct treatment with thrombin inhibitors is crucial for survival in vaccine-induced immune thrombotic thrombocytopenia
Cerebral venous sinus thrombosis, pulmonary embolism, and thrombocytopenia after COVID-19 vaccination in a Taiwanese man: a case report and review of the literature: https://pubmed.ncbi.nlm.nih.gov/34630307/
Increased risk of urticaria/angioedema after BNT162b2 mRNA COVID-19 vaccination in health care workers taking ACE inhibitors: https://pubmed.ncbi.nlm.nih.gov/34579248/
A case of unusual mild clinical presentation of COVID-19 vaccine-induced immune thrombotic thrombocytopenia with splanchnic vein thrombosis: https://pubmed.ncbi.nlm.nih.gov/34843991/
Coagulopathies after SARS-CoV-2 vaccination may derive from a combined effect of SARS-CoV-2 spike protein and adenovirus vector-activated signaling pathways: https://pubmed.ncbi.nlm.nih.gov/34639132/
Isolated pulmonary embolism after COVID vaccination: 2 case reports and a review of acute pulmonary embolism complications and follow-up: https://pubmed.ncbi.nlm.nih.gov/34804412/
Prevalence of thrombocytopenia, anti-platelet factor 4 antibodies, and elevated D-dimer in Thais after vaccination with ChAdOx1 nCoV-19: https://pubmed.ncbi.nlm.nih.gov/34568726/
Epidemiology and clinical features of myocarditis/pericarditis before the introduction of COVID-19 mRNA vaccine in Korean children: a multicenter study: https://pubmed.ncbi.nlm.nih.gov/34402230/
Case report: probable myocarditis after Covid-19 mRNA vaccine in a patient with arrhythmogenic left ventricular cardiomyopathy: https://pubmed.ncbi.nlm.nih.gov/34712717/.
Acute myocardial injury after COVID-19 vaccination: a case report and review of current evidence from the vaccine adverse event reporting system database: https://pubmed.ncbi.nlm.nih.gov/34219532/
Prevalence of thrombocytopenia, antiplatelet factor 4 antibodies, and elevated D-dimer in Thais after vaccination with ChAdOx1 nCoV-19: https://pubmed.ncbi.nlm.nih.gov/34568726/
Epidemiology and clinical features of myocarditis/pericarditis before the introduction of COVID-19 mRNA vaccine in Korean children: a multicenter study: https://pubmed.ncbi.nlm.nih.gov/34402230/
CAd26.COV2-S vaccination may reveal hereditary thrombophilia: massive cerebral venous sinus thrombosis in a young man with normal platelet count: https://pubmed.ncbi.nlm.nih.gov/34632750/
Inflammation and platelet activation after COVID-19 vaccines: possible mechanisms behind vaccine-induced immune thrombocytopenia and thrombosis: https://pubmed.ncbi.nlm.nih.gov/34887867/.
Case report: Take a second look: Cerebral venous thrombosis related to Covid-19 vaccination and thrombotic thrombocytopenia syndrome: https://pubmed.ncbi.nlm.nih.gov/34880826/
Management of a patient with a rare congenital limb malformation syndrome after SARS-CoV-2 vaccine-induced thrombosis and thrombocytopenia (VITT): https://pubmed.ncbi.nlm.nih.gov/34097311/
Bilateral thalamic stroke: a case of COVID-19 (VITT) vaccine-induced immune thrombotic thrombocytopenia or a coincidence due to underlying risk factors: https://pubmed.ncbi.nlm.nih.gov/34820232/.
Thrombocytopenia and splanchnic thrombosis after vaccination with Ad26.COV2.S successfully treated with transjugular intrahepatic intrahepatic portosystemic shunt and thrombectomy: https://onlinelibrary.wiley.com/doi/10.1002/ajh.26258
Case report: vaccine-induced immune immune thrombotic thrombocytopenia in a patient with pancreatic cancer after vaccination with messenger RNA-1273: https://pubmed.ncbi.nlm.nih.gov/34790684/
Vaccine-induced thrombotic thrombocytopenia after Ad26.COV2.S vaccination in a man presenting as acute venous thromboembolism: https://pubmed.ncbi.nlm.nih.gov/34096082/
Cardiovascular magnetic resonance findings in young adult patients with acute myocarditis after COVID-19 mRNA vaccination: a case series: https://pubmed.ncbi.nlm.nih.gov/34496880/
Myocarditis-induced sudden death after BNT162b2 COVID-19 mRNA vaccination in Korea: case report focusing on histopathological findings: https://pubmed.ncbi.nlm.nih.gov/34664804/
Recurrence of acute myocarditis temporally associated with receipt of the 2019 coronavirus mRNA disease vaccine (COVID-19) in an adolescent male: https://pubmed.ncbi.nlm.nih.gov/34166671/
Occurrence of acute infarct-like myocarditis after vaccination with COVID-19: just an accidental coincidence or rather a vaccination-associated autoimmune myocarditis?”: https://pubmed.ncbi.nlm.nih.gov/34333695/.
Self-limited myocarditis presenting with chest pain and ST-segment elevation in adolescents after vaccination with BNT162b2 mRNA vaccine: https://pubmed.ncbi.nlm.nih.gov/34180390/
Multimodality imaging and histopathology in a young man presenting with fulminant lymphocytic myocarditis and cardiogenic shock after vaccination with mRNA-1273: https://pubmed.ncbi.nlm.nih.gov/34848416/
Case report: acute fulminant myocarditis and cardiogenic shock after messenger RNA coronavirus vaccination in 2019 requiring extracorporeal cardiopulmonary resuscitation: https://pubmed.ncbi.nlm.nih.gov/34778411/
Guillain-Barré syndrome after the first dose of Pfizer-BioNTech COVID-19 vaccine: case report and review of reported cases: https://pubmed.ncbi.nlm.nih.gov/34796417/.
A case of sensory ataxic Guillain-Barre syndrome with immunoglobulin G anti-GM1 antibodies after first dose of COVID-19 BNT162b2 mRNA vaccine (Pfizer): https://pubmed.ncbi.nlm.nih.gov/34871447/
Guillain-Barré syndrome after SARS-CoV-2 vaccination in a patient with previous vaccine-associated Guillain-Barré syndrome: https://pubmed.ncbi.nlm.nih.gov/34810163/
Bell’s palsy after inactivated vaccination with COVID-19 in a patient with a history of recurrent Bell’s palsy: case report: https://pubmed.ncbi.nlm.nih.gov/34621891/
Neuromyelitis optica in a healthy woman after vaccination against severe acute respiratory syndrome coronavirus 2 mRNA-1273: https://pubmed.ncbi.nlm.nih.gov/34660149/
Acute bilateral bilateral optic neuritis/chiasm with longitudinal extensive transverse myelitis in long-standing stable multiple sclerosis after vector-based vaccination against SARS-CoV-2: https://pubmed.ncbi.nlm.nih.gov/34131771/
A case series of acute pericarditis after vaccination with COVID-19 in the context of recent reports from Europe and the United States: https://pubmed.ncbi.nlm.nih.gov/34635376/
Miller-Fisher syndrome and Guillain-Barré syndrome overlap syndrome in a patient after Oxford-AstraZeneca SARS-CoV-2 vaccination: https://pubmed.ncbi.nlm.nih.gov/34848426/.
Case report: anti-neutrophil cytoplasmic antibody-associated vasculitis with acute renal failure and pulmonary hemorrhage can occur after COVID-19 vaccination: https://pubmed.ncbi.nlm.nih.gov/34859017/
Bell’s palsy after vaccination with mRNA (BNT162b2) and inactivated (CoronaVac) SARS-CoV-2 vaccines: a case series and a nested case-control study: https://pubmed.ncbi.nlm.nih.gov/34411532/
Allergic reactions, including anaphylaxis, after receiving the first dose of Pfizer-BioNTech COVID-19 vaccine – United States, December 14 to 23, 2020: https://pubmed.ncbi.nlm.nih.gov/33641264/
Allergic reactions, including anaphylaxis, after receiving the first dose of Modern COVID-19 vaccine – United States, December 21, 2020 to January 10, 2021: https://pubmed.ncbi.nlm.nih.gov/33641268/
Pseudo-anaphylaxis reactions to Pfizer BNT162b2 vaccine: report of 3 cases of anaphylaxis following vaccination with Pfizer BNT162b2: https://pubmed.ncbi.nlm.nih.gov/34579211/
Biphasic anaphylaxis after first dose of 2019 messenger RNA coronavirus disease vaccine with positive polysorbate 80 skin test result: https://pubmed.ncbi.nlm.nih.gov/34343674/
Myocardial infarction, stroke, and pulmonary embolism after BNT162b2 mRNA COVID-19 vaccine in persons aged 75 years or older: https://pubmed.ncbi.nlm.nih.gov/34807248/
A case of acute encephalopathy and non-ST-segment elevation myocardial infarction after vaccination with mRNA-1273: possible adverse effect: https://pubmed.ncbi.nlm.nih.gov/34703815/ 767.
Case report: ANCA-associated vasculitis presenting with rhabdomyolysis and crescentic Pauci-Inmune glomerulonephritis after vaccination with Pfizer-BioNTech COVID-19 mRNA: https://pubmed.ncbi.nlm.nih.gov/34659268/
Recurrent herpes zoster after COVID-19 vaccination in patients with chronic urticaria on cyclosporine treatment – A report of 3 cases: https://pubmed.ncbi.nlm.nih.gov/34510694/
Hypermetabolic lymphadenopathy after administration of BNT162b2 mRNA vaccine Covid-19: incidence assessed by [ 18 F] FDG PET-CT and relevance for study interpretation: https://pubmed.ncbi.nlm.nih.gov/33774684/
Evolution of bilateral hypermetabolic axillary hypermetabolic lymphadenopathy on FDG PET/CT after 2-dose COVID-19 vaccination: https://pubmed.ncbi.nlm.nih.gov/34735411/
Lymphadenopathy associated with COVID-19 vaccination on FDG PET/CT: distinguishing features in adenovirus-vectored vaccine: https://pubmed.ncbi.nlm.nih.gov/34115709/.
Regional lymphadenopathy after COVID-19 vaccination: review of the literature and considerations for patient management in breast cancer care: https://pubmed.ncbi.nlm.nih.gov/34731748/
Do you want even more proof? Listed here are 140 references to adverse events of COVID injection that may occur in children.Acute-onset supraclavicular lymphadenopathy coincident with intramuscular mRNA vaccination against COVID-19 may be related to the injection technique of the vaccine, Spain, January and February 2021: https://pubmed.ncbi.nlm.nih.gov/33706861/
Thrombotic adverse events reported for Moderna, Pfizer, and Oxford-AstraZeneca COVID-19 vaccines: comparison of occurrence and clinical outcomes in the EudraVigilance database: https://pubmed.ncbi.nlm.nih.gov/34835256/
Supraclavicular lymphadenopathy after COVID-19 vaccination: an increasing presentation in the two-week wait neck lump clinic: https://pubmed.ncbi.nlm.nih.gov/33685772/
COVID-19 vaccine-related axillary and cervical lymphadenopathy in patients with current or previous breast cancer and other malignancies: cross-sectional imaging findings on MRI, CT and PET-CT: https://pubmed.ncbi.nlm.nih.gov/34719892/
Cervical lymphadenopathy after coronavirus disease vaccination 2019: clinical features and implications for head and neck cancer services: https://pubmed.ncbi.nlm.nih.gov/34526175/
Unilateral axillary lymphadenopathy related to COVID-19 vaccine: pattern on screening breast MRI allowing benign evaluation: https://pubmed.ncbi.nlm.nih.gov/34325221/
Acute-onset supraclavicular lymphadenopathy coincident with intramuscular mRNA vaccination against COVID-19 may be related to the injection technique of the vaccine, Spain, January and February 2021: https://pubmed.ncbi.nlm.nih.gov/33706861/
Thrombotic adverse events reported for Moderna, Pfizer, and Oxford-AstraZeneca COVID-19 vaccines: comparison of occurrence and clinical outcomes in the EudraVigilance database: https://pubmed.ncbi.nlm.nih.gov/34835256/
Supraclavicular lymphadenopathy after COVID-19 vaccination: an increasing presentation in the two-week wait neck lump clinic: https://pubmed.ncbi.nlm.nih.gov/33685772/
COVID-19 vaccine-related axillary and cervical lymphadenopathy in patients with current or previous breast cancer and other malignancies: cross-sectional imaging findings on MRI, CT and PET-CT: https://pubmed.ncbi.nlm.nih.gov/34719892/
Cervical lymphadenopathy after coronavirus disease vaccination 2019: clinical features and implications for head and neck cancer services: https://pubmed.ncbi.nlm.nih.gov/34526175/
Unilateral axillary lymphadenopathy related to COVID-19 vaccine: pattern on screening breast MRI allowing benign evaluation: https://pubmed.ncbi.nlm.nih.gov/34325221/
Abbate, A., Gavin, J., Madanchi, N., Kim, C., Shah, P. R., Klein, K., . . . Danielides, S. (2021). Fulminant myocarditis and systemic hyperinflammation temporally associated with BNT162b2 mRNA COVID-19 vaccination in two patients. Int J Cardiol, 340, 119-121. doi:10.1016/j.ijcard.2021.08.018. https://www.ncbi.nlm.nih.gov/pubmed/34416319
Abu Mouch, S., Roguin, A., Hellou, E., Ishai, A., Shoshan, U., Mahamid, L., . . . Berar Yanay, N. (2021). Myocarditis following COVID-19 mRNA vaccination. Vaccine, 39(29), 3790-3793. doi:10.1016/j.vaccine.2021.05.087. https://www.ncbi.nlm.nih.gov/pubmed/34092429
Albert, E., Aurigemma, G., Saucedo, J., & Gerson, D. S. (2021). Myocarditis following COVID-19 vaccination. Radiol Case Rep, 16(8), 2142-2145. doi:10.1016/j.radcr.2021.05.033. https://www.ncbi.nlm.nih.gov/pubmed/34025885
Aye, Y. N., Mai, A. S., Zhang, A., Lim, O. Z. H., Lin, N., Ng, C. H., . . . Chew, N. W. S. (2021). Acute Myocardial Infarction and Myocarditis following COVID-19 Vaccination. QJM. doi:10.1093/qjmed/hcab252. https://www.ncbi.nlm.nih.gov/pubmed/34586408
Azir, M., Inman, B., Webb, J., & Tannenbaum, L. (2021). STEMI Mimic: Focal Myocarditis in an Adolescent Patient After mRNA COVID-19 Vaccine. J Emerg Med, 61(6), e129-e132. doi:10.1016/j.jemermed.2021.09.017. https://www.ncbi.nlm.nih.gov/pubmed/34756746
Barda, N., Dagan, N., Ben-Shlomo, Y., Kepten, E., Waxman, J., Ohana, R., . . . Balicer, R. D. (2021). Safety of the BNT162b2 mRNA Covid-19 Vaccine in a Nationwide Setting. N Engl J Med, 385(12), 1078-1090. doi:10.1056/NEJMoa2110475. https://www.ncbi.nlm.nih.gov/pubmed/34432976
Bhandari, M., Pradhan, A., Vishwakarma, P., & Sethi, R. (2021). Coronavirus and cardiovascular manifestations- getting to the heart of the matter. World J Cardiol, 13(10), 556-565. doi:10.4330/wjc.v13.i10.556. https://www.ncbi.nlm.nih.gov/pubmed/34754400
Bozkurt, B., Kamat, I., & Hotez, P. J. (2021). Myocarditis With COVID-19 mRNA Vaccines. Circulation, 144(6), 471-484. doi:10.1161/CIRCULATIONAHA.121.056135. https://www.ncbi.nlm.nih.gov/pubmed/34281357
Buchhorn, R., Meyer, C., Schulze-Forster, K., Junker, J., & Heidecke, H. (2021). Autoantibody Release in Children after Corona Virus mRNA Vaccination: A Risk Factor of Multisystem Inflammatory Syndrome? Vaccines (Basel), 9(11). doi:10.3390/vaccines9111353. https://www.ncbi.nlm.nih.gov/pubmed/34835284
Calcaterra, G., Bassareo, P. P., Barilla, F., Romeo, F., & Mehta, J. L. (2022). Concerning the unexpected prothrombotic state following some coronavirus disease 2019 vaccines. J Cardiovasc Med (Hagerstown), 23(2), 71-74. doi:10.2459/JCM.0000000000001232. https://www.ncbi.nlm.nih.gov/pubmed/34366403
Calcaterra, G., Mehta, J. L., de Gregorio, C., Butera, G., Neroni, P., Fanos, V., & Bassareo, P. P. (2021). COVID 19 Vaccine for Adolescents. Concern about Myocarditis and Pericarditis. Pediatr Rep, 13(3), 530-533. doi:10.3390/pediatric13030061. https://www.ncbi.nlm.nih.gov/pubmed/34564344
Chai, Q., Nygaard, U., Schmidt, R. C., Zaremba, T., Moller, A. M., & Thorvig, C. M. (2022). Multisystem inflammatory syndrome in a male adolescent after his second Pfizer-BioNTech COVID-19 vaccine. Acta Paediatr, 111(1), 125-127. doi:10.1111/apa.16141. https://www.ncbi.nlm.nih.gov/pubmed/34617315
Chamling, B., Vehof, V., Drakos, S., Weil, M., Stalling, P., Vahlhaus, C., . . . Yilmaz, A. (2021). Occurrence of acute infarct-like myocarditis following COVID-19 vaccination: just an accidental co-incidence or rather vaccination-associated autoimmune myocarditis? Clin Res Cardiol, 110(11), 1850-1854. doi:10.1007/s00392-021-01916-w. https://www.ncbi.nlm.nih.gov/pubmed/34333695
Chang, J. C., & Hawley, H. B. (2021). Vaccine-Associated Thrombocytopenia and Thrombosis: Venous Endotheliopathy Leading to Venous Combined Micro-Macrothrombosis. Medicina (Kaunas), 57(11). doi:10.3390/medicina57111163. https://www.ncbi.nlm.nih.gov/pubmed/34833382
Chelala, L., Jeudy, J., Hossain, R., Rosenthal, G., Pietris, N., & White, C. (2021). Cardiac MRI Findings of Myocarditis After COVID-19 mRNA Vaccination in Adolescents. AJR Am J Roentgenol. doi:10.2214/AJR.21.26853. https://www.ncbi.nlm.nih.gov/pubmed/34704459
Choi, S., Lee, S., Seo, J. W., Kim, M. J., Jeon, Y. H., Park, J. H., . . . Yeo, N. S. (2021). Myocarditis-induced Sudden Death after BNT162b2 mRNA COVID-19 Vaccination in Korea: Case Report Focusing on Histopathological Findings. J Korean Med Sci, 36(40), e286. doi:10.3346/jkms.2021.36.e286. https://www.ncbi.nlm.nih.gov/pubmed/34664804
Chouchana, L., Blet, A., Al-Khalaf, M., Kafil, T. S., Nair, G., Robblee, J., . . . Liu, P. P. (2021). Features of Inflammatory Heart Reactions Following mRNA COVID-19 Vaccination at a Global Level. Clin Pharmacol Ther. doi:10.1002/cpt.2499. https://www.ncbi.nlm.nih.gov/pubmed/34860360
Chua, G. T., Kwan, M. Y. W., Chui, C. S. L., Smith, R. D., Cheung, E. C., Tian, T., . . . Ip, P. (2021). Epidemiology of Acute Myocarditis/Pericarditis in Hong Kong Adolescents Following Comirnaty Vaccination. Clin Infect Dis. doi:10.1093/cid/ciab989. https://www.ncbi.nlm.nih.gov/pubmed/34849657
Clarke, R., & Ioannou, A. (2021). Should T2 mapping be used in cases of recurrent myocarditis to differentiate between the acute inflammation and chronic scar? J Pediatr. doi:10.1016/j.jpeds.2021.12.026. https://www.ncbi.nlm.nih.gov/pubmed/34933012
Colaneri, M., De Filippo, M., Licari, A., Marseglia, A., Maiocchi, L., Ricciardi, A., . . . Bruno, R. (2021). COVID vaccination and asthma exacerbation: might there be a link? Int J Infect Dis, 112, 243-246. doi:10.1016/j.ijid.2021.09.026. https://www.ncbi.nlm.nih.gov/pubmed/34547487
Das, B. B., Kohli, U., Ramachandran, P., Nguyen, H. H., Greil, G., Hussain, T., . . . Khan, D. (2021). Myopericarditis after messenger RNA Coronavirus Disease 2019 Vaccination in Adolescents 12 to 18 Years of Age. J Pediatr, 238, 26-32 e21. doi:10.1016/j.jpeds.2021.07.044. https://www.ncbi.nlm.nih.gov/pubmed/34339728
Das, B. B., Moskowitz, W. B., Taylor, M. B., & Palmer, A. (2021). Myocarditis and Pericarditis Following mRNA COVID-19 Vaccination: What Do We Know So Far? Children (Basel), 8(7). doi:10.3390/children8070607. https://www.ncbi.nlm.nih.gov/pubmed/34356586
Deb, A., Abdelmalek, J., Iwuji, K., & Nugent, K. (2021). Acute Myocardial Injury Following COVID-19 Vaccination: A Case Report and Review of Current Evidence from Vaccine Adverse Events Reporting System Database. J Prim Care Community Health, 12, 21501327211029230. doi:10.1177/21501327211029230. https://www.ncbi.nlm.nih.gov/pubmed/34219532
Dickey, J. B., Albert, E., Badr, M., Laraja, K. M., Sena, L. M., Gerson, D. S., . . . Aurigemma, G. P. (2021). A Series of Patients With Myocarditis Following SARS-CoV-2 Vaccination With mRNA-1279 and BNT162b2. JACC Cardiovasc Imaging, 14(9), 1862-1863. doi:10.1016/j.jcmg.2021.06.003. https://www.ncbi.nlm.nih.gov/pubmed/34246585
Dimopoulou, D., Spyridis, N., Vartzelis, G., Tsolia, M. N., & Maritsi, D. N. (2021). Safety and tolerability of the COVID-19 mRNA-vaccine in adolescents with juvenile idiopathic arthritis on treatment with TNF-inhibitors. Arthritis Rheumatol. doi:10.1002/art.41977. https://www.ncbi.nlm.nih.gov/pubmed/34492161
Dimopoulou, D., Vartzelis, G., Dasoula, F., Tsolia, M., & Maritsi, D. (2021). Immunogenicity of the COVID-19 mRNA vaccine in adolescents with juvenile idiopathic arthritis on treatment with TNF inhibitors. Ann Rheum Dis. doi:10.1136/annrheumdis-2021-221607. https://www.ncbi.nlm.nih.gov/pubmed/34844930
Ehrlich, P., Klingel, K., Ohlmann-Knafo, S., Huttinger, S., Sood, N., Pickuth, D., & Kindermann, M. (2021). Biopsy-proven lymphocytic myocarditis following first mRNA COVID-19 vaccination in a 40-year-old male: case report. Clin Res Cardiol, 110(11), 1855-1859. doi:10.1007/s00392-021-01936-6. https://www.ncbi.nlm.nih.gov/pubmed/34487236
El Sahly, H. M., Baden, L. R., Essink, B., Doblecki-Lewis, S., Martin, J. M., Anderson, E. J., . . . Group, C. S. (2021). Efficacy of the mRNA-1273 SARS-CoV-2 Vaccine at Completion of Blinded Phase. N Engl J Med, 385(19), 1774-1785. doi:10.1056/NEJMoa2113017. https://www.ncbi.nlm.nih.gov/pubmed/34551225
Facetti, S., Giraldi, M., Vecchi, A. L., Rogiani, S., & Nassiacos, D. (2021). [Acute myocarditis in a young adult two days after Pfizer vaccination]. G Ital Cardiol (Rome), 22(11), 891-893. doi:10.1714/3689.36746. https://www.ncbi.nlm.nih.gov/pubmed/34709227
Fazlollahi, A., Zahmatyar, M., Noori, M., Nejadghaderi, S. A., Sullman, M. J. M., Shekarriz-Foumani, R., . . . Safiri, S. (2021). Cardiac complications following mRNA COVID-19 vaccines: A systematic review of case reports and case series. Rev Med Virol, e2318. doi:10.1002/rmv.2318. https://www.ncbi.nlm.nih.gov/pubmed/34921468
Fazolo, T., Lima, K., Fontoura, J. C., de Souza, P. O., Hilario, G., Zorzetto, R., . . . Bonorino, C. (2021). Pediatric COVID-19 patients in South Brazil show abundant viral mRNA and strong specific anti-viral responses. Nat Commun, 12(1), 6844. doi:10.1038/s41467-021-27120-y. https://www.ncbi.nlm.nih.gov/pubmed/34824230
Fikenzer, S., & Laufs, U. (2021). Correction to: Response to Letter to the editors referring to Fikenzer, S., Uhe, T., Lavall, D., Rudolph, U., Falz, R., Busse, M., Hepp, P., & Laufs, U. (2020). Effects of surgical and FFP2/N95 face masks on cardiopulmonary exercise capacity. Clinical research in cardiology: official journal of the German Cardiac Society, 1-9. Advance online publication. https://doi.org/10.1007/s00392-020-01704-y. Clin Res Cardiol, 110(8), 1352. doi:10.1007/s00392-021-01896-x. https://www.ncbi.nlm.nih.gov/pubmed/34170372
Foltran, D., Delmas, C., Flumian, C., De Paoli, P., Salvo, F., Gautier, S., . . . Montastruc, F. (2021). Myocarditis and Pericarditis in Adolescents after First and Second doses of mRNA COVID-19 Vaccines. Eur Heart J Qual Care Clin Outcomes. doi:10.1093/ehjqcco/qcab090. https://www.ncbi.nlm.nih.gov/pubmed/34849667
Forgacs, D., Jang, H., Abreu, R. B., Hanley, H. B., Gattiker, J. L., Jefferson, A. M., & Ross, T. M. (2021). SARS-CoV-2 mRNA Vaccines Elicit Different Responses in Immunologically Naive and Pre-Immune Humans. Front Immunol, 12, 728021. doi:10.3389/fimmu.2021.728021. https://www.ncbi.nlm.nih.gov/pubmed/34646267
Furer, V., Eviatar, T., Zisman, D., Peleg, H., Paran, D., Levartovsky, D., . . . Elkayam, O. (2021). Immunogenicity and safety of the BNT162b2 mRNA COVID-19 vaccine in adult patients with autoimmune inflammatory rheumatic diseases and in the general population: a multicentre study. Ann Rheum Dis, 80(10), 1330-1338. doi:10.1136/annrheumdis-2021-220647. https://www.ncbi.nlm.nih.gov/pubmed/34127481
Galindo, R., Chow, H., & Rongkavilit, C. (2021). COVID-19 in Children: Clinical Manifestations and Pharmacologic Interventions Including Vaccine Trials. Pediatr Clin North Am, 68(5), 961-976. doi:10.1016/j.pcl.2021.05.004. https://www.ncbi.nlm.nih.gov/pubmed/34538306
Gargano, J. W., Wallace, M., Hadler, S. C., Langley, G., Su, J. R., Oster, M. E., . . . Oliver, S. E. (2021). Use of mRNA COVID-19 Vaccine After Reports of Myocarditis Among Vaccine Recipients: Update from the Advisory Committee on Immunization Practices – United States, June 2021. MMWR Morb Mortal Wkly Rep, 70(27), 977-982. doi:10.15585/mmwr.mm7027e2. https://www.ncbi.nlm.nih.gov/pubmed/34237049
Gatti, M., Raschi, E., Moretti, U., Ardizzoni, A., Poluzzi, E., & Diemberger, I. (2021). Influenza Vaccination and Myo-Pericarditis in Patients Receiving Immune Checkpoint Inhibitors: Investigating the Likelihood of Interaction through the Vaccine Adverse Event Reporting System and VigiBase. Vaccines (Basel), 9(1). doi:10.3390/vaccines9010019. https://www.ncbi.nlm.nih.gov/pubmed/33406694
Gautam, N., Saluja, P., Fudim, M., Jambhekar, K., Pandey, T., & Al’Aref, S. (2021). A Late Presentation of COVID-19 Vaccine-Induced Myocarditis. Cureus, 13(9), e17890. doi:10.7759/cureus.17890. https://www.ncbi.nlm.nih.gov/pubmed/34660088
Greenhawt, M., Abrams, E. M., Shaker, M., Chu, D. K., Khan, D., Akin, C., . . . Golden, D. B. K. (2021). The Risk of Allergic Reaction to SARS-CoV-2 Vaccines and Recommended Evaluation and Management: A Systematic Review, Meta-Analysis, GRADE Assessment, and International Consensus Approach. J Allergy Clin Immunol Pract, 9(10), 3546-3567. doi:10.1016/j.jaip.2021.06.006. https://www.ncbi.nlm.nih.gov/pubmed/34153517
Haaf, P., Kuster, G. M., Mueller, C., Berger, C. T., Monney, P., Burger, P., . . . Tanner, F. C. (2021). The very low risk of myocarditis and pericarditis after mRNA COVID-19 vaccination should not discourage vaccination. Swiss Med Wkly, 151, w30087. doi:10.4414/smw.2021.w30087. https://www.ncbi.nlm.nih.gov/pubmed/34668687
Hasnie, A. A., Hasnie, U. A., Patel, N., Aziz, M. U., Xie, M., Lloyd, S. G., & Prabhu, S. D. (2021). Perimyocarditis following first dose of the mRNA-1273 SARS-CoV-2 (Moderna) vaccine in a healthy young male: a case report. BMC Cardiovasc Disord, 21(1), 375. doi:10.1186/s12872-021-02183-3. https://www.ncbi.nlm.nih.gov/pubmed/34348657
Hause, A. M., Gee, J., Baggs, J., Abara, W. E., Marquez, P., Thompson, D., . . . Shay, D. K. (2021). COVID-19 Vaccine Safety in Adolescents Aged 12-17 Years – United States, December 14, 2020-July 16, 2021. MMWR Morb Mortal Wkly Rep, 70(31), 1053-1058. doi:10.15585/mmwr.mm7031e1. https://www.ncbi.nlm.nih.gov/pubmed/34351881
Helms, J. M., Ansteatt, K. T., Roberts, J. C., Kamatam, S., Foong, K. S., Labayog, J. S., & Tarantino, M. D. (2021). Severe, Refractory Immune Thrombocytopenia Occurring After SARS-CoV-2 Vaccine. J Blood Med, 12, 221-224. doi:10.2147/JBM.S307047. https://www.ncbi.nlm.nih.gov/pubmed/33854395
Hippisley-Cox, J., Patone, M., Mei, X. W., Saatci, D., Dixon, S., Khunti, K., . . . Coupland, C. A. C. (2021). Risk of thrombocytopenia and thromboembolism after covid-19 vaccination and SARS-CoV-2 positive testing: self-controlled case series study. BMJ, 374, n1931. doi:10.1136/bmj.n1931. https://www.ncbi.nlm.nih.gov/pubmed/34446426
Ho, J. S., Sia, C. H., Ngiam, J. N., Loh, P. H., Chew, N. W., Kong, W. K., & Poh, K. K. (2021). A review of COVID-19 vaccination and the reported cardiac manifestations. Singapore Med J. doi:10.11622/smedj.2021210. https://www.ncbi.nlm.nih.gov/pubmed/34808708
Iguchi, T., Umeda, H., Kojima, M., Kanno, Y., Tanaka, Y., Kinoshita, N., & Sato, D. (2021). Cumulative Adverse Event Reporting of Anaphylaxis After mRNA COVID-19 Vaccine (Pfizer-BioNTech) Injections in Japan: The First-Month Report. Drug Saf, 44(11), 1209-1214. doi:10.1007/s40264-021-01104-9. https://www.ncbi.nlm.nih.gov/pubmed/34347278
Ioannou, A. (2021a). Myocarditis should be considered in those with a troponin rise and unobstructed coronary arteries following Pfizer-BioNTech COVID-19 vaccination. QJM. doi:10.1093/qjmed/hcab231. https://www.ncbi.nlm.nih.gov/pubmed/34463755
Ioannou, A. (2021b). T2 mapping should be utilised in cases of suspected myocarditis to confirm an acute inflammatory process. QJM. doi:10.1093/qjmed/hcab326. https://www.ncbi.nlm.nih.gov/pubmed/34931681
Isaak, A., Feisst, A., & Luetkens, J. A. (2021). Myocarditis Following COVID-19 Vaccination. Radiology, 301(1), E378-E379. doi:10.1148/radiol.2021211766. https://www.ncbi.nlm.nih.gov/pubmed/34342500
Istampoulouoglou, I., Dimitriou, G., Spani, S., Christ, A., Zimmermanns, B., Koechlin, S., . . . Leuppi-Taegtmeyer, A. B. (2021). Myocarditis and pericarditis in association with COVID-19 mRNA-vaccination: cases from a regional pharmacovigilance centre. Glob Cardiol Sci Pract, 2021(3), e202118. doi:10.21542/gcsp.2021.18. https://www.ncbi.nlm.nih.gov/pubmed/34805376
Jaafar, R., Boschi, C., Aherfi, S., Bancod, A., Le Bideau, M., Edouard, S., . . . La Scola, B. (2021). High Individual Heterogeneity of Neutralizing Activities against the Original Strain and Nine Different Variants of SARS-CoV-2. Viruses, 13(11). doi:10.3390/v13112177. https://www.ncbi.nlm.nih.gov/pubmed/34834983
Jain, S. S., Steele, J. M., Fonseca, B., Huang, S., Shah, S., Maskatia, S. A., . . . Grosse-Wortmann, L. (2021). COVID-19 Vaccination-Associated Myocarditis in Adolescents. Pediatrics, 148(5). doi:10.1542/peds.2021-053427. https://www.ncbi.nlm.nih.gov/pubmed/34389692
Jhaveri, R., Adler-Shohet, F. C., Blyth, C. C., Chiotos, K., Gerber, J. S., Green, M., . . . Zaoutis, T. (2021). Weighing the Risks of Perimyocarditis With the Benefits of SARS-CoV-2 mRNA Vaccination in Adolescents. J Pediatric Infect Dis Soc, 10(10), 937-939. doi:10.1093/jpids/piab061. https://www.ncbi.nlm.nih.gov/pubmed/34270752
Kaneta, K., Yokoi, K., Jojima, K., Kotooka, N., & Node, K. (2021). Young Male With Myocarditis Following mRNA-1273 Vaccination Against Coronavirus Disease-2019 (COVID-19). Circ J. doi:10.1253/circj.CJ-21-0818. https://www.ncbi.nlm.nih.gov/pubmed/34744118
Kaul, R., Sreenivasan, J., Goel, A., Malik, A., Bandyopadhyay, D., Jin, C., . . . Panza, J. A. (2021). Myocarditis following COVID-19 vaccination. Int J Cardiol Heart Vasc, 36, 100872. doi:10.1016/j.ijcha.2021.100872. https://www.ncbi.nlm.nih.gov/pubmed/34568540
Khogali, F., & Abdelrahman, R. (2021). Unusual Presentation of Acute Perimyocarditis Following SARS-COV-2 mRNA-1237 Moderna Vaccination. Cureus, 13(7), e16590. doi:10.7759/cureus.16590. https://www.ncbi.nlm.nih.gov/pubmed/34447639
Kim, H. W., Jenista, E. R., Wendell, D. C., Azevedo, C. F., Campbell, M. J., Darty, S. N., . . . Kim, R. J. (2021). Patients With Acute Myocarditis Following mRNA COVID-19 Vaccination. JAMA Cardiol, 6(10), 1196-1201. doi:10.1001/jamacardio.2021.2828. https://www.ncbi.nlm.nih.gov/pubmed/34185046
Kim, I. C., Kim, H., Lee, H. J., Kim, J. Y., & Kim, J. Y. (2021). Cardiac Imaging of Acute Myocarditis Following COVID-19 mRNA Vaccination. J Korean Med Sci, 36(32), e229. doi:10.3346/jkms.2021.36.e229. https://www.ncbi.nlm.nih.gov/pubmed/34402228
King, W. W., Petersen, M. R., Matar, R. M., Budweg, J. B., Cuervo Pardo, L., & Petersen, J. W. (2021). Myocarditis following mRNA vaccination against SARS-CoV-2, a case series. Am Heart J Plus, 8, 100042. doi:10.1016/j.ahjo.2021.100042. https://www.ncbi.nlm.nih.gov/pubmed/34396358
Klein, N. P., Lewis, N., Goddard, K., Fireman, B., Zerbo, O., Hanson, K. E., . . . Weintraub, E. S. (2021). Surveillance for Adverse Events After COVID-19 mRNA Vaccination. JAMA, 326(14), 1390-1399. doi:10.1001/jama.2021.15072. https://www.ncbi.nlm.nih.gov/pubmed/34477808
Klimek, L., Bergmann, K. C., Brehler, R., Pfutzner, W., Zuberbier, T., Hartmann, K., . . . Worm, M. (2021). Practical handling of allergic reactions to COVID-19 vaccines: A position paper from German and Austrian Allergy Societies AeDA, DGAKI, GPA and OGAI. Allergo J Int, 1-17. doi:10.1007/s40629-021-00165-7. https://www.ncbi.nlm.nih.gov/pubmed/33898162
Klimek, L., Novak, N., Hamelmann, E., Werfel, T., Wagenmann, M., Taube, C., . . . Worm, M. (2021). Severe allergic reactions after COVID-19 vaccination with the Pfizer/BioNTech vaccine in Great Britain and USA: Position statement of the German Allergy Societies: Medical Association of German Allergologists (AeDA), German Society for Allergology and Clinical Immunology (DGAKI) and Society for Pediatric Allergology and Environmental Medicine (GPA). Allergo J Int, 30(2), 51-55. doi:10.1007/s40629-020-00160-4. https://www.ncbi.nlm.nih.gov/pubmed/33643776
Kohli, U., Desai, L., Chowdhury, D., Harahsheh, A. S., Yonts, A. B., Ansong, A., . . . Ang, J. Y. (2021). mRNA Coronavirus-19 Vaccine-Associated Myopericarditis in Adolescents: A Survey Study. J Pediatr. doi:10.1016/j.jpeds.2021.12.025. https://www.ncbi.nlm.nih.gov/pubmed/34952008
Kostoff, R. N., Calina, D., Kanduc, D., Briggs, M. B., Vlachoyiannopoulos, P., Svistunov, A. A., & Tsatsakis, A. (2021a). Erratum to “Why are we vaccinating children against COVID-19?” [Toxicol. Rep. 8C (2021) 1665-1684 / 1193]. Toxicol Rep, 8, 1981. doi:10.1016/j.toxrep.2021.10.003. https://www.ncbi.nlm.nih.gov/pubmed/34642628
Kostoff, R. N., Calina, D., Kanduc, D., Briggs, M. B., Vlachoyiannopoulos, P., Svistunov, A. A., & Tsatsakis, A. (2021b). Why are we vaccinating children against COVID-19? Toxicol Rep, 8, 1665-1684. doi:10.1016/j.toxrep.2021.08.010. https://www.ncbi.nlm.nih.gov/pubmed/34540594
Kremsner, P. G., Mann, P., Kroidl, A., Leroux-Roels, I., Schindler, C., Gabor, J. J., . . . Group, C.-N.-S. (2021). Safety and immunogenicity of an mRNA-lipid nanoparticle vaccine candidate against SARS-CoV-2 : A phase 1 randomized clinical trial. Wien Klin Wochenschr, 133(17-18), 931-941. doi:10.1007/s00508-021-01922-y. https://www.ncbi.nlm.nih.gov/pubmed/34378087
Kustin, T., Harel, N., Finkel, U., Perchik, S., Harari, S., Tahor, M., . . . Stern, A. (2021). Evidence for increased breakthrough rates of SARS-CoV-2 variants of concern in BNT162b2-mRNA-vaccinated individuals. Nat Med, 27(8), 1379-1384. doi:10.1038/s41591-021-01413-7. https://www.ncbi.nlm.nih.gov/pubmed/34127854
Kwan, M. Y. W., Chua, G. T., Chow, C. B., Tsao, S. S. L., To, K. K. W., Yuen, K. Y., . . . Ip, P. (2021). mRNA COVID vaccine and myocarditis in adolescents. Hong Kong Med J, 27(5), 326-327. doi:10.12809/hkmj215120. https://www.ncbi.nlm.nih.gov/pubmed/34393110
Lee, E., Chew, N. W. S., Ng, P., & Yeo, T. J. (2021). Reply to “Letter to the editor: Myocarditis should be considered in those with a troponin rise and unobstructed coronary arteries following PfizerBioNTech COVID-19 vaccination”. QJM. doi:10.1093/qjmed/hcab232. https://www.ncbi.nlm.nih.gov/pubmed/34463770
Lee, E. J., Cines, D. B., Gernsheimer, T., Kessler, C., Michel, M., Tarantino, M. D., . . . Bussel, J. B. (2021). Thrombocytopenia following Pfizer and Moderna SARS-CoV-2 vaccination. Am J Hematol, 96(5), 534-537. doi:10.1002/ajh.26132. https://www.ncbi.nlm.nih.gov/pubmed/33606296
Levin, D., Shimon, G., Fadlon-Derai, M., Gershovitz, L., Shovali, A., Sebbag, A., . . . Gordon, B. (2021). Myocarditis following COVID-19 vaccination – A case series. Vaccine, 39(42), 6195-6200. doi:10.1016/j.vaccine.2021.09.004. https://www.ncbi.nlm.nih.gov/pubmed/34535317
Li, J., Hui, A., Zhang, X., Yang, Y., Tang, R., Ye, H., . . . Zhu, F. (2021). Safety and immunogenicity of the SARS-CoV-2 BNT162b1 mRNA vaccine in younger and older Chinese adults: a randomized, placebo-controlled, double-blind phase 1 study. Nat Med, 27(6), 1062-1070. doi:10.1038/s41591-021-01330-9. https://www.ncbi.nlm.nih.gov/pubmed/33888900
Li, M., Yuan, J., Lv, G., Brown, J., Jiang, X., & Lu, Z. K. (2021). Myocarditis and Pericarditis following COVID-19 Vaccination: Inequalities in Age and Vaccine Types. J Pers Med, 11(11). doi:10.3390/jpm11111106. https://www.ncbi.nlm.nih.gov/pubmed/34834458
Lim, Y., Kim, M. C., Kim, K. H., Jeong, I. S., Cho, Y. S., Choi, Y. D., & Lee, J. E. (2021). Case Report: Acute Fulminant Myocarditis and Cardiogenic Shock After Messenger RNA Coronavirus Disease 2019 Vaccination Requiring Extracorporeal Cardiopulmonary Resuscitation. Front Cardiovasc Med, 8, 758996. doi:10.3389/fcvm.2021.758996. https://www.ncbi.nlm.nih.gov/pubmed/34778411
Long, S. S. (2021). Important Insights into Myopericarditis after the Pfizer mRNA COVID-19 Vaccination in Adolescents. J Pediatr, 238, 5. doi:10.1016/j.jpeds.2021.07.057. https://www.ncbi.nlm.nih.gov/pubmed/34332972
Luk, A., Clarke, B., Dahdah, N., Ducharme, A., Krahn, A., McCrindle, B., . . . McDonald, M. (2021). Myocarditis and Pericarditis After COVID-19 mRNA Vaccination: Practical Considerations for Care Providers. Can J Cardiol, 37(10), 1629-1634. doi:10.1016/j.cjca.2021.08.001. https://www.ncbi.nlm.nih.gov/pubmed/34375696
Madelon, N., Lauper, K., Breville, G., Sabater Royo, I., Goldstein, R., Andrey, D. O., . . . Eberhardt, C. S. (2021). Robust T cell responses in anti-CD20 treated patients following COVID-19 vaccination: a prospective cohort study. Clin Infect Dis. doi:10.1093/cid/ciab954. https://www.ncbi.nlm.nih.gov/pubmed/34791081
Mangat, C., & Milosavljevic, N. (2021). BNT162b2 Vaccination during Pregnancy Protects Both the Mother and Infant: Anti-SARS-CoV-2 S Antibodies Persistently Positive in an Infant at 6 Months of Age. Case Rep Pediatr, 2021, 6901131. doi:10.1155/2021/6901131. https://www.ncbi.nlm.nih.gov/pubmed/34676123
Mark, C., Gupta, S., Punnett, A., Upton, J., Orkin, J., Atkinson, A., . . . Alexander, S. (2021). Safety of administration of BNT162b2 mRNA (Pfizer-BioNTech) COVID-19 vaccine in youths and young adults with a history of acute lymphoblastic leukemia and allergy to PEG-asparaginase. Pediatr Blood Cancer, 68(11), e29295. doi:10.1002/pbc.29295. https://www.ncbi.nlm.nih.gov/pubmed/34398511
Martins-Filho, P. R., Quintans-Junior, L. J., de Souza Araujo, A. A., Sposato, K. B., Souza Tavares, C. S., Gurgel, R. Q., . . . Santos, V. S. (2021). Socio-economic inequalities and COVID-19 incidence and mortality in Brazilian children: a nationwide register-based study. Public Health, 190, 4-6. doi:10.1016/j.puhe.2020.11.005. https://www.ncbi.nlm.nih.gov/pubmed/33316478
McLean, K., & Johnson, T. J. (2021). Myopericarditis in a previously healthy adolescent male following COVID-19 vaccination: A case report. Acad Emerg Med, 28(8), 918-921. doi:10.1111/acem.14322. https://www.ncbi.nlm.nih.gov/pubmed/34133825
Mevorach, D., Anis, E., Cedar, N., Bromberg, M., Haas, E. J., Nadir, E., . . . Alroy-Preis, S. (2021). Myocarditis after BNT162b2 mRNA Vaccine against Covid-19 in Israel. N Engl J Med, 385(23), 2140-2149. doi:10.1056/NEJMoa2109730. https://www.ncbi.nlm.nih.gov/pubmed/34614328
Minocha, P. K., Better, D., Singh, R. K., & Hoque, T. (2021). Recurrence of Acute Myocarditis Temporally Associated with Receipt of the mRNA Coronavirus Disease 2019 (COVID-19) Vaccine in a Male Adolescent. J Pediatr, 238, 321-323. doi:10.1016/j.jpeds.2021.06.035. https://www.ncbi.nlm.nih.gov/pubmed/34166671
Mizrahi, B., Lotan, R., Kalkstein, N., Peretz, A., Perez, G., Ben-Tov, A., . . . Patalon, T. (2021). Correlation of SARS-CoV-2-breakthrough infections to time-from-vaccine. Nat Commun, 12(1), 6379. doi:10.1038/s41467-021-26672-3. https://www.ncbi.nlm.nih.gov/pubmed/34737312
Moffitt, K., Cheung, E., Yeung, T., Stamoulis, C., & Malley, R. (2021). Analysis of Staphylococcus aureus Transcriptome in Pediatric Soft Tissue Abscesses and Comparison to Murine Infections. Infect Immun, 89(4). doi:10.1128/IAI.00715-20. https://www.ncbi.nlm.nih.gov/pubmed/33526560
Mohamed, L., Madsen, A. M. R., Schaltz-Buchholzer, F., Ostenfeld, A., Netea, M. G., Benn, C. S., & Kofoed, P. E. (2021). Reactivation of BCG vaccination scars after vaccination with mRNA-Covid-vaccines: two case reports. BMC Infect Dis, 21(1), 1264. doi:10.1186/s12879-021-06949-0. https://www.ncbi.nlm.nih.gov/pubmed/34930152
Montgomery, J., Ryan, M., Engler, R., Hoffman, D., McClenathan, B., Collins, L., . . . Cooper, L. T., Jr. (2021). Myocarditis Following Immunization With mRNA COVID-19 Vaccines in Members of the US Military. JAMA Cardiol, 6(10), 1202-1206. doi:10.1001/jamacardio.2021.2833. https://www.ncbi.nlm.nih.gov/pubmed/34185045
Murakami, Y., Shinohara, M., Oka, Y., Wada, R., Noike, R., Ohara, H., . . . Ikeda, T. (2021). Myocarditis Following a COVID-19 Messenger RNA Vaccination: A Japanese Case Series. Intern Med. doi:10.2169/internalmedicine.8731-21. https://www.ncbi.nlm.nih.gov/pubmed/34840235
Nagasaka, T., Koitabashi, N., Ishibashi, Y., Aihara, K., Takama, N., Ohyama, Y., . . . Kaneko, Y. (2021). Acute Myocarditis Associated with COVID-19 Vaccination: A Case Report. J Cardiol Cases. doi:10.1016/j.jccase.2021.11.006. https://www.ncbi.nlm.nih.gov/pubmed/34876937
Ntouros, P. A., Vlachogiannis, N. I., Pappa, M., Nezos, A., Mavragani, C. P., Tektonidou, M. G., . . . Sfikakis, P. P. (2021). Effective DNA damage response after acute but not chronic immune challenge: SARS-CoV-2 vaccine versus Systemic Lupus Erythematosus. Clin Immunol, 229, 108765. doi:10.1016/j.clim.2021.108765. https://www.ncbi.nlm.nih.gov/pubmed/34089859
Nygaard, U., Holm, M., Bohnstedt, C., Chai, Q., Schmidt, L. S., Hartling, U. B., . . . Stensballe, L. G. (2022). Population-based Incidence of Myopericarditis After COVID-19 Vaccination in Danish Adolescents. Pediatr Infect Dis J, 41(1), e25-e28. doi:10.1097/INF.0000000000003389. https://www.ncbi.nlm.nih.gov/pubmed/34889875
Oberhardt, V., Luxenburger, H., Kemming, J., Schulien, I., Ciminski, K., Giese, S., . . . Hofmann, M. (2021). Rapid and stable mobilization of CD8(+) T cells by SARS-CoV-2 mRNA vaccine. Nature, 597(7875), 268-273. doi:10.1038/s41586-021-03841-4. https://www.ncbi.nlm.nih.gov/pubmed/34320609
Park, H., Yun, K. W., Kim, K. R., Song, S. H., Ahn, B., Kim, D. R., . . . Kim, Y. J. (2021). Epidemiology and Clinical Features of Myocarditis/Pericarditis before the Introduction of mRNA COVID-19 Vaccine in Korean Children: a Multicenter Study. J Korean Med Sci, 36(32), e232. doi:10.3346/jkms.2021.36.e232. https://www.ncbi.nlm.nih.gov/pubmed/34402230
Park, J., Brekke, D. R., & Bratincsak, A. (2021). Self-limited myocarditis presenting with chest pain and ST segment elevation in adolescents after vaccination with the BNT162b2 mRNA vaccine. Cardiol Young, 1-4. doi:10.1017/S1047951121002547. https://www.ncbi.nlm.nih.gov/pubmed/34180390
Patel, Y. R., Louis, D. W., Atalay, M., Agarwal, S., & Shah, N. R. (2021). Cardiovascular magnetic resonance findings in young adult patients with acute myocarditis following mRNA COVID-19 vaccination: a case series. J Cardiovasc Magn Reson, 23(1), 101. doi:10.1186/s12968-021-00795-4. https://www.ncbi.nlm.nih.gov/pubmed/34496880
Patone, M., Mei, X. W., Handunnetthi, L., Dixon, S., Zaccardi, F., Shankar-Hari, M., . . . Hippisley-Cox, J. (2021). Risks of myocarditis, pericarditis, and cardiac arrhythmias associated with COVID-19 vaccination or SARS-CoV-2 infection. Nat Med. doi:10.1038/s41591-021-01630-0. https://www.ncbi.nlm.nih.gov/pubmed/34907393
Patrignani, A., Schicchi, N., Calcagnoli, F., Falchetti, E., Ciampani, N., Argalia, G., & Mariani, A. (2021). Acute myocarditis following Comirnaty vaccination in a healthy man with previous SARS-CoV-2 infection. Radiol Case Rep, 16(11), 3321-3325. doi:10.1016/j.radcr.2021.07.082. https://www.ncbi.nlm.nih.gov/pubmed/34367386
Perez, Y., Levy, E. R., Joshi, A. Y., Virk, A., Rodriguez-Porcel, M., Johnson, M., . . . Swift, M. D. (2021). Myocarditis Following COVID-19 mRNA Vaccine: A Case Series and Incidence Rate Determination. Clin Infect Dis. doi:10.1093/cid/ciab926. https://www.ncbi.nlm.nih.gov/pubmed/34734240
Perrotta, A., Biondi-Zoccai, G., Saade, W., Miraldi, F., Morelli, A., Marullo, A. G., . . . Peruzzi, M. (2021). A snapshot global survey on side effects of COVID-19 vaccines among healthcare professionals and armed forces with a focus on headache. Panminerva Med, 63(3), 324-331. doi:10.23736/S0031-0808.21.04435-9. https://www.ncbi.nlm.nih.gov/pubmed/34738774
Pinana, J. L., Lopez-Corral, L., Martino, R., Montoro, J., Vazquez, L., Perez, A., . . . Cell Therapy, G. (2022). SARS-CoV-2-reactive antibody detection after SARS-CoV-2 vaccination in hematopoietic stem cell transplant recipients: Prospective survey from the Spanish Hematopoietic Stem Cell Transplantation and Cell Therapy Group. Am J Hematol, 97(1), 30-42. doi:10.1002/ajh.26385. https://www.ncbi.nlm.nih.gov/pubmed/34695229
Revon-Riviere, G., Ninove, L., Min, V., Rome, A., Coze, C., Verschuur, A., . . . Andre, N. (2021). The BNT162b2 mRNA COVID-19 vaccine in adolescents and young adults with cancer: A monocentric experience. Eur J Cancer, 154, 30-34. doi:10.1016/j.ejca.2021.06.002. https://www.ncbi.nlm.nih.gov/pubmed/34233234
Sanchez Tijmes, F., Thavendiranathan, P., Udell, J. A., Seidman, M. A., & Hanneman, K. (2021). Cardiac MRI Assessment of Nonischemic Myocardial Inflammation: State of the Art Review and Update on Myocarditis Associated with COVID-19 Vaccination. Radiol Cardiothorac Imaging, 3(6), e210252. doi:10.1148/ryct.210252. https://www.ncbi.nlm.nih.gov/pubmed/34934954
Schauer, J., Buddhe, S., Colyer, J., Sagiv, E., Law, Y., Mallenahalli Chikkabyrappa, S., & Portman, M. A. (2021). Myopericarditis After the Pfizer Messenger Ribonucleic Acid Coronavirus Disease Vaccine in Adolescents. J Pediatr, 238, 317-320. doi:10.1016/j.jpeds.2021.06.083. https://www.ncbi.nlm.nih.gov/pubmed/34228985
Schneider, J., Sottmann, L., Greinacher, A., Hagen, M., Kasper, H. U., Kuhnen, C., . . . Schmeling, A. (2021). Postmortem investigation of fatalities following vaccination with COVID-19 vaccines. Int J Legal Med, 135(6), 2335-2345. doi:10.1007/s00414-021-02706-9. https://www.ncbi.nlm.nih.gov/pubmed/34591186
Schramm, R., Costard-Jackle, A., Rivinius, R., Fischer, B., Muller, B., Boeken, U., . . . Gummert, J. (2021). Poor humoral and T-cell response to two-dose SARS-CoV-2 messenger RNA vaccine BNT162b2 in cardiothoracic transplant recipients. Clin Res Cardiol, 110(8), 1142-1149. doi:10.1007/s00392-021-01880-5. https://www.ncbi.nlm.nih.gov/pubmed/34241676
Sessa, F., Salerno, M., Esposito, M., Di Nunno, N., Zamboni, P., & Pomara, C. (2021). Autopsy Findings and Causality Relationship between Death and COVID-19 Vaccination: A Systematic Review. J Clin Med, 10(24). doi:10.3390/jcm10245876. https://www.ncbi.nlm.nih.gov/pubmed/34945172
Sharif, N., Alzahrani, K. J., Ahmed, S. N., & Dey, S. K. (2021). Efficacy, Immunogenicity and Safety of COVID-19 Vaccines: A Systematic Review and Meta-Analysis. Front Immunol, 12, 714170. doi:10.3389/fimmu.2021.714170. https://www.ncbi.nlm.nih.gov/pubmed/34707602
Shay, D. K., Gee, J., Su, J. R., Myers, T. R., Marquez, P., Liu, R., . . . Shimabukuro, T. T. (2021). Safety Monitoring of the Janssen (Johnson & Johnson) COVID-19 Vaccine – United States, March-April 2021. MMWR Morb Mortal Wkly Rep, 70(18), 680-684. doi:10.15585/mmwr.mm7018e2. https://www.ncbi.nlm.nih.gov/pubmed/33956784
Shazley, O., & Alshazley, M. (2021). A COVID-Positive 52-Year-Old Man Presented With Venous Thromboembolism and Disseminated Intravascular Coagulation Following Johnson & Johnson Vaccination: A Case-Study. Cureus, 13(7), e16383. doi:10.7759/cureus.16383. https://www.ncbi.nlm.nih.gov/pubmed/34408937
Shiyovich, A., Witberg, G., Aviv, Y., Eisen, A., Orvin, K., Wiessman, M., . . . Hamdan, A. (2021). Myocarditis following COVID-19 vaccination: magnetic resonance imaging study. Eur Heart J Cardiovasc Imaging. doi:10.1093/ehjci/jeab230. https://www.ncbi.nlm.nih.gov/pubmed/34739045
Simone, A., Herald, J., Chen, A., Gulati, N., Shen, A. Y., Lewin, B., & Lee, M. S. (2021). Acute Myocarditis Following COVID-19 mRNA Vaccination in Adults Aged 18 Years or Older. JAMA Intern Med, 181(12), 1668-1670. doi:10.1001/jamainternmed.2021.5511. https://www.ncbi.nlm.nih.gov/pubmed/34605853
Singer, M. E., Taub, I. B., & Kaelber, D. C. (2021). Risk of Myocarditis from COVID-19 Infection in People Under Age 20: A Population-Based Analysis. medRxiv. doi:10.1101/2021.07.23.21260998. https://www.ncbi.nlm.nih.gov/pubmed/34341797
Smith, C., Odd, D., Harwood, R., Ward, J., Linney, M., Clark, M., . . . Fraser, L. K. (2021). Deaths in children and young people in England after SARS-CoV-2 infection during the first pandemic year. Nat Med. doi:10.1038/s41591-021-01578-1. https://www.ncbi.nlm.nih.gov/pubmed/34764489
Snapiri, O., Rosenberg Danziger, C., Shirman, N., Weissbach, A., Lowenthal, A., Ayalon, I., . . . Bilavsky, E. (2021). Transient Cardiac Injury in Adolescents Receiving the BNT162b2 mRNA COVID-19 Vaccine. Pediatr Infect Dis J, 40(10), e360-e363. doi:10.1097/INF.0000000000003235. https://www.ncbi.nlm.nih.gov/pubmed/34077949
Spinner, J. A., Julien, C. L., Olayinka, L., Dreyer, W. J., Bocchini, C. E., Munoz, F. M., & Devaraj, S. (2021). SARS-CoV-2 anti-spike antibodies after vaccination in pediatric heart transplantation: A first report. J Heart Lung Transplant. doi:10.1016/j.healun.2021.11.001. https://www.ncbi.nlm.nih.gov/pubmed/34911654
Starekova, J., Bluemke, D. A., Bradham, W. S., Grist, T. M., Schiebler, M. L., & Reeder, S. B. (2021). Myocarditis Associated with mRNA COVID-19 Vaccination. Radiology, 301(2), E409-E411. doi:10.1148/radiol.2021211430. https://www.ncbi.nlm.nih.gov/pubmed/34282971
Sulemankhil, I., Abdelrahman, M., & Negi, S. I. (2021). Temporal association between the COVID-19 Ad26.COV2.S vaccine and acute myocarditis: A case report and literature review. Cardiovasc Revasc Med. doi:10.1016/j.carrev.2021.08.012. https://www.ncbi.nlm.nih.gov/pubmed/34420869
Tailor, P. D., Feighery, A. M., El-Sabawi, B., & Prasad, A. (2021). Case report: acute myocarditis following the second dose of mRNA-1273 SARS-CoV-2 vaccine. Eur Heart J Case Rep, 5(8), ytab319. doi:10.1093/ehjcr/ytab319. https://www.ncbi.nlm.nih.gov/pubmed/34514306
Takeda, M., Ishio, N., Shoji, T., Mori, N., Matsumoto, M., & Shikama, N. (2021). Eosinophilic Myocarditis Following Coronavirus Disease 2019 (COVID-19) Vaccination. Circ J. doi:10.1253/circj.CJ-21-0935. https://www.ncbi.nlm.nih.gov/pubmed/34955479
Team, C. C.-R., Food, & Drug, A. (2021). Allergic Reactions Including Anaphylaxis After Receipt of the First Dose of Pfizer-BioNTech COVID-19 Vaccine – United States, December 14-23, 2020. MMWR Morb Mortal Wkly Rep, 70(2), 46-51. doi:10.15585/mmwr.mm7002e1. https://www.ncbi.nlm.nih.gov/pubmed/33444297
Thompson, M. G., Burgess, J. L., Naleway, A. L., Tyner, H., Yoon, S. K., Meece, J., . . . Gaglani, M. (2021). Prevention and Attenuation of Covid-19 with the BNT162b2 and mRNA-1273 Vaccines. N Engl J Med, 385(4), 320-329. doi:10.1056/NEJMoa2107058. https://www.ncbi.nlm.nih.gov/pubmed/34192428
Tinoco, M., Leite, S., Faria, B., Cardoso, S., Von Hafe, P., Dias, G., . . . Lourenco, A. (2021). Perimyocarditis Following COVID-19 Vaccination. Clin Med Insights Cardiol, 15, 11795468211056634. doi:10.1177/11795468211056634. https://www.ncbi.nlm.nih.gov/pubmed/34866957
Truong, D. T., Dionne, A., Muniz, J. C., McHugh, K. E., Portman, M. A., Lambert, L. M., . . . Newburger, J. W. (2021). Clinically Suspected Myocarditis Temporally Related to COVID-19 Vaccination in Adolescents and Young Adults. Circulation. doi:10.1161/CIRCULATIONAHA.121.056583. https://www.ncbi.nlm.nih.gov/pubmed/34865500
Tutor, A., Unis, G., Ruiz, B., Bolaji, O. A., & Bob-Manuel, T. (2021). Spectrum of Suspected Cardiomyopathy Due to COVID-19: A Case Series. Curr Probl Cardiol, 46(10), 100926. doi:10.1016/j.cpcardiol.2021.100926. https://www.ncbi.nlm.nih.gov/pubmed/34311983
Umei, T. C., Kishino, Y., Shiraishi, Y., Inohara, T., Yuasa, S., & Fukuda, K. (2021). Recurrence of myopericarditis following mRNA COVID-19 vaccination in a male adolescent. CJC Open. doi:10.1016/j.cjco.2021.12.002. https://www.ncbi.nlm.nih.gov/pubmed/34904134
Vidula, M. K., Ambrose, M., Glassberg, H., Chokshi, N., Chen, T., Ferrari, V. A., & Han, Y. (2021). Myocarditis and Other Cardiovascular Complications of the mRNA-Based COVID-19 Vaccines. Cureus, 13(6), e15576. doi:10.7759/cureus.15576. https://www.ncbi.nlm.nih.gov/pubmed/34277198
Visclosky, T., Theyyunni, N., Klekowski, N., & Bradin, S. (2021). Myocarditis Following mRNA COVID-19 Vaccine. Pediatr Emerg Care, 37(11), 583-584. doi:10.1097/PEC.0000000000002557. https://www.ncbi.nlm.nih.gov/pubmed/34731877
Warren, C. M., Snow, T. T., Lee, A. S., Shah, M. M., Heider, A., Blomkalns, A., . . . Nadeau, K. C. (2021). Assessment of Allergic and Anaphylactic Reactions to mRNA COVID-19 Vaccines With Confirmatory Testing in a US Regional Health System. JAMA Netw Open, 4(9), e2125524. doi:10.1001/jamanetworkopen.2021.25524. https://www.ncbi.nlm.nih.gov/pubmed/34533570
Watkins, K., Griffin, G., Septaric, K., & Simon, E. L. (2021). Myocarditis after BNT162b2 vaccination in a healthy male. Am J Emerg Med, 50, 815 e811-815 e812. doi:10.1016/j.ajem.2021.06.051. https://www.ncbi.nlm.nih.gov/pubmed/34229940
Weitzman, E. R., Sherman, A. C., & Levy, O. (2021). SARS-CoV-2 mRNA Vaccine Attitudes as Expressed in U.S. FDA Public Commentary: Need for a Public-Private Partnership in a Learning Immunization System. Front Public Health, 9, 695807. doi:10.3389/fpubh.2021.695807. https://www.ncbi.nlm.nih.gov/pubmed/34336774
Welsh, K. J., Baumblatt, J., Chege, W., Goud, R., & Nair, N. (2021). Thrombocytopenia including immune thrombocytopenia after receipt of mRNA COVID-19 vaccines reported to the Vaccine Adverse Event Reporting System (VAERS). Vaccine, 39(25), 3329-3332. doi:10.1016/j.vaccine.2021.04.054. https://www.ncbi.nlm.nih.gov/pubmed/34006408
Witberg, G., Barda, N., Hoss, S., Richter, I., Wiessman, M., Aviv, Y., . . . Kornowski, R. (2021). Myocarditis after Covid-19 Vaccination in a Large Health Care Organization. N Engl J Med, 385(23), 2132-2139. doi:10.1056/NEJMoa2110737. https://www.ncbi.nlm.nih.gov/pubmed/34614329
Zimmermann, P., & Curtis, N. (2020). Why is COVID-19 less severe in children? A review of the proposed mechanisms underlying the age-related difference in severity of SARS-CoV-2 infections. Arch Dis Child. doi:10.1136/archdischild-2020-320338. https://www.ncbi.nlm.nih.gov/pubmed/33262177
(Natural News) The U.S. Centers for Disease Control and Prevention (CDC) is finally admitting that PCR tests have no place in trying to detect the presence of the Wuhan coronavirus (Covid-19) inside a person’s body.
Rochelle Walensky, the fake federal agency’s top dog, told ABC News in a recent interview that the “new science” shows that PCR tests do not work, and the government is no longer using them.
“With all of that science together, we moved forward with isolation recommendations of five days of isolation followed by five days in a mask,” Walensky explained about the new guidelines (watch the interview below).
“Now the question of why we didn’t include a test there is simply because we know that PCRs can stay positive for up to 12 weeks. So we would have people in isolation for a very long time if we were relying on PCRs.”
NaturalNews videos would not be possible without you, as always we remain passionately dedicated to our mission of educating people all over the world on the subject of natural healing remedies and personal liberty (food freedom, medical freedom, the freedom of speech, etc.). Together, we’re helping create a better world, with more honest food labeling, reduced chemical contamination, the avoidance of toxic heavy metals and vastly increased scientific transparency.
NaturalNews videos would not be possible without you, as always we remain passionately dedicated to our mission of educating people all over the world on the subject of natural healing remedies and personal liberty (food freedom, medical freedom, the freedom of speech, etc.). Together, we’re helping create a better world, with more honest food labeling, reduced chemical contamination, the avoidance of toxic heavy metals and vastly increased scientific transparency.
There are nearly 100,000 excess deaths happening per month in the USA right now, according to life insurance companies that are sounding the alarm over what Dr. Robert Malone calls a “mass casualty event” that’s unfolding due to covid vaccines.
— Is this the Holy Grail in Medicine?
Denied by Big Pharma, MMS has proven to be a cheap and effective treatment/cure for virtually every ailment under the sun!
Trump was right… chlorine dioxide cures. It is NOT Bleach as the media claimed, it is safe and natural.
This documentary (mirror) produced by Adam Abraham working with Jim Humble in Mexico tells the story of MMS and many of the accomplishments that has occurred since Jim first wrote the book that is sold on his site – The Miracle Mineral Solution of the 21st Century. There are excerpts and testimony from doctors and scientists in Mexico and the US.
Jim is an ex miner who first witnessed it’s use for treating malaria and has since gone on to investigate the possibility of treating a variety of other ailments and diseases ranging from coughs and colds, flu, tuberculosis, lime disease, psoriasis and cancer.
Quite a number of other people give their opinions and observations who all attest to the effectiveness of MMS.
This documentary is very professional done and it gives you a very interesting look into the new world of MMS. The observations and happenings are all factual.
Please enjoy this documentary and share it with all your friends and family.
Vitamin D optimization is likely the easiest, least expensive and most beneficial strategy that anyone can do to help minimize their risk of infections including COVID-19 coming months
More than 1 billion individuals worldwide, across all age groups, are deficient in vitamin D, which has now been identified as a significant risk factor for positive COVID-19 status, severe COVID-19 infection and death thereof
In Indonesia, people with a vitamin D level between 20 ng/mL and 30 ng/mL had a sevenfold higher risk of death than those with a level above 30 ng/mL. Having a level below 20 ng/mL was associated with a 12 times higher risk of death
To improve your immune function and lower your risk of viral infections, you’ll want to raise your vitamin D to a level between 60 ng/mL and 80 ng/mL (150 nmol/L and 200 nmol/L) by fall
Vitamin D optimization is particularly important for dark-skinned individuals, as the darker your skin, the more sun exposure you need to raise your vitamin D level, as well as the elderly
This article was previously published June 22, 2020, and has been updated with new information.
All things considered, vitamin D optimization is likely the easiest, least expensive and most beneficial strategy that anyone can do to minimize their risk of COVID-19 and other infections in the coming months. Health authorities are already warning of a second wave of COVID-19 in the fall, which means the time to start addressing your vitamin D level is NOW.
We also have a pandemic of vitamin D deficiency, as more than 1 billion individuals worldwide, across all age groups, are deficient in vitamin D.1,2,3,4 Vitamin D deficiency has now been identified as a significant risk factor for positive COVID-19 status,5,6 severe COVID-19 infection7,8,9,10 and death thereof.11,12
In one study,13,14 which looked at data from 780 hospital patients in Indonesia, those with a vitamin D level between 20 nanograms per milliliter (ng/mL) and 30 ng/mL had a sevenfold higher risk of death than those with a level above 30 ng/mL. Having a level below 20 ng/mL was associated with a 12 times higher risk of death.
To improve your immune function and lower your risk of viral infections, you’ll want to raise your vitamin D to a level between 60 ng/mL and 80 ng/mL by fall. In Europe, the measurements you’re looking for are 150 nmol/L and 200 nmol/L. If vitamin D levels were increased in the global population, tens of thousands of people may be saved if or when COVID-19 reemerges.
While prospective controlled studies demonstrating vitamin D’s effectiveness in COVID-19 are still lacking, there are many such studies underway. You can review the status of these trials on clinicaltrials.gov.15 As of early June 2020, more than 20 studies had been launched to investigate the benefits of vitamin D against COVID-19.
The Most Important Paper I’ve Ever Written
The comprehensive vitamin D report below has been reviewed by many vitamin D scientists for accuracy. This was done to develop a resource that everyone can share to help educate others. We will soon be launching a campaign to educate and inspire everyone, everywhere, to start optimizing their vitamin D level NOW. Please download my paper here, and share it with everyone you know.
The purpose of this report is to help you understand why it is so important to optimize vitamin levels for healthy immune functions and then provide you with a detailed strategy of how to do that. This report can be used as a tool to teach your friends, family and community about why and how to be prepared for the next pandemic.
In it, I review the science of how your immune system works, and the regulatory role of vitamin D. I also explain how vitamin D reduces your risk of COVID-19 specifically, and how it helps suppress and control both acute respiratory distress syndrome (ARDS) and cytokine storms, which is a primary cause of death in COVID-19.
Darker-Skinned Individuals Need More Vitamin D
Vitamin D optimization is particularly important for dark-skinned individuals, as the darker your skin, the more sun exposure you need to raise your vitamin D level. Increased skin pigmentation reduces the efficacy of UVB because melanin functions as a natural sunblock.
If you’re very dark-skinned, you may need to spend about 1.5 hours a day in the sun to have any noticeable effect. For many working adults and school-age children, this simply isn’t feasible.
Light-skinned individuals may only need 15 minutes of full sun exposure a day, which is far easier to achieve. Still, they too will typically struggle to maintain ideal levels during the winter. During the winter months at latitudes of greater than 40°, little or no UVB radiation reaches the surface of the earth. That said, residence at low latitude does not guarantee adequate vitamin D levels, since social and cultural norms may limit sun exposure.16
As noted in the MedCram video above, black, Asian and minority ethnic groups are at an increased risk of death from COVID-19. While some have blamed this racial disparity on health care access, a far more likely reason for this is because dark-skinned individuals are far more likely to be deficient in vitamin D.
In fact, the paper cited by MedCram specifically looked at ethnic disparities in COVID-19 mortality among patients in England, where health care is freely available to all, so the health care access rationale doesn’t seem to hold water.
Vitamin D Supplementation Recommended to Quell Mortality
The role of vitamin D is addressed in a reply17 by vitamin D researchers William Grant and Barbara Boucher to The BMJ editorial “Is Ethnicity Linked to Incidence or Outcomes of COVID-19?” They write, in part:
“The recent BMJ editorial by Khunti et al. asks ‘Is ethnicity linked to incidence or outcomes of covid-19?’ Here we outline how ethnicity relates to incidence and outcomes of COVID-19 due, in part, to lack of vitamin D because of increased skin pigmentation and diet …
A potentially important factor not considered in the PHE report was vitamin D deficiency, though mounting evidence suggests that vitamin D deficiency is an important risk factor for acute respiratory tract infections and for COVID-19 …
Mounting evidence demonstrates that vitamin D has important roles in regulating the immune system that should reduce COVID-19 risks; primarily by reducing survival and replication of the SARS-CoV-2 virus and by reducing the risks of ‘cytokine storms’ by reducing pro-inflammatory cytokine production and increasing anti-inflammatory cytokine production.
Vitamin D also promotes local ACE2 formation in the lungs, an effect known to reduce the severity of acute respiratory distress syndrome. Furthermore, higher baseline serum 25(OH)D concentrations are currently being reported to be associated with reduced rates of severe COVID-19 and of mortality.”
Grant and Boucher recommend advising the public to supplement vitamin D daily, especially black, Asian and minority ethnic groups, indoor workers, shift workers, the elderly, those in residential care or those confined to their homes, as well as those who are obese. Doing so might reduce COVID-19 severity and prevent unnecessary deaths.
“Vitamin D is readily available … ‘over the counter’ at supermarkets, chemists and online, but could be provided free to those in financial hardship or unable to access supplies,” Grant and Boucher write, adding:
“Doses of 1,000 IU/day in general and of 4,000 IU/day for those at high risk of deficiency, as above, including the BAME groups, should be advised for the duration of the Covid-19 outbreak …”
Sunscreen Advice Counters Lifesaving Vitamin D Message
Remarkably, while the importance of vitamin D against COVID-19 is becoming more widely recognized by doctors, some are still advising against either sun exposure or vitamin D supplementation, or both.
Some, such as Dr. Pieter Cohen, an internal medicine physician at Cambridge Health Alliance in Massachusetts and an associate professor medicine at Harvard Medical School, is even discouraging people from getting their vitamin D level tested to see if they’re deficient!18 A June 1, 2020, report on Today.com states:19
“The body can manufacture vitamin D when the skin is exposed to the sun or get it from food. ‘I’m not making a general recommendation for supplements. I’m saying: To avoid vitamin D deficiency.
It will usually take only being outdoors, getting incidental sun exposure, plus paying attention to the dietary sources of vitamin D,’ [Dr. JoAnn Manson, chief of preventive medicine at Brigham and Women’s Hospital and professor of medicine at Harvard] noted.
Incidental sun exposure means getting some sunshine during a 30-minute walk or other outdoor exercise while wearing shorts or short sleeves (though you should still use sunscreen). It doesn’t mean going out specifically to sun bathe.”
The advice to wear sunscreen while getting “incidental” sun exposure is medically irrational and incorrect, since sunscreen filters out the very ultraviolet rays that trigger vitamin D production in your skin.
In order for sensible sun exposure to work, you need unprotected exposure. Just make sure you don’t get sunburned. All you need is to stay out until your skin turns the lightest shade of pink. After that, cover up with long sleeves and pants.
Help Us Spread the Word!
It is my sincere hope and desire that all of you will help us in this effort to spread the word about vitamin D and get your friends and family on board to get their vitamin levels optimized. We need a citizen army of activists to spread the word. My vitamin D report can help you in this effort. I urge you to share it with everyone you know. I hope to collaborate with all the major natural medical sites to participate in this process.
The vitamin D level you’re aiming for is between 60 ng/mL and 80 ng/mL. In Europe, the measurements you’re looking for are 150 nmol/L and 200 nmol/L. In my vitamin D report, I detail how to go about doing this, but here’s a quick summary of the key steps:
1.First, measure your vitamin D level — One of the easiest and most cost-effective ways of measuring your vitamin D level is to participate in the GrassrootsHealth’s personalized nutrition project, which includes a vitamin D testing kit.
Once you know what your blood level is, you can assess the dose needed to maintain or improve your level. The easiest way to raise your level is by getting regular, sensible sun exposure, as discussed above.
If you cannot get enough vitamin D from the sun (you can use the DMinder app20 to see how much vitamin D your body can make depending on your location and other individual factors), then you’ll need an oral supplement. It’s strongly recommended to take magnesium and K2 concomitant with oral vitamin D.
2.Assess your individualized vitamin D dosage — To do that, you can either use the chart below, or use GrassrootsHealth’s Vitamin D*calculator. To convert ng/mL into the European measurement (nmol/L), simply multiply the ng/mL measurement by 2.5. To calculate how much vitamin D you may be getting from regular sun exposure in addition to your supplemental intake, use the DMinder app.21
3.Retest in three to six months — Lastly, you’ll need to remeasure your vitamin D level in three to six months, to evaluate how your sun exposure and/or supplement dose is working for you.
The Orwellian Planet continues to reveal itself as now the inventor of mRNA technology has been suspended from Twitter for warning of the deadly side effects. Alex Jones announces he will be on Joe Rogan this week. A verdict in the Maxwell trial is reached. Owen Shroyer gives his response, as does Alex and reporter Kristan Harris. The great bait and switch of the covid lies begins, as Fuaci, Wen and others are now saying the exact opposite of everything they had been saying. Owen also breaks down the idea and concept of A.I. in a way you’ve never heard before.
———————————
Tägliche politische und Geoengineering-Nachrichten: https://vk.com/chembuster
EVEN ATTACKS BY MEANS OF NEGATIVE REVIEWS CANNOT STOP THE TRUTH TO BE EXPOSED
================================================================================
ENGLISH
MEL-K
We want to wish all our patriot pals happy holidays and an amazing New Year! We are back in the sunshine state for some family time as we continue to be on the road escaping the formally great city of NY touring the country meeting patriots everywhere. We are grateful for all your support and for being back in free America.
During this crazy time we live in, remember that unity and love will prevail and that God Wins!. But we all must do our parts. One way we can contribute is to all try to do with less stuff this holiday season but if we must shop, please remember to defund the cabal & refund America by supporting all the amazing Patriots fighting on the front lines.
Let’s also get out and meet each other at Mel’s upcoming live in person speaking events:
Phoenix AZ – January 14-15 (Reawaken America Tour)
Oklahoma City, OK January 22 (Sherwood For Governor – Make Oklahoma Free Rally)
Canton, OH February 18-19 (Reawaken America Tour)
San Diego, CA March 11-12 (Reawaken America Tour)
Redmond, OR – April 1-2 (Reawaken America Tour)
See our website events page and follow the link to the events. Remember to mention Mel K for great discounts on all these fun and informative events. See you there!
RE:AWAKENING Movie Just Launched ! – see our partners page !
Important Update To Those That Support us with Donations:
A certain payment company that sounds like FayGal and their sister company FenMo have deemed The Mel K Show against their respective acceptable use policies. Please use free speech friendly Align Pay for donations at https://themelkshow.com/donate/ or support us in others ways such as our partners or TheMelKShow.TV
We love what we do and are working hard to keep on top of everything to help this transition along peacefully and with love. Please support our work in any way you can. Like, Share, Comment and If you value our work and have the resources please support us through http://www.themelkshow.compartners or donation pages. https://themelkshow.com/donate/
The Mel K Show Mailing Address
1040 First Avenue #367
New York, NY 10022
If you are interested to explore investing in precious metals please contact below and mention MelK for special offers: https://bit.ly/BeverlyHillsPreciousMetals
Andrew Sorchini telephone 866-346-5325
Beverly Hills Precious Metals Website http://www.BH-PM.com
Support Patriots With MyPillow
Go to http://www.MyPillow.com and use offer code “MelK” to support both MyPillow and The Mel K Show
EMP Shield
EMP Shield is designed to protect an entire home from lightning, solar flare (coronal mass ejection), power surges, and an electromagnetic pulse. Use promo code MelK https://www.empshield.com/?coupon=melk
My Daily Sprays
Portable easy to use sprays made with only the best clinically proven ingredients that support healthy daily activity, including superfruits and natural antioxidants. https://bit.ly/MDC-My-Daily-Sprays
Take care of your health with Dr. Mark Sherwood and his team at Functional Medical Institute http://www.Sherwood.tv/melk – download the free e-book to develop physical and emotional resiliency
Thank you amazing patriots for joining us on this journey, for your support of our work and for your faith in this biblical transition to greatness.
——————————————————————-
Tägliche politische und Geoengineering-Nachrichten: https://vk.com/chembuster
While the Democrats and White House have been adamant about pushing the COVID-19 jab on the American people, the Biden administration recently announced that they would be ramping up efforts to get more children to take the jab to fight against COVID-19. Although the administration promises this is for the safety and well-being of children and the future of America, A professor of epidemiology at Yale University isn’t buying the narrative being presented by the White House given that children showing severe symptoms from COVID-19 is rare.
In the video, which can be watched below, Dr. Harvey Risch was speaking on Fox News when the new agenda from the Biden administration came up. Dr. Risch didn’t shy away from the motives behind the push and how the Democrats are not allowing science to guide them when fighting COVID-19.
Alex Jones discusses how the medical establishment is out of control, and he explains how Dr. Fauci’s lawless liberty with horrific scientific experiments is a sign of that imbalance.
Start your journey! Save 25% on Resetwars.com today & get exclusive information that exposes the globalist agenda during our special Holiday Sale that will only be online until Tuesday, December 28th at PM!
Alex Jones lays out the latest world ending developments surrounding COVID vaccines, global government, and humanity’s struggle to maintain its freedom.
Get FREE shipping and double Patriot Points during our Christmas Super Sale now!
Alex Jones breaks down what the WHO’s warning about a global healthcare collapse means and explains how they triggered it through their COVID hysteria. Also, Steve Kirsch joins Alex Jones live via Skype to reveal the findings of new studies that confirm to an even greater degree the fact that COVID vaccines cause cardiovascular disease and cause recipients’ own immune system to attack the heart. Harrison Smith hosts the fourth and final hour.
This short video gives a synopsis of stories from a number of persons who say they and/or their family members suffered severe side effects after getting the COVID-19 shots.
From full-body convulsions to myriad neurological disorders to blood clots and platelet problems to deaths, the reported side effects are severe and disturbing to watch. “I knew it had to be from the vaccine,” one woman says.
In a stunning video interview with a doctor treating COVID-19 patients, The Desert Review uncovers the secrets health officials and hospitals aren’t telling — and that is that “they are being held hostage and segregated from loved ones. And the reason is money.”
“COVID patients in America’s hospitals today are actually being treated worse than prisoners in American jails,” Dr. Elizabeth Lee Vliet says. The very structure of how hospitals are reimbursed for COVID patients is what’s causing this, she says.
“They (the hospitals) are paid by the government to do a PCR test on every patient who walks in the door … Then they are paid extra for a COVID admission to the hospital. They are paid an extra 20% bonus on the entire hospital bill, if the hospital ONLY uses remdesivir to treat the patient.
“And then if the patient goes on a ventilator, which is a consequence of some of the toxicity of remdesivir and the restriction of fluids and nutrients that they are also doing, and once the patient is on a ventilator there is ANOTHER incentive bonus to the hospitals. If the patient dies in the hospital, there is another incentive payment,” Vliet states.
This video is over an hour long but it’s worth watching every minute. It could save your or a loved one’s life.
Elizabeth Lee Vliet MD is a heroic physician who, earlier than most other medical doctors throughout the world, was so appalled by the failure to treat COVID-19 patients that she became a COVID treating physician. Having founded the Truth for Health Foundation, with Peter McCullough, MD MPH as Chief Medical Advisor, she has now found herself confronted with the tragic and horrific reality of COVID patients dying due to neglect and bad treatment in hospitals throughout the U.S. and elsewhere. Many of these treatment centers seem so intent on murdering their patients that they refuse court orders to treat with routine antiviral therapies like steroids as well specific treatments like hydroxychloroquine and ivermectin. Incentivized by high reimbursement payments for treating dying COVID patients and by using potentially deadly treatments like ventilators and remdesivir, the doctors and hospitals have descended into unethical, corrupt medical practices.
These chilling stories highlight the culture of death into which American society is descending. They led our interview to examine the global predators and progressive ideologues who are driving otherwise sane physicians and honorable institutions to kill their patients through a combination of neglect, mistreatment and, at times, deadly interventions. This is an interview that should become a shot heard around the world to alert humanity to the ongoing destruction of Western civilization in the name of treating COVID-19.
Are myocarditis and pericarditis from the COVID-19 shots as “extremely rare” as the CDC and other world health agencies and officials say? Not by a long shot, says Steve Kirsch, who’s been following and investigating reported side effects of the COVID jabs.
A retired engineer with two degrees, Kirsch has no conflicts of interest in this issue; he’s just interested in the truth. And the truth is the rates of myocarditis in boys after a COVID jab are as much as 100 times higher than the 1 in 13,000 you’re being told.
Even before Kirsch’s latest findings, the CDC’s own numbers showed it was more like 41 times higher. But now the numbers from a school in California indicate the number is closer 1 in 95.
This is not something to be swept aside, Kirsch says, because children are being sacrificed for the sake of the shot, and they are going to die unnecessarily unless somebody speaks out. And that, he says, is why he is telling the world the truth, even though he knows the CDC will deny the numbers.
In his latest blog, he meticulously lays out those truths — including the fact that the CDC is lying about the rates of vaccine-induced myocarditis compared to COVID-induced myocarditis.
One reason the CDC has changed its rules to not require retesting for COVID-19 infection after quarantine is that the PCR tests used to determine infectivity can stay positive for up to 12 weeks.
The rapid antigen tests also may be less sensitive to the Omicron variant, according to CDC director Dr. Rochelle Walensky, but even so, if you test negative on the rapid test and you have symptoms, you need to get the PCR test anyway.
Then, if you have symptoms and test positive on the PCR test, you just don’t have to retest after you’ve quarantined, as the long positivity rates for the PCR tests “would have people in isolation for a very long time if we were relying on PCRs,” she told ABC News.
Kyle’s vaccine complication 21 Oct 2021. Kyle age 29 talks with Dr John Campbell about his adverse reactions to the Pfizer jab and how it effects his life and health. 2nd dose taken June 10 2021
Thank you for your ongoing support, Please subscribe to my Bitchute channel.
You can also find me on Telegram https://t.me/hazels_vibes
The Hill
Dec 19, 2021
Tuesday, a Select Subcommittee on the Coronavirus Crisis held a remote hearing examining the urgent need to accelerate global coronavirus vaccination efforts and the critical role that these efforts play in the nation’s public health and economic recovery. Congressman Jim Jordan expressed his desire for CDC to use some of its funding to figure out how effective natural immunity is as an alternative to a vaccine.
December 14, 2021, a Select Subcommittee on the Coronavirus Crisis held a remote hearing in which they debated the need for an accelerated vaccination effort. In the outtake from that meeting (video above), Congressman Jim Jordan, R-Ohio, points out that the U.S. Centers for Disease Control and Prevention and the NIH/NIAID have a combined annual budget of about $58 billion, and a combined staff of 31,000.
With that kind of budget and an army of staff, why has the U.S. government not done a study to determine how natural immunity stacks up against the COVID jab? Jordan asked. The answer he received (from an, unfortunately, unidentified doctor) was refreshingly direct:
“I don’t think they want to know the answer,” because “it would undermine the indiscriminate vaccination policy for every single human being, including extremely low risk people.”
According to a Columbia University study, more than half the American population have now been exposed to the SARS-CoV-2 virus in one form or another, and have natural immunity, and according to an Israeli study, natural immunity is 27 times more effective than the COVID shot.19
So, why are government leaders and so-called health authorities still acting as though natural immunity is irrelevant and the only way to control the pandemic is through repeated injections with experimental — and clearly hazardous — gene transfer technology?
I believe the answer is they’re ignoring natural immunity because their primary objective and goal it to have everyone injected. They want everyone routinely jabbed so they can justify the rollout of health passports, which will become the foundation for an all-encompassing digital ID control system.
In short, our public health agencies have been hijacked and are carrying out an anti-human, anti-health agenda intended to enslave the public in a technocratic control grid.
There’s no doubt anymore that the vaccine passports will be expanded to encompass financial transactions and incorporate a social credit system. Together, all of these pieces will allow an unelected elite to control the lives of every person on the planet, down to the minutest details of our everyday lives.
While Fauci and Collins are certainly not alone in this effort, and likely not even close to the top of the technocratic food chain, they have played very important roles. It’s time to see them for who and what they are, and demand that they be held to account for their actions.
Busted by their own emails! Fauci and his boss, NIH Director Francis Collins, engaged in a conspiracy to defame and destroy the work of three prominent scientists from Stanford, Harvard, and Oxford, which challenged the Fauci/Collins lockdown strategy to address last year’s virus outbreak. Thanks to a Freedom of Information request we see how Anthony “I’m the science” Fauci really operates behind the scenes. Also today, Fauci says force your fully-vaxxed family members to take a covid test before tucking into the turkey.
Another cache of emails obtained via a Freedom of Information Act (FOIA) request by the American Institute for Economic Research (AIER) reveals Dr. Anthony Fauci and his boss, National Institutes of Health director Francis Collins, colluded to quash dissenting views on the lockdowns
October 4, 2020, three medical professors — Martin Kulldorff from Harvard, Sunetra Gupta from Oxford and Jay Bhattacharya from Stanford — launched the Great Barrington Declaration, which called for focused protection of high-risk individuals rather than the continuation of blanket lockdowns
As support of the declaration rapidly spread, Fauci and Collins discussed how they could stop the call for a sane, science-based approach. In an email to Fauci, Collins wrote, “There needs to be a quick and devastating published take down of its premises”
The emails between Fauci and Collins are the smoking gun showing that it is they who are waging war against science
Despite having a combined annual budget of $58 billion, and a combined staff of 31,000, the U.S. Centers for Disease Control and Prevention and the NIH/NIAID have not yet conducted an actual study to determine how natural immunity stacks up against the COVID jab, likely because they don’t want to know the answer
The more we learn about Dr. Anthony Fauci, the worse he looks. The grandfatherly figurehead has now had two years in the limelight, urging people to “follow the science,” which he has shamelessly equated to his own ever-shifting opinion.
Another cache of emails obtained via a Freedom of Information Act (FOIA) request by the American Institute for Economic Research (AIER) now reveals Fauci and his boss, National Institutes of Health director Francis Collins, colluded behind the scenes to quash dissenting views on the lockdowns.1
Fauci and Collins Conspired to Destroy Dissent
October 4, 2020, three medical professors — Martin Kulldorff from Harvard, Sunetra Gupta from Oxford and Jay Bhattacharya from Stanford — launched the Great Barrington Declaration, a statement anyone could sign onto that called for focused protection of high-risk individuals, such as the elderly, rather than the continuation of blanket lockdowns. AIER sponsored the declaration.
“Current lockdown policies are producing devastating effects on short and long-term public health,” the declaration stated. “Keeping these measures in place until a vaccine is available will cause irreparable damage, with the underprivileged disproportionately harmed.”
As support of the declaration rapidly spread, Fauci and Collins seemingly panicked, and discussed how they could possibly stop the growing call for a sane, science-based approach. In an October 8, 2020, email to Fauci, Collins wrote:2,3,4,5
“The proposal from the three fringe epidemiologists who met with the Secretary seems to be getting a lot of attention … There needs to be a quick and devastating published take down of its premises …”
“Don’t worry, I got this,” Fauci replied. Later, Fauci sent Collins links to newly published articles refuting the focused protection solution, including an op-ed in Wired magazine, and an article in The Nation, titled “Focused Protection, Herd Immunity and Other Deadly Delusions.” “Excellent,” Collins replied.
This correspondence is a real peek behind the curtain as to who Fauci and Collins really are. They’re not interested in debating scientific merit. Their go-to strategy is simply to demolish the opposition by any means necessary.
Clearly, there’s nothing “fringe” about these scientists. Bhattacharya, for example, has conducted NIH-funded research for decades.6 If he’s a “fringe” scientist, why is Collins funding him?
As noted by Daniel McAdams of the Ron Paul Liberty Report (video above), behind the scenes, Fauci and Collins are just “nasty bureaucrats who want to destroy anyone who challenges their power … The scientific method does not involve, ‘Oh my gosh, that guy said something that contradicts me, I must destroy him.’”
Fauci’s War on Science
As noted by Jeffrey Tucker in a December 19, 2021, Brownstone article,7 the attacks on the declaration and its creators were particularly shocking considering “They were merely stating the consensus based on science and experience. Nothing more.”
Indeed, March 2, 2020, 850 scientists signed a letter8 to the White House warning against the use of lockdowns, travel restrictions and the closing of businesses and schools.
Fauci himself had even told a Washington Post reporter that “The epidemic will gradually decline and stop on its own without a vaccine”9 — a scientifically correct stance he’s since abandoned. According to Tucker, the emails between Fauci and Collins are the smoking gun showing that it is they who are waging war against science.
“What we find in these emails are highly political people who are obsessed not with science but with messaging and popular influences on the public mind,” Tuckerwrites.10
“What do we learn from these emails? The attacks on tens of thousands of medical professionals and scientists were indeed encouraged from the top. The basis for the attacks were not scientific articles. They were heavily political popular pieces.
This adds serious weight to the impression we all had at the time, which was that this was not really about science but about something far more insidious. You can discover more about this in Scott Atlas’s book on the topic [‘A Plague Upon Our House’]. These new emails confirm his account. It was an outright war on top scientists …
My own estimate is that the convinced advocates of lockdowns when they took place were probably fewer than 50 in the U.S. How and why they managed to grab hold of the reins of power will be investigated by historians for many decades.
The incredibly positive response to the Great Barrington Declaration, which has garnered 900,000 signatures in the meantime, demonstrates that there was and is still life remaining in traditional public health measures deployed throughout the 20th century and still respect for human dignity and science remaining among medical professionals and the general public.
This war on dissent against lockdowns is not only a scandal of our times. The lockdowns and now the mandates have fundamentally transformed society …
We seem ever more to be on the precipice of total disaster, one that will be difficult to reverse. It is urgent that we know who did this, as well as how and why, and take steps to stop it before more damage is done and then becomes permanent.”
Bhattacharya Speaks Out
When news of the Fauci-Collins collusion broke, Bhattacharya tweeted,11 “Now I know what it feels like to be the subject of a propaganda attack by my own government. Discussion and engagement would have been a better path.”
According to Bhattacharya, Collins and Fauci cooked up the false counternarrative that focused protection would “let the virus rip” through populations with devastating effect. This erroneous talking point was then thrown at them again and again.
“When reporters started asking me why I wanted to ‘let the virus rip,’ I was puzzled,”Bhattacharya tweeted December 19, 2021.12“Now I know that Collins and Fauci primed the media attack with the lie.
I was also puzzled by the mischaracterization of the GBD [Great Barrington Declaration] as a ‘herd immunity strategy,’ Biologically the epidemic ends when a sufficient number of people have immunity, either through COVID recovery or vax. Lockdown, let-it-rip, and the GBD all lead to that.
As Martin Kulldorff has said, it makes as much sense to say ‘herd immunity strategy’ as it does to say ‘gravity strategy’ for landing an airplane. The only question is how to land safely, not whether gravity applies.
So the question is how to get through this terrible pandemic with the least harm, where the harms considered include all of public health, not just COVID. The GBD and focused protection of the vulnerable is a middle ground between lockdown and let-it-rip.
Lockdowners like Collins & Fauci … could have engaged honestly in a discussion about it, but would have found that public health is fundamentally about focused protection … Instead, Fauci & Collins decided to smear Martin Kulldorff, Sunetra Gupta, me and supporters of the GBD. They lied about the ideas it contains and orchestrated a propaganda campaign against us …
Fauci & Collins are silent about lockdown harms because they are culpable. The sad fact is that they won the policy war, they got their lockdowns, and now … own the harms. They cannot deny it. The GBD warned them.
They also cannot say that the lockdowns worked to suppress COVID. In the U.S., we followed the Fauci/Collins lockdown strategy and we have 800k COVID deaths. Sweden — more focused on protecting the vulnerable — did better and cannot be ignored …
[History] will judge those in charge of the COVID policy, and it will not judge kindly. [Collins] smears the GBD and its authors because he has no substantive argument
left … Collins’ interview with Baier marks a sad end to an illustrious career, and I take no joy in saying so. Fauci should join him in retirement. They have done enough damage.”
Against Fading Odds, Fauci Tries to Keep Narrative Alive
The damaging character revelations emerge just as Fauci and President Biden struggle to whip up panic about Omicron to keep the need for pandemic countermeasures going. It’s a challenge, for sure, as most people have already realized that Omicron is no worse than a common cold.
During a December 19, 2021, CNN interview, Fauci stated that they “did not anticipate the extent of mutations” that occurred in Omicron.13 So, basically, despite sinking billions of dollars into research, scientists were unable to predict the mutations. That should tell us something.
Disturbingly, there’s now evidence suggesting Omicron might be yet another lab creation. In a recent Bannons War Room interview, Dr. Robert Malone, inventor of the mRNA and DNA vaccine core platform technology,14 reviewed what we know so far about the Omicron variant.
As noted by Malone, the press has been talking about “everything except for the obvious, which is that this is a ‘vaccine’-escaped mutant.’” The variant appears highly resistant to the COVID shots, which is a sign of it having mutated within one or more COVID-jabbed individuals, yet the first recommendation from the mental giants in charge of COVID responses was to push COVID booster shots. This is as irresponsible and irrational as it is unscientific.
“The boosters are a perfect way to bias our immune system so we’re LESS able to respond to this new variant,” Malone explained. “This is [like] jabbing everybody with a flu vaccine from three seasons ago and expecting it to have effects against the current [flu strains].”
Omicron Emerged From Old 2020 Strain
As for the nature and origin of Omicron, Malone said:
“It has the hallmark of a viral agent under tight genetic selection for evolution to escape the ‘vaccine’ responses against the receptor bonding domain. The question that is outstanding right now is — because this is so different from the other strains that are being tracked; it’s in its own separate little evolutionary branch — how did this happen?”
What Malone is referring to is the fact that the closest genetic sequences to Omicron date back to mid-2020. It doesn’t seem to belong to any of the evolutionary branches that have emerged since.15In the time-lapse graphic16 below, Twitter user Chief Nerd illustrates the genomic epidemiology of SARS-CoV-2 from the original strain until now, using data from nextstrain.org.17
It’s a great illustration of just how odd an unnatural Omicron’s emergence really is. As the time-lapse gets toward the end of 2021, suddenly there’s Omicron, emerging like a straight line from a mid-2020 strain, having no semblance to any of the other strains. There’s no precedent for this oddity occurring in nature.
In all, Omicron is said to have some 50 mutations from the original Alpha strain, many of which specifically allow it to circumvent COVID shot-induced antibody defenses.
According to molecular biologist and cancer geneticist Philip Buckhaults, Ph.D.,18 Omicron has 25 nonsynonymous and only one synonymous spike mutation compared to its most recent common ancestor (AV.1). Were it a natural occurrence, that ratio ought to be somewhere between 25 to 50 and 25 to 100.
Until and unless we end up with conclusive proof of its origin, we need to keep all options open, Malone says, and that includes the possibility of Omicron being cooked up in a lab from a previous strain.
One plausible theory is that scientists enabled an early SARS-CoV-2 variant to build antibody resistance, possibly by passaging them through human or humanized cell lines in the presence of convalescent plasma.
Congressman Calls for Natural Immunity Study
December 14, 2021, a Select Subcommittee on the Coronavirus Crisis held a remote hearing in which they debated the need for an accelerated vaccination effort. In the outtake from that meeting (video above), Congressman Jim Jordan, R-Ohio, points out that the U.S. Centers for Disease Control and Prevention and the NIH/NIAID have a combined annual budget of about $58 billion, and a combined staff of 31,000.
With that kind of budget and an army of staff, why has the U.S. government not done a study to determine how natural immunity stacks up against the COVID jab? Jordan asked. The answer he received (from an, unfortunately, unidentified doctor) was refreshingly direct:
“I don’t think they want to know the answer,” because “it would undermine the indiscriminate vaccination policy for every single human being, including extremely low risk people.”
According to a Columbia University study, more than half the American population have now been exposed to the SARS-CoV-2 virus in one form or another, and have natural immunity, and according to an Israeli study, natural immunity is 27 times more effective than the COVID shot.19
So, why are government leaders and so-called health authorities still acting as though natural immunity is irrelevant and the only way to control the pandemic is through repeated injections with experimental — and clearly hazardous — gene transfer technology?
I believe the answer is they’re ignoring natural immunity because their primary objective and goal it to have everyone injected. They want everyone routinely jabbed so they can justify the rollout of health passports, which will become the foundation for an all-encompassing digital ID control system.
In short, our public health agencies have been hijacked and are carrying out an anti-human, anti-health agenda intended to enslave the public in a technocratic control grid.
There’s no doubt anymore that the vaccine passports will be expanded to encompass financial transactions and incorporate a social credit system. Together, all of these pieces will allow an unelected elite to control the lives of every person on the planet, down to the minutest details of our everyday lives.
While Fauci and Collins are certainly not alone in this effort, and likely not even close to the top of the technocratic food chain, they have played very important roles. It’s time to see them for who and what they are, and demand that they be held to account for their actions.
A study published in the British Journal of Nutrition found an association between vitamin B12 deficiency and the incidence of depression in older people living in the community
Older adults with low levels had a 51% increased risk of developing depression during the study. Low levels of vitamin B12 may result from poor diet, or poor absorption related to lower levels of pepsin secretion that releases vitamin B12 from food
Other nutrient deficiencies are also associated with depression, including vitamin D and a low omega-3 index. Vitamin D deficiency may result from limited exposure to sunlight, inadequate absorption or poor conversion to the active form
Omega-3 fatty acids are essential for brain health, blood clotting, muscle activity and more. The omega-3 index is lowest in North America, Europe, Central and South America, Africa and the Middle East. Deficiency contributes to mood disorders, including depression
Research published in December 20211 using data from the Irish Longitudinal Study on Aging (TILDA) discovered those with a vitamin B12 deficiency had a greater risk of symptoms of depression. According to the Anxiety and Depression Association of America,2 264 million people worldwide live with symptoms of depression. In 2017, roughly 17.3 million adults in the U.S. had experienced at least one major depressive episode.
This number rose in 2019 to 19.4 million adults who had experienced at least one major depressive episode.3 It is not uncommon for someone who has depression to also suffer from symptoms of anxiety.4 According to the CDC,5 data from the National Health and Nutrition Examination Survey show women are roughly twice as likely to experience depression as men, which was a pattern that was observed in each age group surveyed.
Symptoms of depression can include feeling sad or empty, hopeless, irritable, worthless and restless. You may have difficulty sleeping, experience appetite or weight changes or have thoughts of death or suicide. Not everyone experiences every symptom. For some individuals, their symptoms make it difficult to function.6
The December 2021 study linked deficiencies in vitamin B12 with the incidence of symptoms of depression in the elderly. Vitamin B12 is a water-soluble vitamin found in some foods.7 It’s also available as a prescription medication and dietary supplement. Your body uses vitamin B12 for the function and myelination of the central nervous system, to form healthy red blood cells and in DNA synthesis.
Food sources include those of animal origin, such as pasture-raised poultry, dairy products, eggs and meat. Absorption of vitamin B12 is dependent on intrinsic factor, which is a transport and delivery binding protein produced in the stomach.8 The bioavailability from food decreases when the amount of vitamin B12 exceeds the capacity of intrinsic factor.
Vitamin B12 is released from food by the activity of hydrochloric acid and gastric protease in the stomach and saliva in the mouth.9 In 1999 it was estimated10 that vitamin B12 deficiency affects up to 15% of people over age 60. In this study, however, classic symptoms of deficiency were often lacking in this population.
The low vitamin B status is attributed to the high prevalence of atrophic gastritis which results in low-acid pepsin secretion and reduces the release of vitamin B12 from food. The 2021 study finds these low levels of vitamin B12 may increase the risk of depression in older adults.11
Vitamin B12 Deficiency Associated With Depression
The study published in the British Journal of Nutrition12 sought to evaluate the relationship between vitamin B12, folate and the incidence of depression in older individuals living in the community. There were 3,849 individuals over age 50 included.
The results showed a link between vitamin B12 deficiency, but not with a folate deficiency.13 The researchers found that even after controlling for factors such as chronic disease, cardiovascular disease, antidepressant use, physical activity and vitamin D status, the results remain significant.14
The older adults who had a B12 deficiency had a 51% increased risk of developing symptoms of depression during the four years of the study. The data also showed that certain factors influenced the vitamin B12 status in older adults. This included geographic location, obesity, smoking, socioeconomic status and gender.
While the link was found between older adults living in the community and a vitamin B12 deficiency, they also found that older individuals in the study had a lower risk of depression. In a press release from Trinity College Dublin, Eamon Laird, from TILDA15 and lead scientist of the study talked about the results in a press release, saying:16
“This study is highly relevant given the high prevalence of incident depression in older adults living in Ireland, and especially following evidence to show that one in eight older adults report high levels of low B12 deficiency rates.
There is a growing momentum to introduce a mandatory food fortification policy of B-vitamins in Europe and the UK, especially since mandatory food fortification with folic acid in the US has showed positive results, with folate deficiency or low status rates of just 1.2% in those aged 60 years and older.”
Vitamin D Deficiency Plays a Role in Mental Health
This recent study highlights the importance of adequate nutrition to protect your optimal health. In addition to vitamin B12, other nutrients have a significant effect on mental health. Vitamin D is one of those nutrients. Vitamin D, also known as calciferol,17 is a fat-soluble vitamin, which your body can absorb from a few foods and produces endogenously when exposed to sunlight.
People can become deficient when they consume less than the recommended level, have limited exposure to sunlight, their absorption from the digestive tract is inadequate, or the kidneys do not convert the vitamin to its active form. Scientists believe that vitamin D deficiency is a vastly overlooked global health problem at epidemic proportions.18
How vitamin D deficiency is defined also varies. For the most part, researchers interpret vitamin D deficiency as serum levels of 25(OH)D at 20 nanograms per milliliter (ng/mL) or less.19 However, optimal serum levels of vitamin D are between 40 ng/mL and 60 ng/mL.20
Early research in 200021 demonstrated there were significantly deficient levels of vitamin D3 in patients who suffered from depression and alcohol addiction. By 2007, researchers had recognized the importance of low levels of vitamin D on mood.22
Further research23 found individuals with fibromyalgia also had a higher risk of low serum levels of vitamin D and it appeared that supplementing with high doses of vitamin D in individuals who were depressed and overweight could ameliorate the symptoms.24 Over the years, researchers continue to ask the question if vitamin D is a causal association with depression or another symptom of the condition.25
Other scientists postulated whether an effective therapy for depression would be the detection and treatment of vitamin D deficiency.26 By 2014,27 one study found hypovitaminosis D was associated with the severity of depression that people experienced. Their results suggested there was an inverse associated dose-response, which implied that low levels of vitamin D may be an underlying biological vulnerability.
In 2018,28 the British Journal of Psychiatry published a systematic review and meta-analysis that demonstrated low levels of vitamin D are associated with depression. The important factor to remember is that it’s highly unlikely supplementation in people whose serum levels are optimal will have any effect on mood disorders. Instead, the effect is more likely to be found in those whose serum levels are low.
Relevance of Omega-3 Fatty Acids for Depression
Omega-3 fats are essential polyunsaturated fatty acids (PUFAs), which your body needs for a variety of functions. These include digestion, blood clotting, brain health and muscle activity. In early 2021, omega-3 fats made the news when data29 revealed individuals with an omega-3 index measuring 5.7% or greater had significantly better outcomes from COVID-19.
An omega-3 index measures the amount on the red blood cell membranes.30 Those with a measurement less than 4% have a higher risk of heart disease. Individuals with an omega index between 4% and 8% have an intermediate risk and those whose level is greater than 8% are at low risk of heart disease.
One 2016 published analysis of the data31 revealed there were areas of the world with omega-3 index measurements greater than 8%. These included Scandinavia, Sea of Japan and indigenous populations who did not eat westernized foods. Areas of the world with levels below 4% included Central and South America, Europe, North America, the Middle East, Southeast Asia and Africa.
While your level of omega-3 is important, equally as important is the ratio between omega-6 and omega-3. I have found it extremely difficult to correct an imbalance by simply taking more omega-3 fats. In fact, just as an excessive amount of omega-6 is dangerous, an excessive amount of omega-3 can also contribute to ill-health.
The imbalance between omega 6 and omega 3 that occurred in the last 150 years is thought to be behind many of the inflammatory-related diseases common in society, including depressive disorders.32 Increasing evidence suggests that a deficiency in omega-3 fats contribute to mood disorders, including depression.33,34,35
Increased Risk in Elderly of Deficiencies and Depression
Vitamin D,36 B1237 and omega-3 fats are common deficiencies found in the general population and older adults. The reason older adults may have nutrient deficiencies is likely related to poor absorption, poor diet and lack of exposure to sunlight.
A lack of optimal levels of nutrients is a significant contributor to the development of inflammation and disease, and one of the health conditions associated with inflammation is depression.38Depression affects the quality of life and productivity in the elderly, at a time when they are often more isolated from others.
To date, many older adults are treated for depression using psychotherapy and/or medications. However, since there is a significant link between nutrition and mood, it only makes sense to first address the potential nutrient deficiencies before adding medications that come with a long list of side effects.
One of the more common classes of antidepressants, selective serotonin reuptake inhibitors (SSRIs),39 may trigger nausea, dizziness, insomnia, anxiety, diarrhea and tremors,40 all of which can be dangerous for older adults. These side effects can negatively impact intake or increase the risk of a fall.
As has been demonstrated during the COVID-19 pandemic, maintaining optimal health and nutrition helps to reduce your risk of contracting a viral illness. The featured study also demonstrates that nutrient intake is crucial to your mental health. It is much easier to address bodily needs before they trigger illness and disease. Although it may take a little time and energy, it is vital for your quality of life to take control of your health.
Japan has taken steps to warn its citizens about serious side effects linked to COVID-19 injections
They’ve added a warning label to the jabs, warning about the risk of myocarditis — inflammation of the heart muscle
Japan is also taking strict measures to monitor and report all side effects to the unprecedented jabs
Hospitals must report, in detail, any adverse effects that occur within 28 days of receiving a COVID-19 injection
Japan’s Ministry of Health includes a “consent to vaccination” section on its website, which states mandatory vaccination and discrimination against those who choose not to be vaccinated are not advised; this includes at workplaces, which are told not to force anyone to get injected
Japan is standing out as a protector of informed consent and medical freedom, during a time in history when many other countries are opting for totalitarian control
Japan has taken steps to warn its citizens about serious side effects linked to COVID-19 injections.1They’ve added a label to the jabs, warning about the risk of myocarditis — inflammation2 of the heart muscle that can cause symptoms similar to a heart attack, including chest pain, shortness of breath, abnormal heartbeat and fatigue.
The U.S. Centers for Disease Control and Prevention states on their website, “Myocarditis and pericarditis have rarely been reported, especially in adolescents and young adult males within several days after COVID-19 vaccination.”3
Further, in June 2021, the U.S. Food and Drug Administration added a warning to patient and provider fact sheets for the Pfizer and Moderna jabs about the “suggested increased risks of myocarditis (inflammation of the heart muscle) and pericarditis (inflammation of the tissue surrounding the heart) following vaccination.”4
Unlike in the U.S., however, Japan is taking measures to monitor and report all side effects to the unprecedented jabs.
Japan Has Strict Reporting Requirements for Jab Side Effects
In Japan, strict legal reporting requirements are in effect for side effects that occur within 28 days of receiving a COVID-19 injection. Hospitals must report, in detail, any adverse effects that occur within that time period.
Japan’s Ministry of Health reported that, as of November 14, 2021, for every 1 million males who received the Moderna COVID-19 injection, 81.79 youths between the ages of 10 and 19 developed myocarditis or pericarditis, as did 48.76 men in their 20s.5
For Pfizer’s COVID-19 jab, 15.66 out of every 1 million 10- to 19-year-old males who received the jab suffered from myocarditis or pericarditis, along with 13.32 of males in their 20s.6 Due to the risk of myocarditis, Britain’s Joint Committee on Vaccination and Immunization (JCVI) recommended against COVID-9 injections for healthy 12- to 15-year-olds. JCVI member Adam Finn told Reuters:7
“… the number of serious cases that we see of COVID in children this age are really very small. There are uncertainties about the long-term implications of (myocarditis), and that makes the risk-benefit balance for these children really quite tight and much tighter than we would be comfortable to make the recommendation.”
In the U.S., where COVID-19 injections are recommended for ages 5 and up, the CDC stated it is “conducting surveys of patients (or their parents or guardians) and health care providers to gather information about myocarditis after mRNA COVID-19 vaccination” and “contacting people who meet the case definition for myocarditis following mRNA COVID-19 vaccination.”8
As of December 8, 2021, 1,908 reports of myocarditis or pericarditis had been reported to the Vaccine Adverse Event Reporting System (VAERS) following COVID-19 jabs, typically among male adolescents and young adults.9 December 17, 2021, just 51 days after approving the shots for children ages 5 to 11, the CDC reported10 that it had so far received reports of eight cases of myocarditis in that age group.
Past investigations have shown only between 1%11 and 10%12 of adverse reactions are ever reported to VAERS, which is a passive, voluntary reporting system, so the actual number could be much higher.
In its approval letter for Comirnaty (Pfizer’s COVID-19 injection), the FDA ordered Pfizer to conduct research to investigate the risk of inflammation in and around the heart, as voluntary reporting mechanisms are insufficient.13
The FDA accepted Pfizer’s suggested timetable for the post-approval study to evaluate incidence of heart and heart sack inflammation, which includes the submission of an interim report at the end of October 2023, a study completion date of June 30, 2025, and submission of a final report October 31, 2025.
Japan Says No to Vaccine Mandates, Discrimination
In stark contrast to much of the rest of the globe, Japan stands against compulsory vaccination. Japan’s Ministry of Health includes a “consent to vaccination” section on its website, which states mandatory vaccination and discrimination against those who choose not to be vaccinated are not advised. This includes at workplaces, which are told not to force anyone to get injected:14,15
“Although we encourage all citizens to receive the COVID-19 vaccination, it is not compulsory or mandatory. Vaccination will be given only with the consent of the person to be vaccinated after the information provided.
Please get vaccinated of your own decision, understanding both the effectiveness in preventing infectious diseases and the risk of side effects. No vaccination will be given without consent. Please do not force anyone in your workplace or those who around you to be vaccinated, and do not discriminate against those who have not been vaccinated.”
The page even links to “human rights counseling in foreign languages,” which details what to do if faced with vaccine discrimination in the workplace.16 Japan is standing out as a protector of informed consent and medical freedom, during a time in history when many other countries are opting for totalitarian control. Rair Foundation explained:17
“Doctors worldwide have echoed Japan’s health authority warnings about the gene-therapies side effects. However, this kind of proper informed consent has cost many doctors in western nations their licenses to practice medicine. The government has accused these doctors of spreading ‘vaccine hesitancy.’
Furthermore, while Japan allows its citizens to choose whether to be injected with the experimental gene-therapies, other countries are forcing citizens to receive the jab. For example, in February 2022, Austria will mandate the injections. Citizens who refuse will face heavy fines and up to one year in prison.”
Japanese Researchers Warn of Blood Clots, Death After Jabs
Reports of both cerebral venous sinus thrombosis and intracranial hemorrhage (ICH) have been reported following COVID-19 shots, including both fatal and nonfatal cases. In a commentary published in the Journal of Pharmaceutical Policy and Practice,18 Japanese researchers revealed that, as of May 2021, 10 deaths were reported following the shots — and the manner of deaths raised a red flag.
Among the five men who died, it was from causes other than stroke, but four of the five women who passed away died from ICH. “This imbalance is incompatible with the mortality data on cardiovascular diseases in the National Statistics, which show no apparent disparity between sexes or between hemorrhagic and ischemic stroke,” they wrote.19
Their analysis revealed “a disproportionately high incidence of death by ICH in Japanese women who received tozinameran [Pfizer’s COVID0-19 shot], suggesting a potential association of ICH with the vaccine.”20 They also believe that a causal link between the deaths from ICH and the shot is possible and warrants further study. Others have also warned that blood clot formation with mRNA vaccines is inevitable.
The mRNA COVID-19 injections affect your body at the cellular level.21 In each dose of the Moderna COVID-19 shot are 40 trillion mRNA — or messenger RNA — molecules. Each mRNA “package” is designed to be absorbed into your cell, but only 25% stay in your arm at the site of the injection. The other 75%, is collected by your lymphatic system and fed into your circulation, Dr. Charles Hoffe, a family physician from Lytton, British Columbia, said.
The cells where mRNA is absorbed are those around your blood vessels — the capillary network, which are the tiniest blood vessels in your body. When the mRNA is absorbed into your vascular endothelium — the inner lining of your capillaries — the “packages” open and genes are released. Each gene can produce many COVID-19 spike proteins, and your body gets to work manufacturing these spike proteins, numbering in the trillions.
Your body recognizes the spike protein as foreign, so it begins to manufacture antibodies to protect you against COVID-19, or so the theory goes. But there’s a problem. In a coronavirus, the spike protein becomes part of the viral capsule, Hoffe says, but when you get the shot, “it’s not in a virus, it’s in your cells.” The spike protein, in turn, can lead to the development of blood clots:22
“So it therefore becomes part of the cell wall of your vascular endothelium, which means that these cells, which line your blood vessels, which are supposed to be smooth so that your blood flows smoothly now have these little spiky bits sticking out.
So it is absolutely inevitable that blood clots will form, because your blood platelets circulate around in your vessels and the purpose of blood platelets is to detect a damaged vessel and block that damage when it starts bleeding. So when a platelet comes through a capillary and suddenly hits all these covid spikes that are jutting into the inside vessel … blood clots will form to block that vessel. That’s how platelets work.”
Japanese Study Reveals Adverse Events Following Jabs
In a preprint study released in October 2021, researchers from Nagasaki International University, Japan, studied adverse events that occur in young Japanese people following Moderna’s COVID-19 shot.23
Using data from 7,965 individuals, they found that 83% experienced local adverse events while 65% experienced systemic adverse events. Those particularly at risk included women, youth under the age of 20 — who often experienced adverse events after the first dose — and those who experienced adverse events after the first dose.
Such information is crucial to proper informed consent, something that not only has been lacking during the pandemic, but actively censored. It’s encouraging to see countries like Japan standing out in their efforts to get a true picture of how dangerous COVID-19 jabs may be. As Health Thoroughfare noted:24
“According to the latest reports, the country is reaffirming its commitment to adverse event reporting requirements to ensure all possible side effects are documented. These efforts from Japan’s health authority are in stark contrast to the measures taken by other countries to coerce citizens into taking the injection, downplaying side effects, and discouraging proper adverse event reporting.”
The COVID shots reprogram your immune system to respond in a dysfunctional manner. Aside from increasing vulnerability to infections, this can also result in autoimmune diseases and cancer
A paper published in early May 2021 reported the Pfizer/BioNTech COVID jab “reprograms both adaptive and innate immune responses,” causing immune depletion
Antigens in vaccines have been shown to induce defects in the immune system that can raise the risk of autoimmune diseases
Leaky or nonsterilizing vaccines can also trigger the evolution of more hazardous viruses, and the COVID jabs are among the leakiest “vaccines” ever created
According to health authorities, the vaccine-evading Omicron variant necessitates a third COVID injection, but this recommendation will only perpetuate mutation
A number of medical experts, scientists and published studies now warn that the COVID shots reprogram your immune system to respond in a dysfunctional manner. Aside from increasing vulnerability to infections, this can also result in autoimmune diseases and cancer.
Pfizer Shot Reprograms Both Arms of Your Immune System
A paper1 posted May 6, 2021, on the preprint server medRxiv reported that the Pfizer/BioNTech COVID jab “reprograms both adaptive and innate immune responses,” causing immune depletion.
While they confirmed the jab “induced effective humoral and cellular immunity against several SARS-CoV-2 variants,” the shot “also modulated the production of inflammatory cytokines by innate immune cells upon stimulation with both specific (SARS-CoV-2) and nonspecific (viral, fungal and bacterial) stimuli.”
In other words, we’re looking at a horrible tradeoff. You may get some protection against SARS-CoV-2 and its variants, but you’re weakening your overall immune function, which opens the door wide to all sorts of other health problems, from bacterial, fungal and viral infections to cancer and autoimmunity.
After the injection, innate immune cells had a markedly decreased response to toll-like receptors 4, 7 and 8 (TLR4, TLR7, TLR8) ligands, while cytokine responses induced by fungi were stronger. According to the authors, defects in TLR7 have previously been linked to an increased susceptibility to COVID-19 in young males.
People who were “fully vaccinated,” having received two doses of the Pfizer shot, also produced significantly less interferon upon stimulation, and this can hamper the initial innate immune response against the virus.
Repeated Vaccinations and the Risk of Autoimmunity
Pathogenic infections and cancer are but two potential outcomes of this kind of reprogramming. Previous research, for example, has linked defects in the immune system to a higher risk of autoimmune diseases. What’s more, it’s been shown that antigens in vaccines, specifically, can induce this kind of immune system dysfunction.2 As reported in the paper in question:3
“Repeated immunization with antigen causes systemic autoimmunity in mice otherwise not prone to spontaneous autoimmune diseases. Overstimulation of CD4+ T cells led to the development of autoantibody-inducing CD4+ T (aiCD4+ T) cell which had undergone T cell receptor (TCR) revision and was capable of inducing autoantibodies.
The aiCD4+ T cell was induced by de novo TCR revision but not by cross-reaction, and subsequently overstimulated CD8+ T cells, driving them to become antigen-specific cytotoxic T lymphocytes (CTL).
These CTLs could be further matured by antigen cross-presentation, after which they caused autoimmune tissue injury akin to systemic lupus erythematosus (SLE). Systemic autoimmunity appears to be the inevitable consequence of over-stimulating the host’s immune ‘system’ by repeated immunization with antigen, to the levels that surpass system’s self-organized criticality.”
Fast-forward to mid-May 2021, when a study4 in the Journal of Clinical Investigations reported that “SARS-CoV-2 mRNA vaccines induce broad CD4+ T cell responses that recognize SARS-CoV-2 variants and HCoV-NL63.” HCoV-NL63 is a human coronavirus associated with the common cold.
“Interestingly, we observed a 3-fold increase in the CD4+ T cell responses to HCoV-NL63 spike peptides after vaccination,” the authors stated, adding, “Our results suggest that T cell responses elicited or enhanced by SARS-CoV-2 mRNA vaccines may be able to control SARS-CoV-2 variants and lead to cross-protection against some endemic coronaviruses.”
What they did not address was that excessive CD4a+ T cell responses could also result in the development of autoantibodies and autoimmune disease.
COVID Shots May Also Cause More Hazardous Variants
We’ve long known that leaky or nonsterilizing vaccines can trigger the evolution of more hazardous viruses.5,6,7,8 So far, SARS-CoV-2 variants have mutated into less dangerous versions, which is fortunate, but the risk of the COVID shots creating a “monster” still remains.
In a February 9, 2021, article,9 NPR highlighted this risk, stating that “vaccines could drive the evolution of more COVID-19 mutants.” According to NPR science correspondent Richard Harris, “the virus is always mutating. And if one happens to produce a mutation that makes it less vulnerable to the vaccine, that virus could simply multiply in a vaccinated individual.”
The Omicron variant appears to have significant resistance against antibodies produced by the original COVID shots, which is why Omicron infection is being primarily reported in those who have received the injections.
In 2018, Quanta Magazine detailed how vaccines drive the evolution of pathogens.10 I’ve referenced that article on previous occasions, as have many others. In response, the editor of Quanta Magazine added a “disclaimer” dated December 6, 2021, to the article, stating:
“This article from 2018 discusses how leaky vaccines — vaccines that do not reduce viral replication or transmission to others — can drive the pathogens they target to evolve and become more virulent. These concerns do not apply to COVID-19 vaccines, because COVID-19 vaccines significantly reduce coronavirus replication and transmission, reducing the chance that mutations occur and variants arise …”
That statement is clearly false, as studies have repeatedly shown the COVID shots are in fact leaky. They do not “significantly reduce” viral replication or transmission, as the editor claims. Quite the opposite.
People who have received one or more COVID shots have been found to harbor higher viral loads than the unvaccinated, and Israel (which appears to have the best tracking and monitoring) reports that the worst COVID cases are in those who are fully vaxxed.
December 6, 2021, Newsweek11 reported a COVID outbreak among “fully vaccinated” hospital staff in Spain. After a Christmas dinner with more than 170 fully vaxxed health care workers in attendance, nearly 70 of them tested positive for COVID. Some reported mild symptoms. Daniel Horowitz pointed out the editor’s false note in a December 9, 2021, Blaze post:12
“Leaky vaccines are worse than no vaccine at all. That is the unmistakable conclusion one would derive from a May 2018 article in Quanta magazine, a top scientific publication, about the unsuccessful attempts to create vaccines for HIV, malaria, and anthrax that aren’t leaky and don’t run the risk of making the pathogens more dangerous.
Yet now that we are seeing such a microbiological Frankenstein play out in real life and people like Dr. Robert Malone have been citing this article to raise red flags about the leaky COVID shots, Quanta magazine took the unprecedented step of slapping an editor’s note on an article three and a half years later to get people to stop applying it to the leakiest vaccine of all time.”
COVID Shots Stop Working Within a Few Months
A study in the New England Journal of Medicine, published December 9, 2021, also confirms that whatever protection you get from the Pfizer COVID shot is short in duration. As explained by the authors:13
“In December 2020, Israel began a mass vaccination campaign against coronavirus disease 2019 (Covid-19) by administering the BNT162b2 vaccine, which led to a sharp curtailing of the outbreak.
After a period with almost no cases of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection, a resurgent Covid-19 outbreak began in mid-June 2021. Possible reasons for the resurgence were reduced vaccine effectiveness against the delta (B.1.617.2) variant and waning immunity.
We used data on confirmed infection and severe disease collected from an Israeli national database for the period of July 11 to 31, 2021, for all Israeli residents who had been fully vaccinated before June 2021.
We used a Poisson regression model to compare rates of confirmed SARS-CoV-2 infection and severe Covid-19 among persons vaccinated during different time periods, with stratification according to age group and with adjustment for possible confounding factors.
Among persons 60 years of age or older, the rate of infection in the July 11-31 period was higher among persons who became fully vaccinated in January 2021 (when they were first eligible) than among those fully vaccinated 2 months later, in March (rate ratio, 1.6 …)
Among persons 40 to 59 years of age, the rate ratio for infection among those fully vaccinated in February (when they were first eligible), as compared with 2 months later, in April, was 1.7 … Among persons 16 to 39 years of age, the rate ratio for infection among those fully vaccinated in March (when they were first eligible), as compared with 2 months later, in May, was 1.6 …
The rate ratio for severe disease among persons fully vaccinated in the month when they were first eligible, as compared with those fully vaccinated in March, was 1.8 … among persons 60 years of age or older and 2.2 … among those 40 to 59 years of age …
These findings indicate that immunity against the delta variant of SARS-CoV-2 waned in all age groups a few months after receipt of the second dose of vaccine.”
Two Doses Aren’t Enough
Earlier this year, vaccine makers and health authorities said the shots were about 95% effective and if enough people got the shots, normalcy would be restored. We now know that was a false promise. The goal post was moved back with the emergence of Delta and then Omicron, for which we’re now told we need a third booster.
December 13, 2021, Reuters14 reported that British scientists have concluded “two-dose COVID-19 vaccine regimens do not induce enough neutralizing antibodies against the Omicron coronavirus variant,” and that “increased infections in those previously infected or vaccinated may be likely.”
‘Just Deal With’ Booster Shots, Fauci Says
When in mid-December 2021, Dr. Anthony Fauci was asked if Americans should expect annual COVID boosters, he replied in the affirmative, saying that Americans will “just have to deal with” the prospect of getting boosters at regular intervals.15 So, in essence, Fauci wants us to accept that booster deficiency is the reason why the COVID-19 “pandemic” continues.
Clearly, that is not the case. The real reason COVID is still an issue is because Fauci and the medical establishment have suppressed viable early treatments. If early treatment was the norm, COVID would rapidly become a distant memory.
Instead, the captured U.S. Food and Drug Administration granted emergency use authorization to novel gene transfer technologies that don’t work like conventional vaccines in that they don’t prevent infection and spread, thus creating an evil cycle of new vaccine-resistant variants. As demonstrated by James Lyons-Weiler (in a now broken weblink), the more we vaccinate, the higher the COVID caseload.
Weiler’s graph looks very much like that in a September 30, 2021, study16 in the European Journal of Epidemiology, which found that the higher the vaccination rate in a given area, the higher the COVID case rate.
Dr. Chris Martenson discusses this finding in the video below. As noted by Martenson, “the line goes the wrong way,” meaning the more heavily “vaccinated” a population is, the worse things get.
“No Discernable Relationship” between Vaccines and Cases
As predicted over a year ago, we’re now on an injection treadmill with no end in sight, and every single dose carries the risk of serious side effects, up to and including permanent disability and death. The only scientifically sound way out of this failed experiment is to stop. No more boosters.
Fortunately, it seems most Americans are starting to catch on, and so far, the fearmongering around Omicron has not resulted in a rush for boosters.17 According to an Axios/Ipsos poll conducted December 10 through December 13, 2021, 67% of unvaccinated respondents said Omicron makes no difference in their decision of whether to get vaccinated; 19% said it makes them more likely while 11% said it makes them less likely to get the shot.
Among respondents who already had received one or two doses, 59% said Omicron makes no difference in their decision to get a third dose; 36% said it makes them more likely and 5% said it makes them less likely to get it.
Considering the shots have been shown to deregulate your immune function, it would be wise to “just say no” to further boosters. Should you develop symptoms of SARS-CoV-2 infection, remember there are safe and effective early treatment protocols, including the I-MASK+18 and I-MATH+,19protocols, which are available for download on the COVID Critical Care website in multiple languages. Other protocols that have great success are:
This is a load of information to review, especially if you are fatigued and sick with COVID or have a family member struggling. After reviewing all of these protocols, I believe the Front Line COVID-19 Critical Care Alliance’s protocol is among the easiest to follow. Below is a summary of that protocol, with minor amendments.
A visionary whose discoveries have treated numerous diseases. A global finance expert. A man who has brought powerful white-collar criminals to justice and invented life-changing medical technologies. These all describe my guest today: Dr. David Martin, PhD.
Why does this man who has worked so closely with Congress think that COVID-19 wasn’t a freak act of nature or lab leak, but a plot years in the making? What criminal patterns has he seen before that are showing themselves again on the world stage?
But most importantly of all, I want to ask him the question on everyone’s minds: Why is President Trump continuing to push the vaccine even as people keep having adverse reactions? What’s really going on?
Join Man in America for an interview you won’t want to miss: 12/23, 2:00 PM ET.
Ivermectin trials put on hold in the UK because of supply issues? That’s not even how these studies work. Dr. Malone exposes the truth – the insidious nature of big pharma again.
Merck cites probability issues, but we all know it’s profit…
This text is a written summary of Dr. Bhakdi’s and Dr. Burkhardt’s presentations at the Doctors for COVID Ethics symposium that was live-streamed by UKColumnon December 10th, 2021. The two presentations can be viewed at the very beginning of the video recording of the symposium.
The authors
Dr. Bhakdi has spent his life practicing, teaching and researching medical microbiology and infectious diseases. He chaired the Institute of Medical Microbiology and Hygiene at the Johannes Gutenberg Unversity of Mainz, Germany, from 1990 until his retirement in 2012. He has published over 300 research articles in the fields of immunology, bacteriology, virology and parasitology, and served from 1990 to 2012 as Editor-in-Chief of Medical Microbiology and Immunology, one of the first scientific journals of this field that was founded by Robert Koch in 1887.
Dr. Arne Burkhardt is a pathologist who has taught at the Universities of Hamburg, Berne and Tübingen. He was invited for visiting professorships/study visits in Japan (Nihon University), the United States (Brookhaven National Institute), Korea, Sweden, Malaysia and Turkey. He headed the Institute of Pathology in Reutlingen for 18 years. Subsquently, he worked as an independent practicing pathologist with consulting contracts with laboratories in the US. Burkhardt has published more than 150 scientific articles in German and international scientific journals as well as contributions to handbooks in German, English and Japanese. Over many years he has audited and certified institutes of pathology in Germany.
The evidence
We herewith present scientific evidence that calls for an immediate stop of the use of gene-based COVID-19 vaccines. We first lay out why the agents cannot protect against viral infection. While no positive effects can be expected, we show that the vaccines can trigger self-destructive processes that lead to debilitating illness and death.
Why the vaccines cannot protect against infection
A fundamental mistake underlying the development of the COVID-19 vaccines was to neglect the functional distinction between the two major categories of antibodies which the body produces in order to protect itself from pathogenic microbes.
The first category (secretory IgA) is produced by immune cells (lymphocytes) which are located directly underneath the mucous membranes that line the respiratory and intestinal tract. The antibodies produced by these lymphocytes are secreted through and to the surface of the mucous membranes. These antibodies are thus on site to meet air-borne viruses, and they may be able to prevent viral binding and infection of the cells.
The second category of antibodies (IgG and circulating IgA) occur in the bloodstream. These antibodies protect the internal organs of the body from infectious agents that try to spread via the bloodstream.
Vaccines that are injected into the muscle – i.e., the interior of the body – will only induce IgG and circulating IgA, not secretory IgA. Such antibodies cannot and will not effectively protect the mucous membranes from infection by SARS-CoV-2. Thus, the currently observed “breakthrough infections” among vaccinated individuals merely confirm the fundamental design flaws of the vaccines. Measurements of antibodies in the blood can never yield any information on the true status of immunity against infection of the respiratory tract.
The inability of vaccine-induced antibodies to prevent coronavirus infections has been reported in recent scientific publications.
The vaccines can trigger self-destruction
A natural infection with SARS-CoV-2 (coronavirus) will in most individuals remain localized to the respiratory tract. In contrast, the vaccines cause cells deep inside our body to express the viral spike protein, which they were never meant to do by nature. Any cell which expresses this foreign antigen will come under attack by the immune system, which will involve both IgG antibodies and cytotoxic T-lymphocytes. This may occur in any organ. We are seeing now that the heart is affected in many young people, leading to myocarditis or even sudden cardiac arrest and death. How and why such tragedies might causally be linked to vaccination has remained a matter of conjecture because scientific evidence has been lacking. This situation has now been rectified.
Histopathologic studies: the patients
Histopathologic analyses have been performed on the organs of 15 persons who died after vaccination. The age, gender, vaccination record, and time of death after injection of each patient are listed in the table on the next page. The following points are of utmost importance:
Prior to death, only 4 of the 15 patients had been treated in the ICU for more than 2 days. The majority were never hospitalized and died at home (5), on the street (1), at work (1), in the car (1), or in home-care facilities (1). Therefore, in most cases, therapeutic intervention is unlikely to have significantly influenced the post-mortem findings.
Not a single death was brought into any possible association with the vaccination by the coroner or the public prosecutor; this association was only established by our autopsy findings.
The initially performed conventional post-mortems also uncovered no obvious hints to a possible role of vaccination, since the macroscopic appearance of the organs was overall unremarkable. In most cases, “rhythmogenic heart failure” was postulated as the cause of death.
But our subsequent histopathological analyses then brought about a complete turnaround. A summary of the fundamental findings follows.
Case #
Gender
Age (years)
Vaccine (injections)
Time of death after last injection
1
female
82
Moderna (1. and 2.)
37 days
2
male
72
Pfizer (1.)
31 days
3
female
95
Moderna (1. and 2.)
68 days
4
female
73
Pfizer (1.)
unknown
5
male
54
Janssen (1.)
65 days
6
female
55
Pfizer (1. and 2.)
11 days
7
male
56
Pfizer (1. and 2.)
8 days
8
male
80
Pfizer (1. and 2.)
37 days
9
female
89
Unknown (1. and 2.)
6 months
10
female
81
Unknown (1. and 2.)
unknown
11
male
64
AstraZeneca (1. and 2.)
7 days
12
female
71
Pfizer (1. and 2.)
20 days
13
male
28
AstraZeneca (1.), Pfizer (2.)
4 weeks
14
male
78
Pfizer (1. and 2.)
65 days
15
female
60
Pfizer (1.)
23 days
Histopathologic studies: findings
Histopathologic findings of a similar nature were detected in organs of 14 of the 15 deceased. Most frequently afflicted were the heart (14 of 15 cases) and the lung (13 of 15 cases). Pathologic alterations were furthermore observed in the liver (2 cases), thyroid gland (Hashimoto’s thyroiditis, 2 cases), salivary glands (Sjögren`s Syndrome; 2 cases) and brain (2 cases).
A number of salient aspects dominated in all affected tissues of all cases:
inflammatory events in small blood vessels (endothelitis), characterized by an abundance of T-lymphocytes and sequestered, dead endothelial cells within the vessel lumen;
the extensive perivascular accumulation of T-lymphocytes;
a massive lymphocytic infiltration of surrounding non-lymphatic organs or tissue with T-lymphocytes.
Lymphocytic infiltration occasionally occurred in combination with intense lymphocytic activation and follicle formation. Where these were present, they were usually accompanied by tissue destruction.
This combination of multifocal, T-lymphocyte-dominated pathology that clearly reflects the process of immunological self-attack is without precedent. Because vaccination was the single common denominator between all cases, there can be no doubt that it was the trigger of self-destruction in these deceased individuals.
Conclusion
Histopathologic analysis show clear evidence of vaccine-induced autoimmune-like pathology in multiple organs. That myriad adverse events deriving from such auto-attack processes must be expected to very frequently occur in all individuals, particularly following booster injections, is self-evident.
Beyond any doubt, injection of gene-based COVID-19 vaccines places lives under threat of illness and death. We note that both mRNA and vector-based vaccines are represented among these cases, as are all four major manufacturers.
If you had COVID-19 or received a COVID-19 injection, you may have dangerous spike proteins circulating in your body
Spike proteins can circulate in your body after infection or injection, causing damage to cells, tissues and organs
The World Council for Health has released a spike protein detox guide, which provides straightforward steps you can take to potentially lessen the effects of toxic spike protein in your body
Spike protein inhibitors and neutralizers include pine needles, ivermectin, neem, N-acetylcysteine (NAC) and glutathione
The top 10 spike protein detox essentials include vitamin D, vitamin C, nigella seed, quercetin, zinc, curcumin, milk thistle extract, NAC, ivermectin and magnesium
Have you had COVID-19 or received a COVID-19 injection? Then you likely have dangerous spike proteins circulating in your body. While spike protein is naturally found in SARS-CoV-2, no matter the variant, it’s also produced in your body when you receive a COVID-19 shot. In its native form in SARS-CoV-2, the spike protein is responsible for the pathologies of the viral infection.
In its wild form it’s known to open the blood-brain barrier, cause cell damage (cytotoxicity) and, as Dr. Robert Malone, the inventor of the mRNA and DNA vaccine core platform technology,1 said in a commentary on News Voice, “is active in manipulating the biology of the cells that coat the inside of your blood vessels — vascular endothelial cells, in part through its interaction with ACE2, which controls contraction in the blood vessels, blood pressure and other things.”2
It’s also been revealed that the spike protein on its own is enough to cause inflammation and damage to the vascular system, even independent of a virus.3
Now, the World Council for Health (WCH), a worldwide coalition of health-focused organizations and civil society groups that seek to broaden public health knowledge, has released a spike protein detox guide,4 which provides straightforward steps you can take to potentially lessen the effects of toxic spike protein. You can view their full guide of natural remedies,5 including dosages, at the end of this article.
Why Should You Consider a Spike Protein Detox?
Spike proteins can circulate in your body after infection or injection, causing damage to cells, tissues and organs. “Spike protein is a deadly protein,” Dr. Peter McCullough, an internist, cardiologist and trained epidemiologist, says in a video.6 It may cause inflammation and clotting in any tissue in which it accumulates.7
For instance, Pfizer’s biodistribution study, which was used to determine where the injected substances end up in the body, showed the COVID spike protein from the shots accumulated in “quite high concentrations” in the ovaries.8
Further, a Japanese biodistribution study for Pfizer’s jab found that vaccine particles move from the injection site to the blood, after which circulating spike proteins are free to travel throughout the body, including to the ovaries, liver, neurological tissues and other organs.9 WCH noted:10
“The virus spike protein has been linked to adverse effects, such as: blood clots, brain fog, organizing pneumonia, and myocarditis. It is probably responsible for many of the Covid-19 [injection] side effects … Even if you have not had any symptoms, tested positive for Covid-19, or experienced adverse side effects after a jab, there may still be lingering spike proteins inside your body.
In order to clear these after the jab or an infection, doctors and holistic practitioners are suggesting a few simple actions. It is thought that cleansing the body of spike protein … as soon as possible after an infection or jab may protect against damage from remaining or circulating spike proteins.”
Spike Protein Inhibitors and Neutralizers
A group of international doctors and holistic practitioners who have experience helping people recover from COVID-19 and post-injection illness compiled natural options for helping to reduce your body’s spike protein load. The following are spike protein inhibitors, which means they inhibit the binding of the spike protein to human cells:
Prunella vulgaris
Pine needles
Emodin
Neem
Dandelion leaf extract
Ivermectin
Ivermectin, for example, docks to the SARS-CoV-2 spike receptor-bending domain attached to ACE2, which may interfere with its ability to attach to the human cell membrane.11 They also compiled a list of spike protein neutralizers, which render it unable to cause further damage to cells. This includes:
N-acetylcysteine (NAC)
Glutathione
Fennel tea
Star anise tea
Pine needle tea
St. John’s wort
Comfrey leaf
Vitamin C
The plant compounds in the table above contain shikimic acid, which may counteract blood clot formation and reduce some of the spike protein’s toxic effects. Nattokinase, a form of fermented soy, may also help to reduce the occurrence of blood clots.12
How to Protect Your ACE2 Receptors and Detox IL-6
Spike protein attaches to your cells’ ACE2 receptors, impairing the receptors’ normal functioning. This blockage may alter tissue functioning and could be responsible for triggering autoimmune disease or causing abnormal bleeding or clotting, including vaccine-induced thrombotic thrombocytopenia.
Ivermectin, hydroxychloroquine (with zinc), quercetin (with zinc) and fisetin (a flavonoid) are examples of substances that may naturally protect your ACE2 receptors.13 Ivermectin works in this regard by binding to ACE2 receptors, preventing the spike protein from doing so.14
Interleukin 6 (IL-6) is a proinflammatory cytokine that is expressed post-injection and levels increase in those with COVID-19. It’s for this reason that the World Health Organization recommends IL-6 inhibitors for people who are severely ill with COVID-19.15 Many natural IL-6 inhibitors, or anti-inflammatories, exist and may be useful for those seeking to detox from COVID-19 or COVID-19 injections:16
Boswellia serrata (frankincense)
Dandelion leaf extract
Black cumin (Nigella sativa)
Curcumin
Krill oil and other fatty acids
Cinnamon
Fisetin
Apigenin
Quercetin
Resveratrol
Luteolin
Vitamin D3 (with vitamin K)
Zinc
Magnesium
Jasmine tea
Spices
Bay leaves
Black pepper
Nutmeg
Sage
How to Detox From Furin and Serine Protease
To gain entry into your cells, SARS-CoV-2 must first bind to an ACE2 or CD147 receptor on the cell. Next, the spike protein subunit must be proteolytically cleaved (cut). Without this protein cleavage, the virus would simply attach to the receptor and not get any further.
“The furin site is why the virus is so transmissible, and why it invades the heart, the brain and the blood vessels,” Dr. Steven Quay, a physician and scientist, explained at a GOP House Oversight and Reform Subcommittee on Select Coronavirus Crisis hearing.17
The existence of a novel furin cleavage site on SARS-CoV-2, while other coronaviruses do not contain a single example of a furin cleavage site, is a significant reason why many believe SARS-CoV-2 was created through gain-of-function (GOF) research in a laboratory. Natural furin inhibitors, which prevent cleavage of the spike protein, can help you detox from furin and include:18
Rutin
Limonene
Baicalein
Hesperidin
Serine protease is another enzyme that’s “responsible for the proteolytic cleavage of the SARS-CoV-2 spike protein, enabling host cell fusion of the virus.”19 Inhibiting serine protease may therefore prevent spike protein activation and viral entry into cells. WCH compiled several natural serine protease inhibitors, which include:20
Green tea
Potato tubers
Blue green algae
Soybeans
N-acetyl cysteine (NAC)
Boswellia
Time-Restricted Eating and Healthy Diet for All
In addition to the targeted substances mentioned above, WCH was wise to note that a healthy diet is the first step to a healthy immune system. Reducing your consumption of processed foods and other proinflammatory foods, including vegetable (seed) oils, is essential for an optimal immune response.
Time-restricted eating, which means condensing your meals into a six- to eight-hour window, is also beneficial. This will improve your health in a variety of ways, primarily by improving your mitochondrial health and metabolic flexibility. It can also increase autophagy,21 which helps your body clear out damaged cells. As noted by WCH:22
“This method … is used to induce autophagy, which is essentially a recycling process that takes place in human cells, where cells degrade and recycle components. Autophagy is used by the body to eliminate damaged cell proteins and can destroy harmful viruses and bacteria post-infection.”
Another strategy to boost your health and longevity, and possibly to help detox spike protein,23 is regular sauna usage. As your body is subjected to reasonable amounts of heat stress, it gradually becomes acclimated to the heat, prompting a number of beneficial changes to occur in your body.
These adaptations include increased plasma volume and blood flow to your heart and muscles (which increase athletic endurance) along with increased muscle mass due to greater levels of heat-shock proteins and growth hormone.24 It’s a powerful detoxification method due to the sweating it promotes.
Top 10 Spike Protein Detox Essentials — and the Full Guide
Below you can find WCH’s full guide of useful substances to detox from toxic spike proteins, including recommended doses, which you can confirm with your holistic health care practitioner. If you’re not sure where to start, the following 10 compounds are the “essentials” when it comes to spike protein detox. This is a good place to begin as you work out a more comprehensive health strategy:25
Vitamin D
Vitamin C
NAC
Ivermectin
Nigella seed
Quercetin
Zinc
Magnesium
Curcumin
Milk thistle extract
World Council for Health’s Spike Protein Detox Guide26
Substance
Natural Source(s)
Where to Get
Recommended Dose
Ivermectin
Soil bacteria (avermectin)
On prescription
0.4 mg/kg weekly for 4 weeks, then monthly
*Check package instructions to determine if there are contraindications prior to use
Hydroxychloroquine
On prescription
200 mg weekly for 4 weeks
*Check package instructions to determine if there are contraindications prior to use
Vitamin C
Citrus fruits (e.g. oranges) and vegetables (broccoli, cauliflower, brussels sprouts)
Supplement: health food stores, pharmacies, dietary supplement stores, online
6-12 g daily (divided evenly between sodium ascorbate (several grams), liposomal vitamin C (3-6 g) & ascorbyl palmitate (1–3 g)
Prunella Vulgaris (commonly known as self-heal)
Self-heal plant
Supplement: health food stores, pharmacies, dietary supplement stores, online
7 ounces (207 ml) daily
Pine Needles
Pine tree
Supplement: health food stores, pharmacies, dietary supplement stores, online
Consume tea 3 x daily (consume oil/resin that accumulates in the tea also)
Neem
Neem tree
Supplement: health food stores, pharmacies, dietary supplement stores, online
As per your practitioner’s or preparation instructions
As vaccine mandates and passports gain ground across the U.S., so too are alleged cases of vaccine card fraud. As reported by WGN Chicago, some prosecutors are now treating fake vaccine cards as a federal crime.
But should they be doing that — and is it even legal to do so? Federal investigators say yes, if it involves use of official U.S. seals and lying to federal investigators.
Already, the feds are charging producers of the fraudulent cards with federal offenses that come with up to 15 years in prison for each count, plus additional time for lying.
En Garde! After coming out with a tell-all book on the real Dr. Anthony Fauci and his follies through the years, Robert F. Kennedy Jr. stands ready to engage anyone and everyone, including Fauci himself as well as Fauci’s media friends, to a one-on-one debate on the truth about Fauci.
Kennedy’s book, “The Real Anthony Fauci: Bill Gates, Big Pharma, and the Global War on Democracy and Public Health,” is a best seller, fully sourced and referenced. It documents Fauci’s follies through the decades and lunges at the connections between him, Gates and the industry.
The picture it paints isn’t pretty, and Fauci and friends like CNN’s Jake Tapper are teaming up and parrying Kennedy’s assertions in an attempt to discredit the book’s contents — but only from a safe point in line.
Although Kennedy has challenged them all to a debate on live TV, they will never actually agree to engage in one, in person, with Kennedy, Steve Kirsch says, because they know they will lose.
This is a Swiss Gold Mine with link after link after link to the studies and sources. And then yet more studies and sources…. As in FULLY referenced and FULLY sourced. How in almost every country of the world the death rate is comparable to a flu season for the general working age population — once you subtract out nursing home deaths. If you will only ever read one more article on COVID-19, this is the one.
Ivermectin is a wonder drug that’s been approved for human use since 1987, and the World Health Organization has had it on its list of essential medicines for years.
With billions of doses administered around the world, its safety profile is proven, and the two men who discovered it were awarded a Nobel prize in 2015. Why, then, is this natural product, which has also been proven safe for animals, so vilified when it’s mentioned for use in combating COVID-19?
For more information, watch this short video about the many other diseases that this antiparasitic, antiviral, anti-inflammatory, antibacterial and anticancer drug has shown promise for.
SOURCE: Odysee December 20, 2021
Resorting to name-calling in the wake of Robert F. Kennedy Jr.’s book, “The Real Anthony Fauci: Bill Gates, Big Pharma, and the War on Democracy and Public Health,” Fauci told Yahoo! News that Kennedy is “a deeply disturbed individual.”
Kennedy has invited anyone who wants to dispute what he’s written to a debate, but so far no one, including Fauci, has taken up the offer. Instead, Fauci is busy name-calling and down-playing the book by saying Kennedy’s truths and accusations are going to hurt people.
Fauci’s words are rolling off Kennedy’s back, however. In response to Yahoo!, he said, ““Dr. Fauci’s belief that, as a government official, he should be immune from criticism is contrary to our nation’s democratic traditions.”
A cache of high-power figures in the COVID-19 pandemic and the so-called “vaccines” to combat the infection have been charged with several crimes against humanity, including war crimes.
Bill and Melinda Gates, Dr. Anthony Fauci, Peter Daszak and a dozen others were charged in the International Criminal Court December 6, 2021 with numerous violations of the Nuremberg Code, The Desert Review reports.
Also charged were the World Health Organization’s director-general, the U.K.’s prime minister and the World Economic Forum’s president Klaus Schwab. The actual filing is 46 pages long, and it describes the alleged crimes in detail.
(Natural News) Two new studies from South Africa found that the country has a lower hospitalization rate for Wuhan coronavirus (COVID-19) infections caused by the post-vaccine omicron variant. High levels of natural immunity among South Africans stemming from prior COVID-19 infections is likely a contributing factor to this.
Since the appearance of the post-vaccine omicron variant, mainstream media outlets have tried to speculate regarding the variant’s virulence and deadliness. They repeatedly ignored South African health authorities, including Health Minister Joe Phaahla, who said that hospitalizations caused by omicron are “relatively low” and that the world has nothing to worry about.
According to data from South African health authorities, COVID-19 cases in South Africa have skyrocketed in recent weeks, in line with the emergence of the post-vaccine omicron variant. But what has puzzled scientists studying the data is that the country’s hospitalization rate has risen at a significantly slower pace compared to previous waves. (Related: In the age of Omicron, the jabbed are now catching & spreading COVID at a higher rate than the unvaxxed.)
The data strongly suggests that people diagnosed with omicron in South Africa were around 80 percent less likely to be admitted to the hospital than those diagnosed with any other COVID-19 variant.
Once admitted to the hospital, patients infected with omicron have a lower chance of developing severe disease. They are also hospitalized for fewer days on average than other COVID-19 patients.
In the first 31 days of the current post-vaccine outbreak, the country recorded 164,911 new COVID-19 cases. But just 3,432 patients were admitted to hospitals for additional care. One-hundred and ninety-four died.
In comparison, during the first 31 days of the previous wave, 38,577 COVID-19 cases were recorded and 10,088 were admitted to hospitals. The death rate of that wave was also more than three times higher than the death rate of the current wave, with 668 deaths in the first 31 days.
High vaccination rates unlikely to protect countries against omicron
“We believe that the evolution of cell-mediated immunity from prior natural infection … is resulting in the uncoupling of the high case rates seen with the omicron variant and the rates of severe disease,” wrote South African researchers in one of the new studies conducted on the outbreak in the country.
They added that the immunity “is primarily due to natural infection.”
While the authors included several caveats in their assessment regarding South Africa’s outbreak, they wrote that it is “difficult to disentangle the relative contribution of high levels of previous population immunity versus intrinsic lower virulence to the observed lower disease severity.”
“Compellingly, together our data really suggest a positive story of a reduced severity of omicron compared to other variants,” said Cheryl Cohen, an epidemiology professor for the University of the Witwatersrand and a member of the National Institute for Communicable Diseases in South Africa and an author for one of the studies.
Cohen believes the data is generalizable to other countries in Sub-Saharan Africa which have similar levels of previous infection and vaccination.
“I think what is unclear is how the picture will be similar in countries where there are high levels of vaccination but very low levels of previous infection,” she said. “The baseline epidemiology is different. But I think, compellingly, our data really suggests a positive story of a reduced severity of omicron compared to other variants.”
Listen to this Situation Update episode of the Health Ranger Report, a podcast by Mike Adams, the Health Ranger, as he speculates about how the post-vaccine omicron variant could be the cure to COVID-19.
For the latest news on the omicron variant, visit Pandemic.news.
The paper they all co-authored together concluded that the Moronic variant is “markedly resistant” to both the primary jabs and the “boosters.” It does not matter how many shots people get; whatever is inside all those syringes will not keep anyone safe against the latest strain of the Fauci Flu.
“A striking feature of this variant is the large number of spike mutations that pose a threat to the efficacy of current COVID-19 vaccines and antibody therapies,” the study explains.
The Moronic variant’s “extensive” mutations have the potential to “greatly compromise” the vaccine, the study adds. In essence, the jabs become worthless following exposure to them (assuming the shots provided any benefits to begin with).
“Even a third booster shot may not adequately protect against Omicron infection,” the paper reads, noting that Moronic “may still pose a risk” to people who have been triple-jabbed.
These findings align with currently emerging clinical data showing that Moronic demonstrates higher rates of both reinfection and vaccine breakthroughs, the authors further found.
One such study says that Moronic is around 70 times more transmissible than “Delta,” though much less severe.
Mother Nature’s micronutrient secret: Organic Broccoli Sprout Capsules now available, delivering 280mg of high-density nutrition, including the extraordinary “sulforaphane” and “glucosinolate” nutrients found only in cruciferous healing foods. Every lot laboratory tested. See availability here.
“It is not too far-fetched to think that this [COVID-19] is now only a mutation or two away from being pan-resistant to current antibodies,” the study added further.
“We must devise strategies that anticipate the evolutional direction of the virus and develop agents that target better conserved viral elements.”
Covid jabs are ineffective against the Delta variant, too
The latest official data claims that 5.3 million people worldwide have died after testing “positive” for the Wuhan Flu. Of this, more than 802,000 deaths occurred in the United States.
Where this data goes wrong, however, is in the fact that almost all deaths for the past 20 some-odd months have been blamed on “covid,” even when they involved things like motorcycle accidents, drownings or other unrelated incidents.
The way the government tabulates “unvaccinated” covid deaths is also deceptive. A fully vaccinated person who dies within the first two weeks post-injection is counted as a “covid” death, it turns out, which greatly inflates the count.
Research published in the Lancet Infectious Diseases journal found that getting vaccinated has little effect on the “Delta” variant as well, along with all other forms of covid.
Not only can a fully vaccinated person still spread the Delta variant, but he or she can also become infected with it. In fact, most new cases of covid, regardless of the variant, seem to be occurring in people who took the jabs.
You might say, based on all of this, that getting jabbed for covid is an exercise in futility. There is no protection to be had from doing it, so why bother and risk other potential complications?
One Natural News commenter speculated that the true reasons for the jab push include generating lots of new cash for Big Pharma; killing people off from organ failure; genetically reengineering the human body; and injecting surveillance and control technology into people.
“Mass hysteria is ruining the USA, thanks to the mainstream media,” wrote another. “MILLIONS of people are still clueless about the conflict-of-interest nature of the mainstream media.”
“The ‘pandemic’ was / is a lie. The ‘safe and effective’ claim about ‘vaccines’ is a lie. And the mainstream media stirs up mass hysteria among the masses.”
The latest news about the Chinese Virus and its many variants can be found at Pandemic.news.
(Natural News) According to an announcement linked below, the US military is rolling out a Spike Ferritin Nanoparticle COVID vaccine (SpFN) that they claim protects users against all strains of coronavirus. If the claim is true, the vaccine might work almost as good as a person’s own immune system, which means that the US military has managed to create a “vaccine” that works almost as good as doing nothing at all.
Scientists in WRAIR’s Emerging Infectious Diseases Branch (EIDB) developed the SpFN nanoparticle vaccine, based on a ferritin platform, as part of a forward-thinking “pan-SARS” strategy that aims to address the current pandemic and acts as a first line of defense against variants of concern and similar viruses that could emerge in the future.
In this context, “pan” means it works on everything. This is supposed to be a “universal” vaccine that treats all variants, now and in the future.
If true, this would make Pfizer and Moderna vaccines obsolete. Not that either one of those is actually a legitimate “vaccine” in the first place, of course. It has been clear from the very start that the purpose of Pfizer and Moderna vaccines was never to build immunity but rather to destroy immunity by hijacking the body and forcing it to manufacture spike protein nanoparticles — which are bioweapons.
From the announcement:
Pre-clinical studies published today in Science Translational Medicine indicate that the SpFN vaccine protects non-human primates from disease caused by the original strain of SARS-CoV-2 and induces highly-potent and broadly-neutralizing antibody responses against major SARS-CoV-2 variants…
Get more news like this without being censored: Get the Natural News app for your mobile devices. Enjoy uncensored news, lab test results, videos, podcasts and more. Bypass all the unfair censorship by Google, Facebook, YouTube and Twitter. Get your daily news and videos directly from the source! Download here.
This is good news. If it works on non-human primates, they can administer it to Nancy Pelosi and whatever creatures are currently running the Pentagon itself.
On a serious note, however, the human body already has amazing nanotechnology that fights EVERY pathogen… it’s called the immune system. And it works better than anything the military can possibly come up with. How do you activate the immune system to function better? Vitamin D.
The neat thing about vitamin D is that it’s dirt cheap, widely available and has a huge margin of safety for everyday use. It also helps the body regulate normal cell division, blood sugar, neurological function, kidney function and much more. Vitamin D is the single most affordable and effective nutritional intervention currently known to humankind, yet nobody in the Pentagon or the government — not Biden and not even Trump — will dare advocate for vitamin D because it isn’t owned by Big Pharma.
Vitamin D can’t turn pharma CEO creeps into overnight billionaires, in other words, so it gets almost zero mention in the corporate-controlled media. We cover vitamin D, of course, with hundreds of news stories. Check out VitaminD.news
They aren’t trying to save soldiers; they’re trying to exterminate them
Given that the Pentagon is now run by treasonous Marxists and communists who hate America, we can only conclude that this new SpFN synthetic biology vaccine technology is a more advanced kill switch to achieve the mass murder of active duty soldiers.
It will probably kill them slowly, over a few years, in order to avoid the mass deaths showing up in the short-term human trials the Army claims to be running. As we have already covered extensively, the spike protein nanoparticles from mRNA vaccines enter cell nuclei and suppress the NHEJ mechanism that repairs double strand breaks (DSBs) in chromosomes, caused by ionizing radiation. NHEJ stands for Non-Homologous End Joining and it is the primary DNA repair mechanism that maintains genetic integrity across all carbon-based lifeforms (including plants). Without NHEJ functioning, a person loses genetic integrity, resulting in mutations, cancer, inability to repair tissue, inability to generate red blood cells, infertility and so on.
There’s no doubt that the Army team working on this synthetic spike protein isn’t testing its ability to suppress NHEJ. Why do they care when there’s zero liability for the military when hundreds of thousands of soldiers die from cancer over the next decade?
It’s all part of decimating the military in preparation for an invasion by China
Sadly, under the control of lunatic left-wing generals, the US military has shifted from defending America to destroying it. This is all driven by communist China, of course, which has ordered treasonous generals to mass murder US soldiers, clearing the way for a Chinese PLA invasion of the continental United States.
The “vaccines” are simply the weapon system to exterminate enough active duty soldiers so that America’s defenses will be largely nullified. Once that is accomplished, the invasion begins. This is how China coerced America into killing off its own active duty military soldiers before the invasion. Classic Sun Tzu, Art of War: The war is won or lost before it even begins, by reshaping the battlefield.
This isn’t a conspiracy theory; it’s the publicly stated military posture of China and its top generals who have repeatedly called for invading and occupying America in order to acquire the farmland needed to keep China’s population alive. (China cannot produce enough food domestically and must currently import food from all over the world.)
Watch my extensive interviews with JR Nyquist if you’re interested in learning the truth about China’s plans to conquer America. Here are a few:
Operation Warp Speed is actually an operation to exterminate Americans
Don’t forget that President Trump launched Operation Warp Speed and bragged about using the US military to distribute and administer vaccines. That plan is still in place, and it almost certainly means the military will be invoked to go door-to-door, forcibly injecting people with death shots at gunpoint.
If you don’t think that day is coming, you are an oblivious idiot. Every single thing you’re seeing happen right now is something I publicly predicted years in advance: The medical kidnapping, forced quarantine centers, vaccine passports, mask mandates, medical censorship and all of it.
People like myself, Alex Jones and a few others have a near-perfect track record of calling all this in advance. What was considered a “conspiracy theory” five years ago is now a public reality.
All they need now is the release of a far more aggressive bioweapon followed by mass media hysteria and a call to silence or imprison all “anti-vaxxers.” In 2022, look for a new state of emergency to be declared, followed by an attempt at nationwide gun confiscation and gunpoint vaccine enforcement anywhere they can get away with it.
They likely won’t be able to pull it off in rural areas and in red states like Texas and Florida, but they’ll try it in New York, California, Colorado, New Jersey and other blue states. Anyone who goes along with it will likely be dead within a decade. The covid death camps will be ramped up across blue states, and exterminations will be under way well before the end of 2022.
It’s a depopulation program, after all. Those who volunteer to be depopulated shall get their wish via the spike protein nanoparticle injections.
First rule of survival: Don’t inject yourself with biological weapons…
Learn more in today’s uncensored Situation Update podcast:
In a small study of party-goers who fell ill with COVID-19 after the party, 98% were vaccinated, Science Norway reports.
The party-goers attended an event that lasted several hours and involved riding a bus from the venue to a restaurant. While it was a private party, attendees were in several public venues and events before and after dinner.
An investigation into the outbreak revealed that 98% were fully vaccinated 79 days before the party. All had a negative PCR test within two days of the party.
In the mid-1960s, the autism rate was 1 in 10,000. By 2012, it had shot up to 1 in 88. In 2016, it was 1 in 68, and now it’s 1 in 44 8-year-olds
Rates vary widely from state to state. In California, where incidence is the highest, 1 in 26 8-year-olds has a diagnosis of autism. Missouri, which has the lowest incidence, has a rate of 1 in 60
Improved diagnosis alone cannot explain this trend. Genetics play only a minor role, and even then, primarily only when combined with toxic exposures
Glyphosate appears to be a leading contributor to autism
Other contributing factors include maternal antibodies associated with autoimmune diseases, maternal immune system overactivation and mitochondrial dysfunction (typically involving electron transport chain overactivity). Mitochondrial abnormalities are suspected of being involved in as many as 80% of cases
In the mid-1960s, the autism rate was 1 in 10,000.1 By 2012, it had risen to 1 in 88,2 then 1 in 68 as of 2016,3 and now, we’re looking at an autism rate of 1 in 44 8-year-olds, although rates vary widely from state to state.4
In California, where incidence is the highest, 1 in 26 8-year-olds has a diagnosis of autism. Missouri, which has the lowest incidence, has a rate of 1 in 60. According to the U.S. Centers for Disease Control and Prevention, the dramatic uptick is in part due to improved and more comprehensive identification and diagnosis.
However, improved diagnosis alone cannot explain this trend. One in 44 children were not autistic in the 1980s, with or without diagnosis. No, something is going on. One or more environmental factors are clearly having a devastating impact on our children.
Mitochondrial Dysfunction in Autism
According to an October 2020 scientific review5 in the journal Seminars in Pediatric Neurology, “Several lines of evidence implicate mitochondria in the pathophysiology of autism spectrum disorder (ASD).” For years, autism was believed to be due to genetics, but empirical studies have proven genetic predispositions play a very small role.
The authors point to “novel abnormalities” in mitochondrial function that have been found in autistic children, and the fact that treatments targeting mitochondrial dysfunction, such as L-carnitine supplementation and a ketogenic diet, have been fruitful.
In 2007, approximately 4% of autistic children could be diagnosed with a definite mitochondrial disease. More recent investigations looking at mitochondrial biomarkers and electron transport chain activity suggest mitochondrial abnormalities may be involved in as many as 80% of cases. Biomarkers of mitochondrial dysfunction include elevated levels of:
Lactate
Pyruvate
Alanine
Creatine kinase
Ubiquinone
Acyl-carnitines
Carnitine (low levels being an indication of dysfunction)
As noted by the authors, this is “remarkably interesting” because mitochondria are “very vulnerable to environmental factors.” In other words, something in our environment is triggering mitochondrial dysfunction in an ever-growing percentage of children. The question is what?
Children whose autism is rooted in mitochondrial dysfunction will typically have a key set of symptoms that include:
Fatigability
Gastrointestinal disorders
Seizures and/or epilepsy
Motor delay and/or ataxia and/or muscle weakness
Unusual neurodevelopmental regression, including multiple regressions or regression later than commonly associated with ASD
Mitochondrial Overactivity
While classic mitochondrial disease is defined, at least in part, by severe deficits in electron transport chain activity, in children with ASD, mitochondrial dysfunction tends to involve overactivity. According to the authors:6
“… we have shown that about one-third of LCLs [lymphoblastoid cell lines] derived from children with ASD repeatedly show elevated respiratoryiou rates, approximately 200% of controls, for respiratory parameters associated with adenosine triphosphate production.
We have also demonstrated the consequences of elevated respiratory rates; specifically, this subset of ASD LCLs are more sensitive to acute exposure to reactive oxygen species (ROS) such that respiratory rates drop precipitously with acute increases in ROS.
We hypothesized these changes represent an adaptive response to previous environmental exposures, a phenomenon known as mitoplasticity.
To support this hypothesis, we demonstrated that elevated respiratory rates can be induced in LCLs with prolonged exposure (96 hours) to mild ROS, a microenvironment that simulates the effect of environmental toxicants on mitochondria.
Additionally, we have demonstrated that this subset of LCLs respond differently to environmental agents associated with ASD, including trichloroacetaldehyde hydrate and ethylmercury, and enteric short chain fatty acids propionate and butyrate, as compared to ASD LCLs which do not demonstrate these high respiratory rates at baseline.”
Important Nutritional Supplements
Two helpful treatments have already been mentioned: L-carnitine supplementation and ketogenic diets. Studies evaluating ketogenic diets and ASD have found them to be well-tolerated by a majority of children.
A review of four studies found 18% of children saw significant improvement on a ketogenic diet, 40% reported moderate improvement and 32% had mild improvement. Only 8% experienced a worsening of their symptoms.7
In cases where the ASD is caused by mitochondrial dysfunction, however, supplementing specific cofactors become important. The good news is this kind of supplementation is very safe and well tolerated. There’s virtually no risk involved, in terms of adverse side effects. Among the most important nutritional cofactors are:8
Of these, L-carnitine has been most widely studied. As explained in this paper:9
“Two medium sized (n = 30, 30) double-blind placebo-controlled studies using L-carnitine treatment (50 mg/kg/d for 3 months and 100 mg/kg/d for 6 months) found that scores on the Childhood Autism Rating Scale (CARS) improved with L-carnitine as compared to placebo with one study finding that greater symptomatic improvement was correlated with a greater increase in blood carnitine levels.
A small (n = 10) 8-week open-label trial of L-carnitine used particularly high doses (up to 400 mg/kg/d in 3 divided doses, maximum of 6000 mg/d) …
Several parental rated measures showed improvements in behavior and hyperactivity before correction for multiple comparisons and improvements in language correlated with post-treatment blood carnitine levels. Children with ASD and genetic mutations in the carnitine pathway also appear to response to L-carnitine.”
CoQ10 has also been evaluated in clinical trials. In one, 50 mg of ubiquinol was given twice a day for three months. Children who attained a CoQ10 blood level above 2.5 umol/L saw improvements in communication, interactions, sleep and food rejection.10
A three-month-long regimen of L-carnitine, CoQ10 and alpha-lipoic acid also produced encouraging results, improving mitochondrial function and ASD-related behavior. When the children discontinued the cocktail, their behavior worsened again.
Autism and Autoimmunity
Previous research also suggests ASD may have an autoimmunity component. As explained in a 2009 paper titled “Autoimmunity in Autism”:11
“Increasing evidence of autoimmune phenomena in individuals with autism could represent the presence of altered or inappropriate immune responses in this disorder, and this immune system dysfunction may represent novel targets for treatment.
Furthermore, in recent studies, antibodies directed against the fetal brain have been detected in some mothers of children with autism; these antibodies have the ability to alter behavioral outcomes in the offspring of animal models.”
Research12,13 published in 2013 found that more than 1 in 10 mothers of autistic children had antibodies associated with autoimmunity that adversely reacted with proteins in the brain of the baby, resulting in ASD. The authors point out that any activation of the mother’s immune system “might lead to an increased risk of a child with ASD.”
In light of the COVID injection campaign, the possibility of autoantibodies playing a role in ASD is extremely troublesome, as autoimmune diseases are a potential side effect. We don’t yet really know the extent of which the SARS-CoV-2 spike protein interacts with the human brain, but it’s clearly not beneficial.
Women, in particular, are suffering neurological dysfunction as a result of the COVID shot. How might the spike protein affect offspring? That’s still too early to say, but I suspect we’ll come to find that the effect can be devastating.
Toxic Chemicals Implicated in Autism
Not surprisingly, exposure to toxic chemicals in utero has also been identified as a potentially causative factor. According to the National Academy of Sciences, an estimated 3% of all neurobehavioral disorders in children are caused by toxic exposures.
Another 25%, the interaction of toxic exposures and genetic factors is thought to be causative.14,15 In 2012, scientists identified 10 chemicals suspected of causing learning disabilities and ASD:16
Lead
Methylmercury
Polychlorinated biphenyls (PCBs)
Organophosphate pesticides, including glyphosate
Organochlorine pesticides
Endocrine-disrupting chemicals
Automotive exhaust
Polycyclic aromatic hydrocarbons (PAHs)
Brominated flame retardants
Perfluorinated compounds
Of these, glyphosate is a top suspect17,18 for the simple reason that exposure to it is so widespread. Research19 published in 2019 found women exposed to 11 commonly used pesticides — including glyphosate — during pregnancy have a higher risk of having a child diagnosed with autism.
Pregnant women who lived within a 2,000-meter (1.24 miles) radius of a highly-sprayed area were 10% to 16% more likely to have children diagnosed with autism than those who lived farther away. As reported by Time:20
“When they looked at diagnoses of autism spectrum disorder that also came with intellectual disabilities, they found on average 30% higher rates among children who were exposed to the pesticides while in utero. Exposure in the first year of life increased the risk of autism by up to 50% compared to those not exposed to certain pesticides.”
Glyphosate Is Likely a Key Culprit
Stephanie Seneff, Ph.D., who has spent a large portion of her career studying glyphosate, believes it is a significant cause or contributor to autism. She’s shown glyphosate:
Disrupts your gut microbiome
Impairs peristalsis — a feature that is exceedingly common in children with autism21
Inhibits bile acid release by impairing gallbladder contraction — Many autistic children have very pale stool, suggestive of low bile acid levels
Impairs digestive enzymes — Many autistic children also have undigested particles in their stool, which suggests a lack of digestive enzymes. And, indeed, glyphosate affects your digestive enzymes, particularly trypsin, pepsin and lipase
The Roles of GI Inflammation and Maternal Gut Bacteria
Another potential trigger is maternal gut inflammation. Research22 published in early December 2021 found that when pregnant mice were challenged with immune activation, it changed their gut microbiota. This altered microbiota in turn primed the offspring for intestinal inflammation that resulted in neurodevelopmental disorders. MIT News reported the findings, noting:23
“Infection during pregnancy with elevated levels of the cytokine IL-17a may yield microbiome alterations that prime offspring for aberrant immune responses …
When a mother experiences an infection during pregnancy and her immune system produces elevated levels of the molecule Interleukin-17a (IL-17a), this can not only alter brain development in her fetus, but also alter her microbiome such that after birth the newborn’s immune system can become primed for future inflammatory attacks.
In four studies beginning in 2016,24 study co-senior authors Gloria Choi of MIT and Jun Huhof Harvard University traced how elevated IL-17a during pregnancy acts on neural receptors in a specific region of the fetal brain to alter circuit development, leading to autism-like behavioral symptoms in mouse models.
Their new research … shows how IL-17a can act to also alter the trajectory of immune system development. ‘We’ve shown that IL-17a acting on the fetal brain can induce autism-like behavioral phenotypes such as social deficits,’ says Choi …
‘Now we are showing that the same IL-17a in mothers, through changes in the microbiome community, produces co-morbid symptoms such as a primed immune system.’
The researchers caution that the study findings are yet to be confirmed in humans, but that they do offer a hint that central nervous and immune system problems in individuals with autism-spectrum disorders share an environmental driver: maternal infection during pregnancy.”
Here, the COVID-19 pandemic may end up worsening an already terrible trend, as the infection is associated with elevated IL-17a. IL-17a is a key molecule in both the innate and adaptive immunity that helps mobilize your immune system response during early infection. It’s been singled out as being involved in the thrombotic and vascular mechanisms of COVID-19 specifically.25
One October 2021 study26 suggested IL-17a acts as a silent amplifier of the COVID-19 immune response, resulting in some of the worst side effects associated with the infection. While pregnant women are universally instructed to get the COVID shot to protect themselves from the infection, there’s every reason to suspect the injection may cause far more harm than the infection itself.
If you get COVID while pregnant, you may or may not have a serious case of it, but if you take the shot, you have a 100% chance of suffering the effects of it, which for many include dramatically elevated levels of inflammation.
From my perspective, getting the COVID jab because you fear what COVID-19 might do to you and/or your baby is actually irrational, as your risk of adverse effects from the shot is exponentially higher than your risk of severe COVID-19 infection.
Autism Is a Multifactorial Condition
A number of other culprits could also be named, such as retroviruses (which the COVID shots can reactivate) and electromagnetic field (EMF) exposure. According to Judy Mikovits, Ph.D., a retrovirus family known as xenotropic murine leukemia virus-related viruses (XMRV) may play a causal role in autism.27
Disturbingly, one source for XMRVs is contaminated childhood vaccines. Mikovits details the history of this in her book, “Plague: One Scientist’s Intrepid Search for the Truth About Human Retroviruses and Chronic Fatigue Syndrome (ME/CFS), Autism and Other Disease.”
In previous interviews with me, Mikovits has also expressed concern that the COVID shots may activate latent XMRV infection. If it does, we could expect the autism rate to explode at an even more exponential rate than we’re seeing already.
I predict the COVID shots will be found to contribute to autism in a number of different ways. But even in the absence of these injections, it’s clear that environmental toxicities are wreaking havoc with our children’s health.
There’s no single answer to this problem. Since many different toxins can contribute, preventing autism must include the elimination of most toxic exposures.
Top suspects include childhood vaccines, the 10 chemicals listed earlier (glyphosate in particular), autoimmune antibodies, gut inflammation, retroviruses and EMF exposure. To this list, I would also add the COVID gene transfer injections, as they can be a source of severe inflammation and autoimmunity, and have been shown to have a direct adverse impact on neurology.
Most Americans do NOT know about the many benefits of NAD “drip” therapy
Wondering why most Americans don’t know about these safe methods to beat Covid? Because they work and they’re inexpensive, that’s why. NAD regenerative therapy is simple and convenient, where the person can sit in a chair and read, surf the internet or watch a movie while the drip is administered through an IV (for about 90 minutes).
On a cellular level, NAD IV therapy delivers oxidized coenzyme directly into the bloodstream, allowing more of the vital coenzyme to be absorbed by the body, circumventing the digestive system that would otherwise break down much of the effectiveness before it gets to the cells.
NAD is known to improve cognition, reduce pain, boost energy, revive neurological function, reduce inflammation and delay the onset of cardiovascular and metabolic diseases. In fact, lowered levels of NAD have been scientifically linked to fatty liver disease and diabetes, but hospitals and most medical doctors in America are not allowed to tell their patients about it or use it for Covid because it works. Only useless means of addressing Covid are allowed in Western Medicine, like gene therapy jabs (that CAUSE vascular and immune problems), Remdesivir (that cripples kidney function), masks that cause bacterial infections and booster shots that will worsen ADE disorder (autoimmune deficiency enhancement disorder).
Dana White is not anti-vaccine so how will the mass media degrade him and say he’s an anti-science freak, when he already got the Covid jabs? Here’s White commenting on the situation:
“Rogan is a very brilliant guy, very smart guy who talks to the best and the brightest out there. And I’m not a believer in the narrative. I’m not a big believer in the narrative. But you know what, at the end of the day, (Jim)? It’s a free country.”
For the most reliable truth news about health and safety on the internet, tune to Pandemic.news to learn how to best cope with Covid government mandates.
A federal bill passed by the U.S. House of Representatives barely got a blink from mainstream media, but it’s one that will have wide-ranging, long-lasting impact on the entire U.S. if it makes it through the Senate and becomes law.
H.R. 550, entitled “Immunization Infrastructure Modernization Act of 2021,” expands the powers of state and local health departments to track citizens’ vaccination status and set the stage for vaccine passports and possibly no-fly lists.
The far-reaching bill literally gives powers to unelected health care directors, who could arbitrarily set dangerous precedents when it comes to vaccine mandates, restrictions of services and other sanctions against unvaccinated individuals — all without fear of losing their jobs in the next election cycle.
It’s time to contact your legislators and let them know by phone or email that they need to stand for freedom of choice and restore democracy to the health care setting.
A leading technology and media expert who has been dubbed “the original COVID-19 whistleblower” has scored an interview with a Canadian military officer who says he was part of the October 2019 World Military Games in Wuhan.
The officer shared how he and others at the games became ill while they were there, and continued to be very ill on the flight home and after they got home, but both military and health officials are denying that COVID-19 might have been the cause of their illness.
In a five-hour podcast, Metzl talks about COVID, the possibility that it was caused by a lab leak and other COVID-related topics.
In a quiet change to its terms of service, Twitter is now arbitrarily censoring tweets that claim people who have had the COVID-19 shots can spread or shed the virus.
The social giant also listed other COVID-related offenses that could garner penalties, including citing medical research that Twitter determines is representative of “a specific narrative that diminishes the significance of the disease.” The penalties range from having “corrective” labels put on the offending tweets to being permanently banned from Twitter.
“The change was made on December 2, 2021, according to Wayback Machine archives retrieved by Reclaim the Net,” Mediaite reports. “The policy contradicts the Centers for Disease Control and Prevention guidance, which notes the ‘risk for SARS-CoV-2 infection in fully vaccinated people cannot be completely eliminated as long as there is continued community transmission of the virus.’”
November 2, 2021, the prestigious British Medical Journal published an article about Pfizer’s COVID-19 clinical trials, written by a commissioned investigative reporter. It included what The BMJ said were “dozens of internal company documents, photos, audio recordings and emails.”
Yet, besides passing The BMJ’s “usual high-level editorial oversight and review,” and even though the work underwent both a legal review and an external peer review, Facebook/Meta CEO Mark Zuckerberg’s “fact” checkers labeled it as “misleading” and “false information.”
Concerned that the so-called “fact” checkers seriously didn’t know what they were doing, The BMJ tried to contact the fact checkers, but they didn’t respond. So, The BMJ editors decided to take on Facebook and the fact checkers with a public letter to Zuckerberg.
“There is also a wider concern that we wish to raise,” the editors wrote. “We are aware that The BMJ is not the only high quality information provider to have been affected by the incompetence of Meta’s fact checking regime. To give one other example, we would highlight the treatment by Instagram (also owned by Meta) of Cochrane, the international provider of high quality systematic reviews of the medical evidence.”
To top it off, The BMJ requested that Facebook get its act together: “Rather than investing a proportion of Meta’s substantial profits to help ensure the accuracy of medical information shared through social media, you have apparently delegated responsibility to people incompetent in carrying out this crucial task.
“We hope you will act swiftly: specifically to correct the error relating to The BMJ’s article and to review the processes that led to the error; and generally to reconsider your investment in and approach to fact checking overall.”
The latest official data coming from the United Kingdom is that pandemic deaths are now happening in double- and triple-“vaccinated” individuals — all since August 2021. Specifically, according to Daily Expose, “the latest official data shows that the vaccinated population have accounted for 3 in every 5 Covid-19 cases, 3 in every 5 Covid-19 hospitalizations, and 4 in every 5 Covid-19 deaths.”
Yet, government officials including Prime Minister Boris Johnson are insistent on restricting the freedoms of those they identify as “unvaccinated.” The reason they give is that the government needs to protect the public from the new Omicron COVID-19 variant.
But since the vaccinated are the majority of who’s getting sick and dying, what is the purpose of the new strict measures? Daily Expose has one answer, saying it “suggests vaccine passports have absolutely nothing to do with protecting public health, and instead everything to do with controlling the nation.”
One team published an engineering analysis to determine the current underreporting factor (URF) from the VAERS information and found the factor to be 41. When applied against the government data they found 173% more children died from the vaccine than from the illness
Using this same URF, the number of deaths from COVID rose to 815,326 and the number permanently disabled to 1,338,404. To date, the total reported deaths from the infection is 803,043, which means the shot has killed more children and adults than the virus
Although there is little reason to give children the shot, officials are spinning the idea that it is needed for herd immunity. Yet, health officials must be aware there is a significant lack of evidence to support this, and children are dying in the process
Pilot deaths and injuries affect commercial flights, logistical distribution of goods and military readiness. In one affidavit as part of a federal lawsuit against the military vaccine mandate, physician Lt. Col. Theresa Long alleges protocols are not followed after the COVID shot
Many scientists and health experts have warned that vaccinating children against COVID-19 is unnecessary and extremely risky. Since the beginning of the pandemic, it has been obvious that children were at exceptionally low risk for hospitalization and death from the infection.1 Despite this, massive efforts are underway to ensure that every child gets a shot.
If the current data from the Vaccine Adverse Events Reporting System (VAERS)2 are any indication of what the future holds, we are facing the greatest public health calamity in modern history. I believe it is not a new COVID-19 variant causing this, but the current vaccination campaign. Unfortunately, I have no doubt that the deaths caused by the vaccines will end up far exceeding the number of deaths from the illness.
Despite the clear and present dangers of this genetic therapy, vaccine makers, encouraged and endorsed by government health agencies, are steamrolling ahead with trials and recommendations for the shot in children. In May 20213 parents found out that their children can get vaccinated without their consent if they fall under something called the “mature minor” doctrine.
This allows providers to treat minors, without parental consent, under certain circumstances. The age group under question was between ages 14 and 18 when there is a “rebuttable presumption of capacity, and the physician may treat without parental consent unless the physician believes that the minor is not sufficiently mature to make his or her own health care decisions.”
In July, two lawsuits were filed in federal court that challenged the Washington D.C. city law which allowed minors to be vaccinated without parental consent.4 In September 2021, The Guardian reported that children aged 12 to 15 in the U.K. may be administered a COVID-19 shot by teams in the school system without parental consent.5
If parents do not consent but the child wants the vaccine, the team can determine if a 12-year-old is able to make an informed decision. Most recently, one California mother spoke to the news media and expressed outrage after the school system allegedly offered her son a pizza in exchange for his taking the genetic therapy shot.6
With each passing month, it becomes more obvious that the battleground in the fight for liberty and freedom has been taken to our young children. A recent review of data7 from the CDC and the Vaccine Adverse Event Reporting System (VAERS) shows that more children have died from the vaccine than have died from the illness.
VAERS Underreporting Factor Affects Data
To compare the number of deaths from COVID illness against those who have died from the genetic therapy injection, we must address the known underreporting factor in VAERS. To date, the VAERS database is the only reporting system used by the CDC and FDA that is accessible to the public. According to VAERS, it:8
“… is a passive reporting system, meaning it relies on individuals to send in reports of their experiences. Anyone can submit a report to VAERS, including parents and patients.”
Additionally, it is the only area where the public, including doctors and other medical professionals, can voluntarily report vaccine adverse events, including death. According to VAERS,9 health care professionals are mandated by law to report serious injury adverse events that occur within a specified time period after the shot, and those events that are listed by the manufacturer as a contraindication to further doses.
However, the system only “encourages” providers to report events after vaccination whether the shot caused the event or not. In other words, the system depends on the health care professionals’ knowledge that the VAERS system exists and their willingness to spend time filling out the document which asks for:10
Medical information and history on the patient
The facility where the injection was given
The contact information on the person completing the form
The vaccine type, manufacturer and lot number
The best doctor or healthcare professional to contact about the adverse event
What area of the body where the vaccine was injected
A description of the adverse events and treatment
The results or outcome of the adverse events
Medical tests and laboratory results that were done
Any vaccines that were given in the month before the genetic therapy injection was given.
The manufacturer, lot number and site where those additional injections were given
Any adverse events to any previous vaccines the patient may have had
The patient’s race and ethnicity
The date and time the adverse event started
The patient’s age at the time of vaccination
Allergies to medications, foods or other products
Whether the patient was pregnant at the time of vaccination
Any illnesses in the month leading up to the vaccination
Any chronic or long-standing health conditions
Any prescriptions, over-the-counter medications, dietary supplements or herbal remedies being taken at the time of vaccination
While much of this information is necessary for data tracking, you can see how the time-consuming nature of filling out this form can easily become overwhelming when doctors have multiple patients with adverse events from the COVID-19 shots.11 Lack of knowledge of the system, and a growing physician shortage12 with subsequent lack of time have also likely contributed to the underreporting factor (URF).
In an early grant report submitted by the U.S. Department of Health and Human Services, which is part of the VAERS system, the writers admitted that:13
“Although 25% of ambulatory patients experience an adverse drug event, less than 0.3% of all adverse drug events and 1-13% of serious events are reported to the Food and Drug Administration (FDA). Likewise, fewer than 1% of vaccine adverse events are reported.”
As of December 3, 2021, there were 946,461 adverse events and 19,886 deaths reported to the system.14 If only 1% of the events are reported, this translates to 94.64 million adverse events and 1.98 million deaths. To ascertain a better estimate of how many people have been injured from the current genetic injection, the issue of the URF was again addressed in a paper published in November 2021.15
The process for defining a new URF was published in a 62-page paper.16 Using an engineering analysis of the available data and judgment based on peer reviewed literature and expertise of the scientists, an underreporting factor of 41 was determined.
Agency Data Show 173% More Children Died From Shot Than Virus
In this short video, you’ll hear just several of the stories of parents who are grieving the loss of their children after giving them a vaccine they were promised would protect them. Many, thinking they were doing the right thing, took an experimental shot and have left devastated parents and families behind.
While evaluating the data, one of the writers of the paper, Steve Kirsch, recognized the gravity of the situation as it relates to the number of children who have died after taking the vaccine versus the number who have died from the illness. CDC data ending December 8, 2021,17 shows 757 children younger than 18 were listed as casualties of COVID-19.
He points out that many of these deaths, like those in adults, are likely children who died with COVID and not from COVID.18 However, to maintain simplicity, he used those numbers for comparison. Then, using data from VAERS ending December 3, 2021, he found 32 deaths from the vaccine.
Using the URF of 41, this suggests there have been 1,312 deaths that are likely to have been caused by the injection as compared to the 757 deaths the CDC records as having been caused by the illness. If you do the math, this means the shot has killed roughly 173% more children than the illness.
Using the same URF of 41 and the current data ending December 3, 2021, from OpenVAERS we can estimate there should have been 38,804,901 reports and 815,326 deaths. This is vitally important as the total number of deaths recorded for COVID-19 as of December 15, 2021. is 795,839.19 This means the shot has currently killed more children and adults than the virus.
Deaths
19,886
815,326
Anaphylaxis
8,432
345,712
Miscarriage
3,230
132,430
Permanently disabled
32,644
1,338,404
Severe allergic reaction
35,009
1,435,369
Hospitalizations
102,857
4,217,134
Bell’s Palsy
11,896
487,736
Myocarditis/Pericarditis
16,918
693,638
Pilot Deaths, Injuries and Shot Mandates Affect Shortage
Pilot deaths and injuries affect commercial flights, logistical distribution of goods and military readiness. In mid-2020, thousands of pilots were laid off or decided to retire when flights were canceled around the country and around the world during lockdowns. Government mandates for the genetic therapy shot have also curbed the hiring of potential aviators.21
It takes up to two years to train a pilot, and Boeing estimates there will be a need for more than 600,000 new pilots over the next two decades. After the release of the shot in 2021, some noted an excessive number of pilot deaths in 2021, versus the number who died in 2019 and 2020.22
As the data on this situation continue to be released, it’s important to note that one Army flight surgeon has also stepped forward to warn that the COVID jab may increase the risk of sudden cardiac death among military pilots.23
Physician Lt. Col. Theresa Long filed an affidavit alleging the Army isn’t following DOD protocols to screen for side effects of myocarditis associated with the Pfizer and Moderna shots. The affidavit is part of a federal lawsuit against the vaccine mandate for the U.S. military. In the affidavit Long claims:24
“… there is no functional myocardial screening currently being conducted … it is my professional opinion that substantial foreseen risks currently exist, which require proper screening of all flight crews. Based on the DOD’s own protocols and studies, the only two valuable methodologies to adequately assess this risk are through MRI imaging or cardio biopsy which must be carried-out.”
In October 2021, The Defender,25 the publication of the Children’s Health Defense, asked a question that many may have overlooked. Are these vaccine mandates that appear to be reducing critical services and personnel, such as pilots, health care providers and first responders, an intentional sabotage designed to weaken America and expand control?
The loss of critical pilots is not only the result of death, but also life-altering disabilities after the shot. The Defender26 covered Sen. Ron Johnson’s, R-Wis., expert panel on COVID vaccine injuries, during which a 33-year-old commercial airline pilot from Cleveland, Mississippi, testified about his injuries.
Cody Flint had been healthy with no underlying medical conditions before receiving Pfizer’s genetic therapy injection. His first dose was February 1, 2021. Within 30 minutes he developed a severe headache that evolved into a burning sensation in his neck. Two days later he realized something wasn’t right, but only after having taken his airplane into the air. He described what happened next:27
“I was starting to develop tunnel vision and my headache was getting worse. Approximately two hours into my flying I pulled my airplane up to turn around and felt an extreme burst of pressure in my ears. Instantly I was nearly blacked out, dizzy, disoriented, nauseous and shaking uncontrollably. By the grace of God, I was able to land my plane without incident, though I do not remember doing this.”
The doctors initially told him he had an attack of vertigo and a severe panic attack. However, without a history of either, and a continuing decline of his medical condition, the doctors then told him that ”only an adverse reaction to the Pfizer vaccination or major head trauma could have caused this much spontaneous damage.”
After one year and numerous spinal taps and two surgeries, Flint shared that the vaccine stole his career and his future. He spent all his savings to pay his medical bills and his family “is on the verge of losing everything we have.”
Statistical Tricks Behind Fear Mongering
It is important to note here that the claims made by Pfizer that the vaccine is 95% effective is not an effectiveness rating you may imagine. You might think that 95% effective means that the shot protects 95 out of 100 people.
But that is something called a relative risk reduction, which actually is the difference in event rates for both groups being studied.28 In other words, it’s the reflection of the number of vaccinated people who got COVID during the trials compared to the number who were not vaccinated. If you look at the absolute risk reduction, which is far more relevant for public health measures, you’ll see that number is actually less than 1%.29
This means that out of 100 people who got the injection, it is effective for less than one person. While this makes the vaccine of dubious benefit, it also speaks to the propaganda and fear-mongering vaccine makers and vaccines stakeholders have used to promote the dangerous shot — especially when the National Institutes of Health says absolute risk reduction “is the most useful way of presenting research results.”30
Experts Are Using Herd Immunity Reasoning to Convince Parents
Since children have little reason to get the COVID shot, health officials are spinning the idea that they should be vaccinated for the sake of herd immunity. They want you to believe that not only should you look at the people around you as vectors of disease, but also that children could be asymptomatic carriers and supposedly silently spreading a deadly disease to Grandma’s house.
What they aren’t telling you, and the media is not covering, are the studies that show children are not driving the pandemic, and in fact appear less likely to transmit COVID-19 than adults.31 The Children’s Health Defense noted:32
“In short, public health leaders say, parents must ‘vaccinate the young to protect the old.’ Given the federal government’s estimate that one vaccine injury results from every 39 vaccines administered, it seems clear that officials expect children to shoulder 100% of the risks of COVID vaccination in exchange for zero benefit.”
Herd immunity occurs when enough people have acquired immunity to an infectious disease so that it no longer is widely spread in the community. This is calculated using a reproductive number or R0.33 This is the estimated number of new infections that may occur from one infected person. R1 means that one person who is infected is expected to infect one other person.
When R0 is below 1 it indicates that cases are declining and R0 above 1 suggests that they are on the rise. While it’s far from an exact science, a person’s susceptibility to infection is known to vary depending on factors including age, health and contacts within the community.
The initial calculation for COVID-19 health intervention tracking was based on assumptions that each person had the same susceptibility and would mix randomly with others in the community. However, a study published in Nature Reviews Immunology34 suggested the herd immunity threshold for COVID-19 may need adjustment since children are less susceptible to the disease. The scientists wrote:35
“Another factor that may feed into a lower herd immunity threshold for COVID-19 is the role of children in viral transmission. Preliminary reports find that children, particularly those younger than 10 years, may be less susceptible and contagious than adults, in which case they may be partially omitted from the computation of herd immunity.”
In other words, the idea that we must vaccinate children to protect adults is not backed by evidence in this illness. After decades of studying vaccine research and holding responsible positions in health care, you would hope that individuals like Dr. Anthony Fauci,36 director of the National Institute of Allergy and Infectious Diseases and Dr. Rochelle Walensky,37 director of the Centers for Disease Control and Prevention, should understand the science.
If an assumption is made that these individuals do understand the science that doesn’t support vaccinating children, and they have at least glanced at the VAERS data collected by the CDC and FDA, then you must ask the question — what is the underlying goal of vaccinating children with a potentially lethal and disabling shot when they have an exceedingly low risk of severe COVID-19 or dying from the illness?
Of the COVID-19 deaths in the U.S., none received adequate and/or early-enough treatment. At least 85% of COVID deaths were preventable
There are three components to SARS-CoV-2 infection: viral replication, cytokine storm and blood clotting, therefore necessitating a multidrug approach, and treatment must begin early to be effective
Research published in 2006 showed hydroxychloroquine reduced viral replication of SARS-CoV-1 (the original SARS virus). It also has well-established anti-inflammatory properties. These two properties help explain its usefulness against COVID-19
There were clear intentional efforts to prevent use of hydroxychloroquine against COVID-19, likely in an effort to make the COVID jabs appear necessary
You cannot get COVID-19 twice; those with natural immunity have robust, long-lasting immunity. The Pfizer COVID shot, meanwhile, has been shown to have undetectable effectiveness 201 days after the second dose and Moderna’s effectiveness reaches zero around day 121
If you could only listen to one podcast to get up to speed on COVD-19, you are in luck as one of the top clinicians in the world on understanding COVID-19, Dr. Peter McCullough, finally made his way to the largest podcast in the world, Joe Rogan and, as expected, it was epic. You will do yourself a serious disservice if you don’t watch the entire, nearly three-hour, interview at normal speed.
McCullough is an internist, cardiologist and epidemiologist, and in this podcast, he reviews and summarizes what we know about the COVID jabs. McCullough also discusses the importance of early treatment, which has been universally suppressed and ignored from the start.
He’s convinced, and states unequivocally in this interview, that of the COVID-19 deaths in the U.S., none received adequate and/or early-enough treatment. In short, people did not, and certainly don’t now, need to die from this infection, barring some serious underlying condition.
It’s treatable, and later variants, such as Delta and Omicron, appear generally milder than the original virus, resulting in even easier-to-treat illness. From early on, researchers and clinicians demonstrated that early treatment, be it with hydroxychloroquine, ivermectin or steroids and anticoagulants — in some combination — resulted in far better outcomes and saved lives.
When you just let the infection run its course without treatment, most COVID-19 patients were riddled with blood clots and other complications by the time they were hospitalized. According to McCullough, we know that at least 85% of all COVID deaths could have been avoided with early treatment.
Early Treatment Is Key
In August 2020, McCullough’s landmark paper “Pathophysiological Basis and Rationale for Early Outpatient Treatment of SARS-CoV-2 Infection” was published online in the American Journal of Medicine.1
It was the first published report on how to treat COVID on an outpatient basis and described a comprehensive COVID treatment protocol for frontline doctors. Before this, there were about 4,000 papers discussing the potential benefit of various remedies, but none that actually sought to present a comprehensive protocol for treatment.
A follow-up paper, “Multifaceted Highly Targeted Sequential Multidrug Treatment of Early Ambulatory High-Risk SARS-CoV-2 Infection (COVID-19)” published in Reviews in Cardiovascular Medicine in December 2020,2 became the basis for an AAPS home treatment guide.
Importantly, McCullough and the team of collaborators he put together understood early on that there were three components to this infection: viral replication, cytokine storm and blood clotting, therefore necessitating a multidrug approach.
One drug that gained early attention was hydroxychloroquine, as research published in 2006 showed it reduced viral replication of SARS-CoV-1 (the original SARS virus). It also has well-established anti-inflammatory properties. It’s been routinely used in the treatment of lupus, for example. But as explained by McCullough, there were clear intentional efforts to prevent use of the drug against COVID-19.
The U.S. government refused to release its stockpiles, and doctors were told they’d lose their medical license if they used it. The largest manufacturing plant of hydroxychloroquine even mysteriously burned down, and in South Africa, “mercenaries” were breaking into pharmacies and burning the drug.
In addition to that, a fraudulent paper was published in the journal Lancet, falsely stating that hydroxychloroquine was dangerous. “It looked like it was a step to bury hydroxychloroquine as a treatment,” McCullough says. When focus shifted to ivermectin, that drug also became inaccessible and was widely vilified as “horse paste” in the mainstream media.
Treatment Was Suppressed for a Reason
Considering the overwhelming success doctors have had in treating the infection with these and other drugs, why aren’t hospitals everywhere doing it? Why have health authorities fought against treatment in general, and the use of hydroxychloroquine and ivermectin in particular? In McCullough’s words:
“It seems to me, early on, there was an intentional, very comprehensive suppression of early treatment in order to promote fear, suffering, isolation, hospitalization and death. And it seemed to be completely organized and intentional in order to create acceptance for and then promote mass ‘vaccination.'”
The plan to create acceptance for novel mRNA gene transfer technology in lieu of a conventional vaccine by suppressing treatment options has been explained in detail in Dr. Peter Breggin’s book, “COVID-19 and the Global Predators: We Are the Prey,”3 and Pamela Popper’s book, “COVID Operation: What Happened, Why It Happened and What’s Next.”4 McCullough recommends both, if you want to understand how this was coordinated and planned.
Robert Kennedy Jr.’s book, “The Real Anthony Fauci” also shows, using extensive documentation, that Moderna was working on an mRNA injection for COVID-19 well before the world even knew it existed. He reveals extensive collusion occurred to push this novel gene transfer technology on the world, with devastating effects.
When asked why more doctors aren’t using these early treatment protocols, McCullough points out that of the 1 million or so doctors in the U.S., probably only 500 or so actually understand that viable treatments are being suppressed with the intent to drive uptake of the gene transfer shots. Those relatively few who do understand what’s going on face censorship and the threat of having their medical license removed if they speak out about treatment.
Questions About Reinfection Linger
A widespread concern that Rogan brings up is whether or not you can actually get COVID twice. According to McCullough, the answer is a hard no. You cannot. You might think you have it twice, because you’ve tested positive.
After intense pressure to produce evidence of reinfection, the U.S. Centers for Disease Control and Prevention finally admitted they don’t have a single verified case of someone getting sick with COVID twice.
To prove reinfection, McCullough says, you’d need to have a positive PCR test at a cycle threshold below 28 (not 40 or 45, as is routinely done), and a positive antigen immunoassay test to show that you actually had antibodies from the first infection, and a gene sequencing test showing you in fact have the SARS-CoV-2 virus.
What’s more, dozens of studies confirm that natural immunity is robust and long-lasting. “So why is there so much resistance to the idea that people have natural immunity?” Rogan asks, to which McCullough replies, “All roads lead to the ‘vaccine.'”
Dr. Robert Malone disagrees with McCullough on this issue, pointing to a December 4, 2021, study showing 12% out of a sample of 1,200 individuals experienced COVID reinfection.5 In a Twitter post, Malone said:6
“I have caught it twice, as has my wife. I was asymptomatic, she was not. This is a rapidly mutating RNA virus. Just like the common cold. The symptoms will not be as severe — but yes, people catch it more than once. Even Delta …”
Relative Versus Absolute Risk Reduction
Now, when it comes to the efficacy of these COVID shots, the manufacturers have employed a classic strategy to mislead the masses and make the shots sound far better than they actually are. That strategy is looking at relative risk reduction rather than absolute risk reduction.
While the COVID shots boasted efficacy rates between 67% and 95% at the outset, those were the relative risk reductions. The four available COVID shots in the U.S. provide an absolute risk reduction between just 0.7% and 1.3%.7,8
Now, compare that to the noninstitutionalized infection fatality ratio across age groups, which is 0.26%.9 Since the absolute risk that needs to be overcome is lower than the absolute risk reduction these injections can provide, mass vaccination simply cannot have a favorable impact. Yet here we are, being told to get used to the idea of getting booster shots at ever-increasing intervals. It just doesn’t add up.
Of course, as I’ve reported on several occasions, research and clinical experience clearly show that the effectiveness of these shots rapidly wanes. Six months after the second dose, your protection is nil. Meanwhile, your body continues producing toxic spike protein for at least 15 months after each dose.
Efficacy Rapidly Wanes
McCullough cites a Swedish study10 published October 25, 2021, which looked at data from 842,974 pairs, where each person who had received two COVID jabs was paired and compared against an unvaccinated individual, to see if the vaccinated had fewer symptomatic cases and hospitalizations.
Early on, the double-jabbed appeared to have good protection, but that quickly changed. The Pfizer jab went from 92% effectiveness at Day 15 through 30, to 47% at Day 121 through 180, and zero from Day 201 onward. The Moderna shot had a similar trajectory, being estimated at 59% from Day 181 onward. The AstraZeneca injection had a lower effectiveness out of the gate, waned faster than the mRNA shots, and had no detectable effectiveness as of Day 121.
All the while, millions of Americans have already had COVID11 and have natural immunity that doesn’t wane in this manner. Yet they are being shunned and fired for not complying with COVID jab mandates. Again, it just doesn’t add up. Never before has a vaccine been required for anyone with natural immunity against a disease, and there’s good reason for that. It’s completely illogical.
Just like you don’t need a measles vaccine if you’ve had measles, you don’t need a COVID shot if you’ve had COVID. In fact, you are at increased risk of adverse events if you do take it. Remember, if you already have natural immunity, you’re exposing yourself to the harms of the shot with no hope of benefit.
The Most Dangerous Injections in Medical History
As explained in this interview, the COVID shots are the most dangerous, most lethal drugs ever used — and the U.S. Food and Drug Administration and CDC knew this as early as mid-February, when the deaths reported to the U.S. Vaccine Adverse Events Reporting System (VAERS) hit 182.
Historically, any drug with five unexplained deaths gets a black box warning. At 50 unresolved deaths, it’s pulled from the market altogether. None of that happened here. To this day, the FDA and CDC claim not a single death is attributable to the COVID shots, even as the reported death toll is nearing 20,00012 (including international reports), with half of them occurring within 48 hours of the injection. Eighty percent occur within a week post-injection.
That is simply unheard of. The temporal association is stronger than anything we’ve seen before. McCullough also cites research concluding that in 86% of cases, there was no other explanation for the death other than the COVID shot.
McCullough points out that in any given year, an average of 150 deaths following vaccination are reported to VAERS. That’s 150 deaths from an average of 278 million vaccine doses given.
Here, we had 182 deaths at a point in time when only 27 million doses had been administered. So, you cannot blame it on the volume of shots given. The same trends can be found in other countries’ databases as well, such as the U.K.’s Yellow Card scheme.
What’s more, vaccine side effects are notoriously underreported, so as staggering as the VAERS data are, they’re just the tip of the iceberg. Historically, only 1%13 to 10%14 of adverse effects are reported. For the COVID shots, the underreporting factor has been calculated to be anywhere between 31 and 100. That means that to get a more accurate range, you have to multiply the VAERS number by 31 and 100.
The absolute most-conservative estimate so far is an underreporting factor of five. That estimate came from an FDA whistleblower who used Centers for Medicare and Medicaid Services data to estimate the underreporting in VAERS.15 According to that whistleblower, the number of Americans killed by the shots was at least 45,000 as of July 9, 2021. At that time, VAERS reported 9,048 deaths following COVID injection.
Who’s at Greatest Risk for COVID Jab Side Effects?
As explained by McCullough, one of the reasons for this massive death toll is the fact that the COVID shot introduces an uncontrolled dose of spike protein into your body — a far greater dose than what you get when naturally infected with the virus. And the spike protein is the most lethal part of the virus. It’s responsible for the most problematic symptoms of infection.
So, the shots are killing the same people that would be in dire straits were they infected by the virus. It’s also killing some who would likely fare OK with the wild virus but cannot handle the excessive spike protein load produced by the COVID shot.
Consistent Data Point to Clear and Present Danger
As noted by McCullough, we have a very clear safety signal from VAERS. We also have clear biological plausibility, meaning we can explain why and how people might be harmed by these shots. The data are also internally and externally consistent, within VAERS and databases in other countries. The same patterns are seen everywhere.
Normally association does not mean causality unless very specific criteria are met, and in the case of the COVID jabs, those criteria are indeed met. “We’ve fulfilled what’s called the Bradford Hill criteria for causality,” McCullough says. In other words, we have evidence that the injuries and deaths are not accidental. The COVID shots are indeed injuring and killing people at unprecedented rates, despite what the lying CDC states.
Myocarditis Will Likely Be Widespread
Interestingly, the shots appear to harm men and women differently. Women are having far higher rates of neurological injuries, whereas boys and young men account for some 80% of myocarditis (heart inflammation). Just how bad is the myocarditis wave?
Research published in 201716 calculated the background rate of myocarditis in children and youth, showing it occurs at a rate of four cases per million per year. Assuming there are 60 million American children, the background rate for myocarditis would be 240 cases a year.
How many cases of myocarditis have been reported to VAERS following COVID injection so far? 16,918 as of December 3, 2021,17 and it’s going up by several hundred to a couple of thousand every week. We’re also seeing myocarditis in adult men.
“Doctors have never seen so many cases of myocarditis,” McCullough says. “It is frequent, and it is severe.” Patients require heart medication, and must remain sedentary for extended periods of time. While myocarditis is typically a nonfatal adverse event, it can shave years off your life.
Research published in 2019 showed 13% of myocarditis cases ends up with progressive heart failure. Their hearts just never fully recover from the damage. In the study, another 36% improved but never fully recovered.
“My fear is, some of these kids who develop myocarditis will be in the 13% category where they have progressive left ventricle dysfunction and heart failure,” McCullough says.
While we don’t yet know exactly how COVID jab myocarditis compares to naturally-occurring myocarditis, the data we currently have suggest the damage incurred by the spike protein is rather severe.
According to McCullough, 86% of youth who develop myocarditis in response to the jab are sick enough to require hospitalization. Research also shows young boys are far more likely to be hospitalized with myocarditis than they are being hospitalized with COVID-19, McCullough says.
Reject Boosters
If you’ve taken one or two COVID jabs months ago and nothing bad happened, count your blessings. You’re among the lucky ones. If you persist in taking boosters, however, your luck is probably going to run out at some point. It’s really only a matter of time before the amount of spike protein in your system overwhelms it, producing noticeable damage.
Again, evidence suggests the spike protein may remain for 15 months post-injection. McCullough believes it will last at least a year after each dose. If you start getting boosters every three to six months, you’re never going to get rid of that spike protein.
You’ll be adding more and more with each dose, and it’s the same spike protein that causes problems in COVID-19. If you fear COVID-19, you ought to be just as fearful of the COVID shots, if not more so, as you end up with far more spike protein from the shot than you do from the natural infection.
At this point in time, the evidence is clearly weighing against the COVID shots. They’re causing far more harm than good, especially among children, who are not at high risk of dying from COVID-19 in the first place.
Italian Archbishop Vigano sent a message to the American people. He continues to speak out against the globalist threat this Christmas season.
He shared his message below:
DEAR AMERICAN PEOPLE, DEAR FRIENDS, for two years now, a global coup has been carried out all over the world, planned for some time by an elite group of conspirators enslaved to the interests of international high finance. This coup was made possible by an emergency pandemic that is based on the premise of a virus that has a mortality rate almost analogous to that of any other seasonal flu virus, on the delegitimization and prohibition of effective treatments, and on the distribution of an experimental gene serum which is obviously ineffective, and which also clearly carries with it the danger of serious and even lethal side effects. We all know how much the mainstream media has contributed to supporting the insane pandemic narrative, the interests that are at stake, and the goals of these groups of power: reducing the world population, making those who survive chronically ill, and imposing forms of control that violate the fundamental rights and natural liberties of citizens. And yet, two years after this grotesque farce started, which has claimed more victims than a war and destroyed the social fabric, national economies, and the very foundations of the rule of law, nothing has changed in the policies of Nations and their response to the so-called pandemic.
In a stunning 51-page report, the Canadian Covid Care Alliance — a group of over 500 doctors, scientists and health care professionals — unveils the clinical studies upon which health care leaders around the world based their decisions to approve and then mandate the COVID-19 shots.
For example, did you know that Pfizer’s original trial report of December 2020 actually showed only two months’ worth of safety and efficacy data? Did you know the claim that the shot had a 95% efficacy represented only the “relative” risk reduction, NOT the absolute reduction, i.e., the actual efficacy number, which was 0.84%?
Did you know that Pfizer’s most recent report showed an increase in both illness and deaths — meaning there is no benefit to the shot when compared to the risks? In page after page and chart after chart, this report blows the whistle on all the missteps, deceit and misleading demographics used to justify the COVID shots.
Janci Chunn Lindsay, Ph.D., a molecular biologist and toxicologist, has called for an immediate halt to COVID-19 mRNA and DNA vaccines due to multiple safety concerns
There’s credible concern that the COVID jabs will cross-react with syncytin (a retroviral envelope protein) and reproductive genes in sperm, ova and placenta in ways that may impair fertility and reproductive outcomes
In the case of the COVID shots, important animal studies that help ascertain toxic and systemic effects were not done. We’re now seeing danger signals that are not being heeded. Preliminary safety results of mRNA COVID shots used in pregnant women, published in April 2021, revealed an 82% miscarriage rate when the jab was administered during the first 20 weeks of pregnancy
CDC data reveal more than 300 children between the ages of 12 and 18 have died from myocarditis, a now-recognized side effect of the COVID jab, yet the shot is now authorized for children as young as 5
Since the COVID gene therapies do not prevent infection, but only lessen symptoms, they are actually a treatment, not a prevention. And there are far safer and more effective treatment available, including nebulized peroxide, ozone therapy, and hydroxychloroquine and ivermectin regimens
Janci Chunn Lindsay, Ph.D., is a molecular biologist and toxicologist and director of toxicology and molecular biology for Toxicology Support Services LLC. April 23, 2021, she delivered a three-minute public comment to the U.S. Centers for Disease Control and Prevention’s Advisory Committee on Immunization Practices (ACIP).
Her expertise is analysis of pharmacological dose-responses, mechanistic biology and complex toxicity dynamics. In her ACIP comment (see video below), Lindsay described how she aided the development of a contraceptive vaccine in the 1990s that ended up causing unintended autoimmune destruction and sterility in animals which, despite careful pre-analysis, had not been predicted. She explains:
“We were developing what was meant to be a temporary contraceptive vaccine, which was very attractive because it prevented fertilization rather than preventing implantation — or it should have; that was the idea.
Unfortunately, even though quite a bit of analysis was done in different animal models to make sure that it did not have an autoimmune action, it did end up having an autoimmune action and caused complete ovarian destruction.
Now it’s used in that manner [for permanent sterilization] in dogs, cats and other animals. So, that’s a cautionary tale of how animal studies can help us avoid mistakes in humans when they’re used properly, and when proper animal studies are done.”
We May Be Sterilizing an Entire Generation
At the time, she called for an immediate halt to COVID-19 mRNA and DNA vaccines due to safety concerns on multiple fronts. In particular, she noted there is credible concern that they will cross-react with syncytin (a retroviral envelope protein) and reproductive genes in sperm, ova and placenta in ways that may “impair fertility and reproductive outcomes.”
Not a single study has disproven this hypothesis, she noted. Another theory of how these injections might impair fertility can be found in a 2006 study,1 which showed sperm can take up foreign mRNA, convert it into DNA, and release it as little pellets (plasmids) in the medium around the fertilized egg.
The embryo then takes up these plasmids and carries them (sustains and clones them into many of the daughter cells) throughout its life, even passing them on to future generations. It’s possible that the pseudo-exosomes that are the mRNA contents would be perfect for supplying the sperm with mRNA for the spike protein.
So, potentially, a vaccinated woman who gets pregnant with an embryo that can (via the sperms’ plasmids) synthesize the spike protein according to the instructions in the vaccine, would have an immune capacity to attack that embryo because of the “foreign” protein it displays on its cells. This then would cause a miscarriage.
“We could potentially be sterilizing an entire generation,” Lindsey warned. The fact that there have been live births following COVID-19 vaccination is not proof that these injections do not have a reproductive effect, she said.
Lindsay also pointed out that reports of menstrual irregularities and vaginal hemorrhaging in women who have received the injections number in the thousands,2,3,4 and this too hints at reproductive effects. In this interview, we dive deeper into these mechanisms.
Something Has Gone Horribly Wrong
When asked how she ended up getting so passionately involved in this controversial topic, Lindsay replies:
“I became interested in the issue because science was not making sense anymore. For instance, herd immunity was being redefined. Herd immunity has always been defined by a combination of the natural infection with vaccination practices that work.
Suddenly, herd immunity was changed to only being attained through vaccination, and I knew that that was horribly wrong, yet it was being touted everywhere. It was certainly being touted by [Dr. Anthony] Fauci and others who know better.
Other things were also happening within the scientific world. Two of our top tier journals, The New England Journal of Medicine and The Lancet, published fraudulent hydroxychloroquine studies.
Ostensibly they had gone through peer review, and it should’ve been easy to catch the errors in these studies — as well as many other studies that allow for the emergency use authorization of these gene therapies — and they weren’t caught.
Hydroxychloroquine and ivermectin are very safe. They’ve been used safely in pregnant women and children for decades, and suddenly they were being vilified as if they were not safe. As a toxicologist, I know they are safe.
So, these types of things really piqued my attention along with all of the stuff going on in the background with respect to the New World Order and the agenda set by the World Economic Forum, and our joining into this, along with so many other countries, despite their intent, their materials, which claim life will be changed as we know it.
We will ‘own nothing and be happy [about it]’ in just a few years. All of these things converged for me into a sense that something had gone horribly wrong, that our regulatory institutes were captured, and that our scientific journals were not being honest anymore …
There’s a paper that came out in 2006 called ‘Disease Mitigation Measures in the Control of Pandemic Influenza.’5 This paper is wonderful. It goes through World Health Organization and CDC guidelines on how to react during a pandemic, what works and what doesn’t work, and it clearly points out that masks don’t work.
They knew at that point they don’t work. Travel lockdowns don’t work. It’s a wonderful paper to basically go through everything we have done in response to this pandemic, and say that’s an inappropriate way to respond, and we have scientific data that proves it. So, I encourage everybody to go back to that paper … to really see how crazy we’ve gotten in the mandates that make no scientific sense at all.”
Massive Danger Signal Is Being Ignored
As noted by Lindsay, in the case of the COVID shots, important animal studies that help ascertain toxic and systemic effects were not done. But we’re still seeing danger signals that need to be heeded.
Preliminary safety results of mRNA COVID shots used in pregnant women, based on data from the V-Safe Registry, were published in The New England Journal of Medicine (NEJM) in April 2021.6
According to this paper, the miscarriage rate within the first 20 weeks of pregnancy was 12.5%, which is only slightly above the normal average of 10%. (Looking at statistical data, the risk of miscarriage drops from an overall, average risk rate of 21.3% for the duration of the pregnancy as a whole, to just 5% between Weeks 6 and 7, all the way down to 1% between Weeks 14 and 20.7)
However, there’s a distinct problem with this calculation, as highlighted by Drs. Ira Bernstein and Sanja Jovanovic, and Deann McLeod, HBSc, of Toronto. In a May 28, 2021, letter to the editor, they pointed out that:8
“In table 4, the authors report a rate of spontaneous abortions <20 weeks (SA) of 12.5% (104 abortions/827 completed pregnancies). However, this rate should be based on the number of women who were at risk of an SA due to vaccine receipt and should exclude the 700 women who were vaccinated in their third-trimester (104/127 = 82%).”
In other words, when you exclude women who got the shot in their third trimester (since the third trimester is AFTER week 20 and therefore should not be counted when determining miscarriage rate among those injected BEFORE week 20), the miscarriage rate is a whopping 82%.
Of those 104 miscarriages, 96 of them occurred before 13 weeks of gestation, which strongly suggests that getting a COVID shot during the first trimester is an absolute recipe for disaster.
“They concluded, very fraudulently, in my estimation, that it was safe to vaccinate in the third trimester, and said nothing about the clear safety signal in the first trimester,” Lindsay says. “It’s just so dishonest, so purposefully manipulative.”
As for the women who get the shot in their third trimester, there’s still no telling what the ramifications might be in the long term.
“We just don’t know, and that’s the problem,” Lindsay says. “There are all kinds of things that can go wrong with these types of therapies, and have gone wrong in animal models. We don’t know what will happen in the future for these women or for their children. This could be passed on.
We’re seeing now a lot of mention of constitutive expression, whether that’s failure of the mRNA to degrade or integration into the genome. That’s still being investigated.”
Children Are Dying From COVID Jab-Induced Myocarditis
Lindsay goes on to cite a CDC report that shows more than 300 children between the ages of 12 and 18 have died from myocarditis, a now-recognized side effect of the COVID jab.
We also know, based in part on whistleblower testimony, that more than 50,000 Americans have died within three days of these shots,9,10 and that’s just from one database (the Vaccine Adverse Event Reporting System or VAERS). There are 10 other databases that feed into the CDC that the public does not have access to.
“This many deaths, it’s appalling and alarming,” Lindsay says. “Dr. Peter McCullough says the safety signal for typical vaccines, other than this gene therapy, would’ve been around 186 total. We’re now up to [17,128 reported deaths in VAERS, as of October 15, 202111], but they haven’t paused this in children.
They have not paused this while they’re investigating the myocarditis. Instead, they’re pushing it even more. Has this ever happened before? I mean, does this happen in a scenario where the population is at essentially zero risk for the disease? …
The cardiac deaths alone in perfectly healthy kids, and pulmonary embolism deaths in kids, should’ve stopped this. They are at no risk [from COVID-19]. There is no reason to vaccinate them, absolutely zero reason to give them these gene therapies because they’re at no risk [from the infection] …
You know [the shot] is causing heart failure, pulmonary emboli, cardiac arrest in healthy teenagers, and you’re not pausing to investigate the risk versus reward scenario? Something is horribly wrong.
Unfortunately, our regulatory institutions are not going to stop this. They’ve clearly been captured. It’s something that we’re going to have to do. Vaccinated and non-vaccinated must stand together to say, ‘No, you’re not going to experiment on my children’ …
With the RSV vaccines and the dengue fever vaccines, we had deaths in children that were much fewer in number that stopped those campaigns as well. It’s very, very clear — if you don’t get anything else out of this interview with me, understand that our regulatory and safety agencies have been captured.
They’re not doing their job to protect you or your children. You must not trust them, because they are not doing anything according to practices that used to be adhered to. It’s clear that they’ve been captured and compromised, and I hate to say that. I really hate to say that, but that’s the only logical answer …
We have all these breakthrough cases too. If you look at Michigan, and I’ve actually been privy to some other databases of true death numbers in different states [comparing] those who are vaccinated and those who don’t, and I can tell you that the media is lying with respect to the unvaccinated making up 99% of hospitalizations. They’re absolutely lying.”
How the Jab Can Sabotage Fertility
Getting back to the fertility issue, Lindsay cites a Singaporean study that examined the COVID jab’s ability to interfere with fertility by triggering anti-syncytin-1. The study included 15 women, two of whom were pregnant. She explains:
“They did something that I had asked to be done a long time ago, which was to measure anti-syncytin antibodies in an ELISA test. The syncytins are conformationally and genetically similar to the [SARS-CoV-2] spike protein, this fusogenic spike protein.
The thought by several experts was that you could have an autoimmune reaction to the syncytins by developing an immune reaction to the spike protein, and then that would prevent successful pregnancy.
But the syncytins are also important in a number of psychological diseases, such as bipolar depression. They’re important on autoimmune disease, lupus and multiple sclerosis. They are present in skeletal muscle. There’s some association with breast cancer. They’re really important ancient retroviral elements.
What this study found was extremely interesting. It found that every single one of these women who had been vaccinated developed autoantibodies to syncytin-1. Now, the authors kind of dismissed this and said, ‘Oh, but we don’t think that those antibodies were high enough to mean anything.’
But there was a clear difference between the pre-gene therapy sera [blood sample] and the post-therapy sera … What it shows is that there is an antibody response, and the significance of it, we don’t really know. But every single one of the women developed an antibody response that was different from the baseline … and I think that’s probably what’s causing some of these pregnancy losses.”
Are COVID Jabs a Population-Wide Immunocontraceptive?
When asked what she thinks the motive behind this mass injection campaign might be, considering the clear danger signals, she replies:
“I certainly think that to discount that it is a form of population-wide contraceptive would be naïve. There’s a paper that came out in 2005. It’s called ‘Evaluation of Fusogenic Trophoblast Surface Epitopes as Targets for Immune Contraception.’12
This paper tried to find contraceptive peptides in persons that had infertility problems already that were isolated to placentation. So, it was taking a backwards approach, getting the sera from people who had fertility problems and trying to see what they had antibodies to that was causing the fertility problems …
This work was sponsored by the WHO and the Rockefeller Foundation [and the National Institutes of Health]. No surprise there. It was then picked up by a company called AplaGen that took it to patent in 2007.
These are 12-mer peptides, and there’s a series of eight of them that can be used to induce sterility. When they patented it, they also said that it could be used to ameliorate sterility. Interestingly, it was also associated with all of the things that we know syncytin is associated with, — lupus, skeletal muscle disorders, bipolar depression [and] a number of other things.
Even though they don’t name syncytin proteins as the proteins that are targeted, they worked backwards from these peptides, and then said they were a series of other proteins. Sometimes we know that proteins can be called the same thing in different discovery realms. So, that’s going to take more research, but it was certainly interesting to me.
What it really points out is that there were efforts to use peptides or immunocontraceptive means at the placental trophoblast interface to cause sterilization … So, it would be naïve to think that this was not on the plate for future use.”
How Long Will Effects Last?
An obvious question is, how long might these effects last? Are they lifelong? Of course, any answer we come up with here will be hypothetical only, as the studies simply haven’t been done. That said, with her background in molecular biology, Lindsay is at least qualified to theorize.
The mRNA is extremely fragile, which is why a nanolipid with polyethylene glycol delivery system is used. In addition, about 30% of the mRNA has been genetically modified to decrease degradation. As a result, the mRNA being injected is magnitudes sturdier than natural mRNA.
What’s more, the nanoliposomes allow for superior penetration into tissues, and we now know it spreads throughout your body. It doesn’t stay in your deltoid. How long this modified and stabilized mRNA remains viable is still unknown, however. A corollary question is whether this mRNA might be integrated into your genome to become a permanent fixture.
“The answer is, we don’t know for sure,” Lindsay says. “Of course, with the adenoviral vector vaccines [Janssen and AstraZeneca], they’re more prone to integration into the genome. We know that from animal studies and past experiments.
With the mRNA technology, we’ve never stabilized something like this in this manner. What we do know is that recent studies have come out — Bruce Patterson’s group and another group — both came out with the finding that the spike protein is being expressed, [it’s] present on monocytes, as far out as from the time that the people were given the gene therapy.
So, that gives us an indication that it is resistant, for sure, to degradation. The longer it stays around, and is resistant to degradation, the more likely that genomic integration events can occur. But I don’t know the answer to whether or not it will become a permanent feature.”
Make a Rational Choice
As explained by Lindsay, no coronavirus vaccine has ever been successfully brought to market, despite 20 years of effort. All have failed due to antibody dependent enhancement, where the vaccination facilitates infection rather than protects against it.
Now, we’re to believe a safe and effective coronavirus “vaccine” has been developed in mere months. She also makes another important point. Since the COVID gene therapies do not prevent infection, but only lessen symptoms, they are actually a treatment, not a prevention.
And there are far safer and more effective treatments available, including nebulized peroxide, ozone therapy, and hydroxychloroquine and ivermectin regimens.
“If all these gene therapies do is lessen the diseases, then they’re not a vaccine, they are a treatment,” she says. “They are a treatment that you don’t know the mid- or long-term consequences of, that have already caused a number of adverse events. You have to use your common sense to say, why wouldn’t I use a treatment that has been known to be safe over 70 years as opposed to one that is brand-new, that is experimental?”
Other Safety Signals
Aside from fertility issues, heart inflammation and blood clots, another side effect seen among the fully “vaccinated” is de novo Type 1 diabetes in adults. This makes sense considering Pfizer’s biodistribution study showed the spike protein accumulates in the pancreas. The natural SARS-CoV infection can also have this effect.
Type 1 diabetes is a serious problem, as it leaves you metabolically handicapped for the rest of your life, dependent on extremely costly insulin injections. Doctors are also reporting an increase in pancreatic cancer and acute myeloid leukemia.
Where Do We Go From Here?
“Many scientists and physicians feel as I do, and are trying to figure out where we go from here,” Lindsay says, “because our typical safety and regulatory agencies have been compromised.” She believes we need to continue sharing the data and facts that mainstream media refuse to discuss, and continue urging those who have received the jab to at least protect their children.
“We need to stand together as one people and say we’re not going to accept this, especially not for our children, and try to get to the bottom of this and see what’s really behind all these efforts. Is it really about a virus, or is it more about other political motivations and campaigns, as it seems to be?”
I’m less optimistic about the idea of breaking through the brainwashing to get people to not sacrifice their children. So many have their minds set in cement with the wrong information. They could have their brother, sister, mother or father get the shot and die with the needle still on their arm, and they’d still go out to get a booster the next day.
I’ve seen it so many times. My friends, their parents, their siblings and loved ones — there’s this barrier that prevents any openness to new information. They’ve made their decision. Mark Twain said, “It’s far easier to fool someone than to convince them they’ve been fooled.” And it’s true.
So, while I agree that we must keep trying, and have faith that truth will prevail, I also think it’s important to have realistic expectations. We’re up against the most effective propaganda campaign in modern history. It’s psychological warfare at its best.
From my perspective, being a pragmatic realist, I believe the best strategy is to reinforce and support those who didn’t buy into the propaganda narrative to begin with, because they don’t struggle with that cognitive dissonance. If we stick together and support each other, so none of us get sucked into the lunacy, then we can at least preserve the control group.
Ultimately, the truth will come out, as long as we can preserve the control group. In a year or two, or three, we will clearly be able to tell how devastating this intervention was simply by comparing the two groups. I suspect those who got the shot will be severely crippled in various ways, and those who didn’t get the shot will have far better health in comparison.
“I absolutely agree that we have to preserve a control group. We also have to think of ways that we can help those that have been injured. I brought this out in a letter I recently wrote, advocating for Dr. McCullough.
People who have gotten this inoculation, if they have mid- to long-term effects, if you deny that any adverse effects are really going on, then the efforts going into those treatments for people who are having side effects are not going to be there. We have to accept that these [side effects] are real in order to help people who have already taken the inoculations, and I believe we have to try.”
The U.S. Vaccine Adverse Event Reporting System (VAERS) is among the best adverse event data collection systems in the world, but it’s antiquated and difficult to use. Still, it’s a good way to detect safety signals that weren’t detected during premarket testing or clinical trials
There are unmistakable, unprecedented safety signals in VAERS for the COVID shots. While the U.S. Food and Drug Administration and Centers for Disease Control and Prevention claim no deaths can be attributed to the COVID jabs, it’s impossible to discount 8,986 deaths in the U.S. territories alone, reported as of November 26, 2021
The estimated underreporting factor for COVID jab injuries in VAERS is between 31 and 100, so the actual death toll in the U.S. could be anywhere from 278,500 to 898,600
There’s a strong safety signal for female reproductive issues and for heart inflammation (myocarditis) in young men and boys. VAERS data show an inverse relationship between myocarditis and age, with youths being more frequently affected than older men
VAERS data are being deleted without explanation. Each week, about 100 or so reports are routinely deleted, so there are now thousands of inexplicably missing reports
Jessica Rose, Ph.D., a research fellow at the Institute for Pure and Applied Knowledge in Israel, has taken a deep-dive into the U.S. Vaccine Adverse Events Reporting System (VAERS), and in this interview she shares the details of what she’s finding.
VAERS, despite flaws and drawbacks, is one of the greatest tools we have to evaluate vaccine safety. It was implemented as a consequence of the 1986 National Childhood Vaccine Injury Act. While vaccine companies were given blanket immunity against liability for adverse reactions under this law, VAERS was created to collect injury reports in a centralized database so that the post-marketing safety of childhood vaccines could be monitored.
The system was actually launched in 1990, so we have three decades’ worth of data to compare trends against. Granted, vaccine injuries are notoriously underreported. Investigations have found only 10%1 to as little as 1%2,3 of injuries are reported.
When it comes to the COVID jab specifically, calculations4 by Steve Kirsch, executive director of the COVID-19 Early Treatment Fund, suggest injuries are underreported by a factor of 41. But despite that and other shortcomings, VAERS can still provide valuable information about a given vaccine.
Rose is a computational biologist with postdoc degrees in molecular biology and biochemistry. While a native Canadian, she did her postgraduate training in Israel, where she still lives. When her dream of surfing in Australia were dashed due to the COVID-19 outbreak, she decided to start writing code for statistics and graphics, and as the pandemic wore on, she applied those programming skills to the VAERS database.
No, People Are Not Filing Fake Reports
A common attempt to explain away the VAERS data by so-called fact checkers is to say that it’s unreliable because anyone can file a report. This is pure hogwash. Yes, anyone can file a report, but there are penalties for filing a false report, and the filing is time-consuming and exacting. We can be quite certain there’s no over-reporting going on.
It takes on average 30 minutes to fill out a report, and the system is set up in such a way that you cannot save anything until you get to the very end. Even worse, each page will time out after an allotted period of time, forcing you to start from the beginning if you take too long to fill in the details.
“This probably frustrates enough people that they don’t start again,” Rose says. Indeed, the cumbersomeness of the website itself has often been cited as a reason for why doctors don’t report adverse events. Doctors don’t have the time to do it, and most patients don’t know they can file on their own. As noted by Rose:
“[VAERS] is probably one of the best adverse event data collection systems in the world, but it’s completely lamentable. It’s antiquated … Nonetheless … it’s a way to detect safety signals that weren’t detected during premarket testing or clinical trials.
And it is functioning that way, because there are many, many safety signals [about the COVID jabs] being thrown out by the data. For example, everyone’s heard of myocarditis … which is one of the safety signals being thrown off in VAERS. And so, we’ve learned that it happens in young people, more so in boys.”
One explanation for this gender discrepancy has to do with androgens. Testosterone has been shown to facilitate entry of the spike protein into cells by activating a specific enzyme. This could help explain why men, who have higher testosterone levels, are getting myocarditis at much higher rates than women.
Most Lethal ‘Vaccines’ in Medical History
Rose continues:
“I implore everybody to do this … [VAERS] is very accessible. Just go to their website and download the CSV files. You can play with it in Excel, or use whatever is compatible with the CSV file. The OpenVAERS system is even easier to use.
There are three separate files that you can download for the domestic data set, which includes the individual’s data, the symptoms or adverse events that they reported (and it can be up to 15 different types), and the injection data …
You can merge them so that, as per [each] VAERS ID, you have a lot more information … That’s what I did. All you have to do is count the number of adverse events that have occurred in 2021. In the context of the COVID-19 products, exclude all the other vaccines to isolate the signal, and compare the number of adverse events to the total number of adverse events reported in every single year going back 30 years.
There’s absolutely zero comparison. The average number of adverse event reports for the past 10 years is ~39,000, and that includes the adverse event report data for all of the vaccines combined. There are a lot of them …
So we’re looking at about 39,000 total adverse events per year [on average for all vaccines], as opposed to 675,942 [adverse events post COVID jab] in the domestic dataset alone [Editor’s note: Please note that all data are as of the day of the interview and have not been updated prior to publication]. And this does not include the underreporting factor …
We see the same trend when we isolate standalone adverse events like death. There are over 10,000 [post COVID jab] deaths reported now in the domestic dataset alone, not including the underreporting factor, and in the previous 10 years, the average was 155 deaths for the entire year for all the products combined. This is over 6,000% increase in reporting for deaths.
So, the question I’ve been posing to the FDA, the CDC and whoever wants to listen to me is, ‘What’s the cut-off number?’ Because you kind of think of death as being the worst outcome in terms of adverse events in the context of a vaccine or a biological product.
I think there are worse things than death personally. But most people think death is pretty bad. So that’s why I always talk about death in this context. What’s the cut-off number here? How many people have to die in order for these products to be deemed unsafe? So that’s basically all you have to do in VAERS. I mean, you can stop there. You don’t have to look at anything else. But there’s so much more.”
Can Causation Be Established?
While the U.S. Food and Drug Administration and Centers for Disease Control and Prevention outrageously deny that a single death can be attributed to the COVID jabs, it’s simply impossible to discount 19,532 deaths5 (8,986 in the U.S. territories alone6) reported as of November 26, 2021. As noted by Rose:
“It’s not even statistically plausible to say that not one death out of 10,000 was caused [by the shot]. It’s not scientific to say that … Those people, not 100% of them would have died anyway? That’s not how life works.”
The FDA and CDC are also ignoring standard data analyses that can shed light on causation. It’s known as the Bradford Hill criteria — a set of 10 criteria that need to be satisfied in order to show strong evidence of causal relationship. One of the most important of these criteria is temporality, because one thing has to come before the other, and the shorter the duration between two events, the higher the likelihood of a causative effect.
“So, when you’re talking about percentages of people who died within 24 hours of one of these jabs, let’s say you’re talking 50%,” Rose says. “That’s kind of suspicious to me. [Yet] they completely deny the causal effect. It’s just because of coincidence?”
There’s also a strong safety signal for female reproductive issues. Preliminary post-marketing data showed women who got the jab in the first 20 weeks of pregnancy had a miscarriage rate of 82%.7,8Pfizer’s own data, which Rose analyzed, showed a miscarriage rate of 69% when given during the first 20 weeks. Yet no one is warning pregnant women away from these injections: Quite the contrary — women are being universally lied to.
How to Assess Underreporting
As mentioned, Kirsch has calculated an underreporting factor for post COVID jab events of 41, which is likely quite conservative. Rose’s calculation is even more conservative than that. She explains:
“Steve [Kirsch] and I are good friends. We’ve been working very closely on all of this stuff for a long time. His underreporting factor is 41. He estimated that based on a peer-reviewed publication that estimated anaphylaxis numbers, so he used anaphylaxis as a proxy for death.
What that means is that when you hear us say these numbers, you have to multiply them by 41, if you want to go with Steve’s estimate, or 31, in the case of mine. Mine is the most conservative estimate. I took Pfizer’s Phase 3 clinical trial data that they presented to the FDA.
There were over 18,000 participants in the drug group and the placebo groups, and there were a certain percentage of individuals in each arm that succumbed to a severe adverse event, which includes death, hospitalization, visit to the ER, a life threatening adverse event, disability or birth defect.
So, 0.7% of people in the drug arm succumbed to a severe adverse event according to their data. I used that rate, and multiplied it by the number of people who had been injected with one shot of Pfizer on a certain date, August 10, and that number becomes your expected number of people that would succumb to a severe adverse event based on their data.
So, you take that number and divide it by the number of reports of severe adverse events, and you get a multiplication factor, an underreporting factor. When you use that base dataset, the Pfizer Phase 3 clinical trial data, you get 31. Ronald Kostoff has also published a paper in Toxicology Reports, and his estimate is 100, I believe.
So, whenever you’re talking about the underreporting factor, I think you should talk about it in terms of a range, because each adverse event is going to have their own [underreporting factor] …
I think if people actually knew the reality of what was going on, they would decide very quickly, right now, never to go near these things. This isn’t hearsay. It’s not conjecture. The clinical trials are garbage, and there’s no safety data. I’m not just saying this — it’s very reflective in all of these adverse event data collection systems all over the world.
They’re all saying the same thing, the Yellow Card [system in the U.K.], the U.S. [VAERS], Australia’s [system9]. They’re all saying the same thing. As an example, myocarditis and young boys. You know, it’s not something that you can ignore. There’s a reason why this is happening. It’s because the [shots] are not safe.”
What Are VAERS IDs and Why Are They Missing?
VAERS IDs are the numbers assigned to individual report entries. Aside from underreporting, another oddity that strongly suggests the data are worse than we think is that VAERS IDs are going missing. In other words, case reports are being deleted from the system after they’ve been put in. Rose investigated this after seeing videos saying hundreds, perhaps thousands, of people had their reports deleted.
So, she set out to either confirm or deny whether reports were going missing each week, as data sets are updated weekly. She’s been downloading all the data sets since January 2021, which put her in the unique position of being able to compare the different sets, because when the data set is updated, the old data is overwritten.
Now, there are valid reasons for deleting a VAERS ID. One reason would be if both the doctor and the patient file a report. The two reports then need to be combined, and the ID number of one of the duplicated reports is erased. However, what Rose found is that reports are indeed being deleted that shouldn’t be. She explains:
“The way I was determining if entries, if their IDs, were disappearing was by finding out which VAERS IDs didn’t show up in the next update, because you would assume that every single ID that got into the system would stay in the system. And so, the next update would have that data set and a little more, but that’s not how it works.
There are removals every single week, and they’re not explained. There’s no explanation for these. So, the first thing I did when I found this — and it was over 1,000 [missing IDs] — was to check if a high proportion of these deleted reports were deaths. It wasn’t anything overly suspicious, something like 18%.
Then I checked severe adverse events, then I checked children, because this is a big one that’s happening now. A lot of babies are going missing in VAERS, and they shouldn’t be there [since the COVID shots aren’t being given to babies yet], which is probably why they’re being removed.
So, there wasn’t anything overtly suspicious about the nature of the [missing] IDs. But that’s not even the point. These are people who trusted in these products, and listened to people who are telling them they are safe and effective. They were healthy. They went out and got the shots.
Some of them suffered an adverse event, some of them died. These reports got filed to VAERS, and then they got removed. That’s atrocious. I’m not speculating here, either. This is what is happening. They went through this horrifying experience, which no human should be going through, and then they got disappeared. I don’t even know what the word for that is. It’s appalling.”
Data on Children Are Being Deleted
Rose has also delved into the VAERS data for children. Disturbingly, there are apparently thousands, likely tens of thousands of instances if you factor in underreporting, where the jabs have been given to children that were too young to receive the shot at the time they got it.
At the time she looked into this, there were approximately 5,570 reports with a metric code indicating that the product was given to a patient of inappropriate age. In fact, it was the most frequently occurring adverse event type among young children.
“So, there were so-called medical professionals injecting children without confirming their age,” she says, “and then those children suffered adverse reactions in the thousands. And this doesn’t include the underreporting factor. Some of them died. In the 5- to-11 age group, two of them died. One was 11, one was 13, and the timeframe between the death and the injection in one of the kids was five days, in the other it was one day.
So, this was in close temporal proximity. The part that’s even more disturbing than that is that … something like 60 children had died between the ages of zero and 18, and 38% of those children were under 2. [The next week] that percentage went down to 30%. I’m like, wait now, that was late last week. What happened to them?
There are these enormous inconsistencies in the data. Here’s another one. I have about 100 different files that contain algorithms that run code for specific things, like I have a kid’s file, a cancer file, a prion disease file. So, I run them all with the updated data.
Myocarditis is one of them. And there was this big chunk of data for the 50- to 75-year-olds pertaining to myocarditis reports last week, and this week, it’s one-half. It’s staggeringly obvious that something’s very different in the data. The absolute number of reports went up, but it seems to have shifted somehow.
There could be a plausible explanation. But the fact is there’s no reference at all as to how this data is being shifted around. There’s no record. So, we as the public, have no idea what’s actually going on. All we can say with absolute certainty is that something is going on.”
Myocarditis Report Pulled From Publication
Together with Dr. Peter McCullough, Rose recently wrote and submitted a paper10 on myocarditis cases in VAERS following the COVID jabs to the journal Current Problems in Cardiology. Everything was set for publication when, suddenly, the journal changed its mind and took it down. You can find the pre-proof on Rose’s website. The data clearly show that myocarditis is inversely correlated to age, so the risk gets higher the younger you are.
“Most of the reporting in VAERS was in young boys, aged 15. There was a sixfold difference in reporting following dose one and two, which indicates dose response and/or causal effect. The rate for myocarditis in 12- to 15-year-olds is 19 times above background reporting for the United States, so there’s a lot of stuff in that paper that was really important,” Rose says.
“There are many other papers coming out now that are 100% supporting what we found. It’s not debatable. They [pulled] this paper five days before that FDA meeting for the 5- to 11-year-olds, and I don’t think that was a coincidence, because it would have informed people as to the potential risk of myocarditis in young people. So, of course, they don’t want that, because they already bought 30 million doses for the 5- to 11-year-olds.”
Latent Infections Reactivated
Another common side effect of the jabs is the reactivation of latent infections such as herpes infections and shingles. Rose explains:
“There are a bunch of papers that have come out that lend some ideas as to why this is happening,” Rose says. “One makes the claim that CD8+ T cell populations are becoming compromised. In the acquired branch of the immune system, you have immune cell populations called CD4+ T cells and CD8+ T cells.
Everyone’s heard of HIV/AIDS. So, the idea there is that you have a virus that preferentially infects CD4+ T cells, which are the generals of the immune system. They kind of coordinate all the other cells to do their jobs. If you have a depletion in this type of cell, then the rest of the immune system kind of collapses, because they don’t have their general telling them what to do.
The CD8+ T cells are the killer cells. These cells are in charge of killing virally infected cells, so they’re very important in the context of a viral infection. One of these studies showed that in people post injection, the gene profiles were very different for CD positive T cells.
If we’re talking about going beyond immune dysregulation, if we’re talking about immune dysfunction, if we’re talking about certain immune cells being depleted, that could be a possible reason why you’re seeing a reemergence of a latent viral species, possibly. We’re also seeing cancer resurgences.
Another paper that came out shows that there might be problems in the realm of double-stranded DNA repair. There are two enzymes (BRCA and 53BP1) that have been reported to be impaired that are very important in repairing double stranded DNA breaks, and if you have an impairment of essential proteins that are meant to repair double stranded DNA breaks, you have serious problems.
One of those problems is proliferation of cells. So, whenever you get a certain type of exposure to a virus, say a cold or a flu virus, and it gets the better of you so your acquired immune system kicks in, you get these swollen glands. That is actual populations of T cells proliferating.
If you have stunted proliferative capacities, or if you have an impairment of that process, you don’t have an immune system if it happens in T cell and B cell populations …
So, in addition to the hyperinflammation that the spike protein seems to be inducing all over the body, there’s this immune function impairment. That’s really scary to me. [It’s something] we need to investigate and absolutely another reason why these rollouts should stop right now.”
More Information
To learn more, be sure to peruse Rose’s website, Jessica’s World. There, you’ll find links to videos in which she summarizes her various findings, and a weekly graphic update of the latest VAERS datafor death, female reproductive issues, breakthrough COVID infections, cardiovascular events and immunological events.
Another excellent resource is OpenVAERS, which summarizes the most pertinent VAERS data for you on a weekly basis. If you click on the COVID Vaccine Adverse Event Reports, there’s a sliding bar at the top of the page where you can select to view data either for the U.S. territories only, or all VAERS reports, which includes international reports.
Bill Gates and Anthony Fauci have created a formidable public-private partnership that wields incredible power over the American public, along with global health and food policies
Inspired by Rockefeller’s business model, Bill and Melinda Gates donated $36 billion worth of Microsoft stock to the Bill & Melinda Gates Foundation between 1994 and 2018
Gates also created Bill Gates Investments (BGI), which predominantly invests in multinational food, agriculture, pharmaceutical, energy, telecom and tech companies with global operations
Gates strategically targets BMGF’s charitable gifts to give him control of the international health and agricultural agencies and the media, allowing him to dictate global health and food
Fauci and Gates met in person, shaking hands in 2000 in an agreement to control and expand the global vaccine enterprise
You can read all of the details in Robert F. Kennedy Jr.’s best-selling book, “The Real Anthony Fauci,” which contains more than 2,200 footnotes of referenced data
Bill Gates and Anthony Fauci have become household names in the U.S., their largely sterling reputations protected by a heavily biased press. Less known is the deep partnership between the two — the culmination of which has created a formidable public-private partnership that wields incredible power over the American public, along with global health and food policies.
You can read all of the details in Robert F. Kennedy Jr.’s bestselling book, “The Real Anthony Fauci,” which contains more than 2,200 footnotes backing up its data. It exposes the connection between Gates and Fauci, as well as how Gates patterned his rise to control after John Rockefeller’s empire.
In 1913, Rockefeller created the Rockefeller Foundation, which is largely responsible for creating the Big Pharma-controlled medical paradigm that exists today. The foundation imbued its philosophy, precepts and ideologies into the League of Nations Health Organization, which turned into the World Health Organization.
Now, Gates contributes to WHO via multiple avenues, including the Bill & Melinda Gates Foundation (BMGF) as well as GAVI, which was founded by the Gates Foundation in partnership with WHO, the World Bank and various vaccine manufacturers. Together, this makes Gates WHO’s No. 1 funder.
How Gates Used Rockefeller’s Business Model
Inspired by Rockefeller’s business model, Bill and Melinda Gates donated $36 billion worth of Microsoft stock to the BMGF between 1994 and 2018. Gates also created a separate entity, Bill Gates Investments (BGI), which manages his personal wealth and his foundation’s corpus.
BGI predominantly invests in multinational food, agriculture, pharmaceutical, energy, telecom and tech companies with global operations. Federal tax laws require the BMGF to give away a portion of its foundation assets annually to qualify for tax exemption.
Gates strategically targets BMGF’s charitable gifts to give him control of the international health and agricultural agencies and the media, allowing him to dictate global health and food policies so as to increase profitability of the large multinationals in which he and his foundation hold large investment positions.
As was the case with Rockefeller, whose wealth only grew after his Standard Oil Company was forced to split into 34 different companies, Gates’ strategic gifts have only magnified his wealth. Gates’ personal net worth grew from $63 billion in 2000 to $129.6 billion in 2021,1 his wealth expanding by $23 billion during the 2020 lockdowns alone.2
How Gates Controls the WHO
How does a private citizen, not an elected official, gain so much control over a global health agency like WHO? When it was founded, WHO could decide how to distribute its contributions. Now, 70% of its budget is tied to specific projects, countries or regions, which are dictated by the funders.3 As such, Gates’ priorities are the backbone of WHO, and it wasn’t a coincidence when he said of WHO, “Our priorities, are your priorities.”4
As of 2018, the cumulative contributions from the Gates Foundation and GAVI made “Gates the unofficial top sponsor of the WHO, even before the Trump administration’s 2020 move to cut all his support to the organization,” according to Kennedy. “Plus, Gates also routes funding to WHO through SAGE [Strategic Advisory Group of Experts] and UNICEF and Rotary International bringing his total contributions to over $1 billion.”
These tax-deductible donations give Gates both leverage and control over international health policy, “which he largely directs to serve the profit interest of his pharma partners.”
Further, “Gate’s vaccine obsession has diverted WHO’s program contributions from poverty alleviation, nutrition and clean water to make vaccine uptake its preeminent public health metric. And Gates is not afraid to throw his weight around,” according to Kennedy. “… The sheer magnitude of his foundation’s financial contributions has made Bill Gates an unofficial — albeit unelected — leader of the WHO.” Gates’ power has grown further due to his decadeslong partnership with Fauci.
Fauci’s Immense Power
Alone, both Gates and Fauci wield immense power in their fields. Together, they’re a formidable, if unfortunately nefarious, force.
As the director of the National Institute of Allergy and Infectious Diseases (NIAID) — part of the U.S. National Institutes of Health (NIH) — “Fauci has a $6.1 billion budget that he distributes to colleges and universities to do drug research for various diseases,” Kennedy says. “He has another $1.7 billion that comes from the military to do bioweapons research.”5
This is where Fauci’s power lies: in his capacity to fund, arm, pay, maintain and effectively deploy a large and sprawling standing army. The NIH alone controls an annual $37 billion budget distributed in over 50,000 grants supporting over 300,000 positions globally in medical research.6
The thousands of doctors, hospital administrators, health officials and research virologists whose positions, careers and salaries depend on AIDS dollars flowing from Dr. Fauci, Gates and the Wellcome Trust (Great Britain’s version of the Gates Foundation) are the officers and soldiers in a mercenary army that functions to defend all vaccines and Dr. Fauci’s HIV/AIDS doxologies.
Along with Gates, Fauci had the power to influence funding of U.S. foreign aid to Africa for AIDS, prioritizing that for vaccines and drugs instead of nutrition, sanitation and economic development. Yet, Fauci and his team, funded by Gates, have never created a vaccine for AIDS, despite squandering billions of dollars, and causing uncounted human carnage. In 2020, many of the Gates/Fauci HIV vaccine trials in Africa suddenly became COVID-19 vaccine trials.7
As explained in Kennedy’s book, HIV provided Gates and Fauci a beachhead in Africa for their new brand of medical colonialism and a vehicle for the partners to build and maintain a powerful global network that came to include heads of state, health ministers, international health regulators, the WHO, the World Bank, the World Economic Forum, key leaders from the financial industry and military officials who served as command center of the burgeoning Biosecurity Apparatus.
Their foot soldiers were the army of frontline virologists, vaccinologists, clinicians and hospital administrators who relied on their largesse and acted as the community-based ideological commissars of this crusade.
Fauci ‘Enthusiastic’ About Gates COVID Partnership
April 1, 2020, Fauci spoke with Gates on the phone, according to emails released in 2021. Fauci referred to the phone call in an email to Emilio Emini, the director of the Gates Foundation’s tuberculosis and HIV program, stating, “As I had mentioned to Bill yesterday evening, I am enthusiastic about moving towards a collaborative and hopefully synergistic approach to COVID-19.”8
The email was part of 3,000 emails obtained via a FOIA public records request by the Informed Consent Action Network (ICAN). Despite having no medical degree, Gates has been granted direct access to top government health officials, who regard him as a public health authority. In June 2021, Daily Mail reported:9
“The Gates Foundation has committed at least $1.75 billion toward the global effort to fight the pandemic — a sum that opened doors at the highest levels of government. Following Fauci’s phone call with Gates, the Gates Foundation executive Emini emailed him to follow up and ask ‘how we can coordinate and cross inform each other’s activities.’
‘There’s an obvious need for coordination among the various primary funders or the focus we need to have given the state of the pandemic will become lost through uncoordinated activities,’ Emini wrote.”
Fauci also said he would facilitate a call between Emini and the Biomedical Advanced Research and Development Authority (BARDA),10 which provides funding for vaccine and drug development, promoting “the advanced development of medical countermeasures to protect Americans and respond to 21st century health security threats.”11 Daily Mail continued:12
“The Gates Foundation’s partnership with BARDA resulted in at least one joint funding project. In June 2020, Evidation Health announced that BARDA and the Gates Foundation were financing an effort to ‘develop an early warning algorithm to detect symptoms of COVID-19.’
It’s unclear whether the warning system was ever launched, and Evidation issued no further statements on the project after the initial announcement. Other emails released … make it clear that the Gates Foundation remained actively involved in the NIH’s pandemic response.”
The Fauci-Gates partnership led to $1 billion in increased funding to Gates’ global vaccine programs, even as the NIH budget itself experienced little growth.13 Long before the April 2021 phone call, however, Kennedy’s book reveals that Fauci and Gates met in person, shaking hands in 2000 in an agreement to control and expand the global vaccine enterprise.
Why Haven’t You Heard About This Before?
When you’re one of the richest people in the world, you can buy virtually anything you want — including control of the media so that it only prints favorable press. If you have enough money — and Gates certainly does — you can even get major media companies like ViacomCBS, which runs MTV, VH1, Nickelodeon and BET, among others, to insert your approved PSAs into their programming — and BMGF has.14
Via more than 30,000 grants, Gates has contributed at least $319 million to the media, Alan MacLeod, a senior staff writer for MintPress News, revealed.15 From press and journalism associations to journalistic training, Gates is an overarching keeper of the press, which makes true objective reporting pertaining to Gates himself — or his many initiatives — virtually impossible.16
Speaking with MintPress News, Linsey McGoey, a professor of sociology at the University of Essex, U.K., explained that Gates’ philanthropy comes with a price:17
“Philanthropy can and is being used deliberately to divert attention away from different forms of economic exploitation that underpin global inequality today.
The new ‘philanthrocapitalism’ threatens democracy by increasing the power of the corporate sector at the expense of the public sector organizations, which increasingly face budget squeezes, in part by excessively remunerating for-profit organizations to deliver public services that could be delivered more cheaply without private sector involvement.”
It’s a sentiment Kennedy, who believes Fauci and Gates should be investigated for criminal wrongdoing, has echoed. In an interview, he stated that billionaires are in collusion with media, corporations and politicians in order to increase their tremendous wealth:18
“The most important productive strategy or the big talk around the oligarchs and the intelligence agencies and the pharmaceutical companies who are trying to impoverish us and obliterate democracy, their strategy is to create fear and division.
So orchestrate fear, divide Republicans from Democrats and blacks from whites and get a lot of infighting so nobody notices that they are making themselves billions and billions, while they impoverish the rest of us and execute the controlled demolition of American constitutional democracy.”
For more details on how the Fauci-Gates-Pharma alliance is furthering the agenda of totalitarian control, using unfathomable power and greed — all under the guise of a pandemic — read “The Real Anthony Fauci.”
Doctors who explain clearly why vaccines aren’t safe or effective. The majority are censored by youtube. They are criminals revoking you First Amendment rights. RISE UP AMERICANS AND FIGHT.
The Council for Responsible Nutrition (CRN) and the Natural Products Association (NPA) have filed separate citizen petitions with the FDA requesting that the agency reverse their position on NAC; the agency is now asking for more information on the 58-year-old supplement
According to some legal experts, the actions taken by the FDA are not legal under U.S. code Title 21. The FDA has used the exclusion provision three other times, all of which financially benefited the pharmaceutical industry
While past actions may have opened the door to the most recent attack against NAC, it is not difficult to understand why the FDA chooses now to target NAC, when it has demonstrated effective action against COVID-19
Evidence suggests those with a glutathione deficiency have worse outcomes with COVID-19. NAC is a precursor to glutathione and may help lower the risk of severe disease
NAC can be part of your early at-home treatment that is crucial to lowering the severity of the illness and reducing the risk of long-haul symptoms
N-acetylcysteine (NAC) is a powerful antioxidant that was approved as a drug in September 1963.1 Since that time it’s been used as a nutritional supplement that is not found in natural sources.2 NAC contains the amino acid cysteine, which is a precursor to glutathione, also called “the master antioxidant.”3
Glutathione is made of three amino acids — glutamic acid, glycine and cysteine.4 However, NAC is only available in supplement form. The precursors to NAC can be found in foods that are high in cysteine, which include pork, beef, chicken, eggs, dates and sunflower seeds.5
NAC is used in prescription form as an antidote for acetaminophen-induced hepatotoxicity.6 It is also a powerful mucolytic agent for use in upper respiratory conditions. Memorial Sloan-Kettering7 also lists uses in the treatment of depression, precancers, HIV and AIDS, and to alleviate cancer treatment side effects.
In 2020, NAC made the news when the FDA decided over-the-counter sales of this compound, which at that time had been available for 57 years, should require a physician’s prescription going forward. The FDA issued warning letters8 to seven companies the agency said were illegally selling hangover products. By May 2021, Amazon, which also owns Whole Foods, decided to remove any supplements containing NAC.9
FDA Requests More Information on NAC
As Natural Products Insider reports, the letters warned that NAC could not be “lawfully marketed in dietary supplements because it was first studied as a drug in 1963.”10 The Council for Responsible Nutrition (CRN) sent a letter in December 2020 to the FDA’s Office of Dietary Supplement Programs describing the position as “legally invalid.”11
The CRN and the Natural Products Association (NPA) filed separate citizen petitions with the FDA. The CRN letter in December 2020 challenged the FDA’s determination that NAC should be precluded from supplementary use.12 They then filed a citizen position petition June 1, 2021, requesting the FDA reverse their position and outlining why this sudden policy change is “legally invalid on multiple grounds.”13
The NPA filed a separate citizen petition with the FDA14 requesting that the agency not exclude NAC as a dietary supplement or, alternatively, that the Department of Health and Human Services (HHS) issue a regulation finding NAC is lawful in supplements. While the HHS has the authority, it has not been used in the 27 years since the law giving the HHS such power was enacted in 1994.
November 24, 2021, the FDA announced they were requesting more information about how NAC has been marketed as a dietary supplement.15 Natural Products Insider reports that this was encouraging to some in the industry as it signaled the FDA was open to the idea of issuing the regulation that NAC is a lawful ingredient in supplements.16 The FDA called this:17
“… tentative responses to both citizen petitions, requesting additional information from the petitioners … and noting that the agency needs additional time to carefully and thoroughly review the complex questions posed in these petitions.”
The FDA18 also requested information and data on the date that NAC was first marketed as a dietary supplement, reports of adverse events and details on how the products are marketed and sold. The data are requested by January 25, 2022. Steve Mister, president and CEO of CRN said in a statement:19
“The provisions of the Dietary Supplement Health and Education Act of 1994 (DSHEA) may not be interpreted retroactively to remove ingredients that were lawfully marketed in 1994 and have enjoyed a long history of safe use since then. The delay in clearing up the status of NAC by asking for more data and refusing to admit its error disregards the law and disserves consumers who use NAC.
This is not a complicated determination for the FDA to make. DSHEA makes clear that ingredients in use as dietary supplement ingredients prior to its enactment are grandfathered into the supplement marketplace. Thus, pharmaceutical manufacturers could not have had any expectation of exclusivity in the years prior to the creation of this provision of the law.
Given the long history of safe use of NAC, FDA cannot now try to establish a safety concern in order to award this ingredient exclusively to drug makers.”
FDA First Used Legally Questionable Drug Exclusion Provision
U.S. code Title 21,20 specifically defines what a dietary supplement is and is not. According to experts, the actions of the FDA in banning the sale of NAC and finding it a “medication” is illegal under the law. Attorney Stan Soper21 writes that under Title 21 §321 paragraph (ff)(3)(b)10 the actions of the FDA do not meet the Drug Exclusion Provision.
According to Soper,22 the exclusion provision has only been invoked a few times, specifically when used to keep red yeast rice, vitamin B6 and cannabidiol (CBD) from being sold as supplements. In each of these cases there was a potential pharmaceutical financial loss that triggered the assertion the supplement was illegal.
In the case of red yeast rice, it contains a naturally occurring substance that acts in a similar manner to Lovastatin, a statin medication.23 In 2005, drug manufacturer Biostratum filed an investigational new drug (IND) application with the FDA to use vitamin B6 in the treatment of diabetic kidney disease.
Their argument was there was “no evidence that it was marketed as a dietary supplement or food prior to its IND and Phase II investigations.”24 In 2009 the FDA declared vitamin B6 was not a dietary supplement despite documentation that it had been sold as such before the IND application.
The FDA has also invoked the Drug Exclusion Provision against CBD, warning that it is not a legal dietary supplement since there was no meaningful evidence it was marketed as such before drug investigations were approved for Sativex and Epidiolex, which are drugs that contain CBD.
After the 2018 Farm Bill was signed legalizing hemp, then-FDA secretary Dr. Scott Gottlieb made the statement that it was illegal to introduce CBD into the food supply or market it as a supplement.25 Soper postulates26 that the use of the Drug Exclusion Provision against CBD may have opened the door for the FDA to use it against NAC.
Why Take Aim at NAC?
In the citizen petition27 sent to the FDA June 1, 2021, CRN argued that the FDA failed to sufficiently explain this sudden change in policy on NAC, thus “rendering it arbitrary and capricious.” According to CRN, before the seven warning letters in July 2020, “it was FDA’s longstanding policy to permit the marketing of dietary supplements containing NAC.”
Even though the agency had reviewed more than 100 notification structure/function claims for NAC-containing supplements over the years, they never raised the drug exclusion clause. In one response to a petition for a qualified health claim, the FDA had even stated that NAC was considered a dietary supplement.
While the Drug Exclusion Provision on CBD may have opened the door, it still raises the question of why the FDA chose now to target NAC. Historically the provision was used inappropriately to protect the finances of pharmaceutical companies. That is also likely the root of the motivation to ban NAC as a supplement.
As pulmonologist Dr. Roger Seheult succinctly explains in the MedCram video below, NAC is a crucial chemical compound necessary to reduce the oxidative stress associated with severe COVID-19 infections and thus may significantly impact the sales of antiviral drugs. And, as I and other health experts have pointed out in the past, without severe disease, is there truly a need for a vaccine?
Glutathione Depletion Worsens COVID-19 Outcomes
Researchers have been studying NAC since it was discovered. In 2010,28 researchers found that it could inhibit the expression of proinflammatory cytokines in cells that were infected with highly pathogenic H5N1 influenza virus. These same proinflammatory cytokines play a crucial role in severe COVID-19.
Researchers have confirmed that in severe cases, cytokine levels are elevated and once they reach excessive levels it triggers a cytokine storm.29 This causes significant tissue damage that NAC may be able to inhibit. In one 2020 paper,30 the authors describe a case of COVID-19 in a patient with glucose-6-phosphate dehydrogenase (G6PD) deficiency.
This is a genetic disorder that can lead to hemolytic anemia31 and depletes glutathione,32 increasing the risk for human coronavirus infections such as the common cold. NAC was given to the G6PD-deficient patient and nine other COVID patients on ventilators. The NAC “elicited clinical improvement and markedly reduced CRP in all patients.”33
Other published papers have since demonstrated there is a potential use of NAC in the treatment of COVID-19.34,35,36 One 2021 study37 compared consecutive patients hospitalized with moderate or severe COVID-19 pneumonia.
One group received only standard care and the other group received 600 mg of NAC twice daily for 14 days. There were 42 in the NAC group and 40 in the control group. Treatment with NAC led to lower rates of severe respiratory failure and significantly lower mortality rates.
Early at Home Treatment Is Crucial
NAC is only one in a line of treatment modalities that have proven to be successful but have been vilified by governmental agencies. Since the start of this pandemic, it seems global and national health authorities have done everything in their power to discourage and prevent people from accessing treatments, such as ivermectin38,39,40 and hydroxychloroquine,41,42,43,44 that compete with the COVID jab.
The actions around NAC appear to be yet another shameful attempt to prevent patients from helping themselves. By limiting access to nutritional supplements that have demonstrated the capability of reducing severity of the infection, agencies are essentially boosting the risk that infections progress into more serious cases.
Should you come down with symptoms of COVID-19, early treatment is crucial. Not only can it significantly reduce the length of time that you’re sick, but early treatment will also minimize your risk of long-hauler syndrome,45 which can include symptoms that last much longer than the original infection.46 This can include cough, body aches, difficulty sleeping, headaches and brain fog.
There is also scientific evidence that NAC can improve a variety of lung problems, including pneumonia and acute respiratory distress syndrome (ARDS), common characteristics of COVID-19. For example:
Research47 published in 2018 found NAC reduces oxidative and inflammatory damage in patients with community-acquired pneumonia.
Another 2018 study48 found NAC improves postoperative lung function in patients undergoing liver transplantation.
A 2017 meta-analysis49 found a significant reduction in ICU stays among ARDS patients treated with NAC.
NAC is also a well-known mucolytic used to help clear mucus out of the airways of cystic fibrosis patients.50 Some studies also suggest NAC can help reduce symptoms of COPD and prevent exacerbation of the condition.51
Dr. Robert Malone, the inventor of the mRNA and DNA vaccine core platform technology, shares scientific censorship that’s running rampant in medical journals
Data on repurposing existing drugs to treat COVID-19 is being blocked, rejected and buried
Scientific journals depend on revenue from selling journal reprints to pharmaceutical companies — major financial motivation to print only research that’s favorable to the pharmaceutical industry
Rampant lawlessness, in which rules and regulations about bioethics are being completely disregarded, has taken over
We’re experiencing a threat of global slavery of the entire population to financial interests that can be traced back to BlackRock and the Vanguard Group, the two largest asset management firms in the world
Sonia Elijah with TrialSite News was the first U.K. journalist to interview Dr. Robert Malone, the inventor of the mRNA and DNA vaccine core platform technology.1 That interview was taken down by YouTube within a matter of hours because Malone detailed scientific truths that go against the narrative being pushed globally.2
Her second interview with Malone is above. You can now hear some of the points that have been censored, starting with scientific censorship at medical journals. Malone has had multiple peer-reviewed papers seeking to repurpose existing medications as COVID-19 treatments blocked from publication by journals.
In one example, Malone and colleagues found that combined treatment with celecoxib, a nonsteroidal anti-inflammatory drug, and high-dose famotidine, a heartburn drug sold under the brand name Pepcid, led to improved outcomes among COVID-19 patients, including 100% survival.3 It’s been repeatedly rejected for publication.
Malone was also a former guest editor of a special issue of Frontiers in Pharmacology, which published an abstract of a peer-reviewed study by Pierre Kory on ivermectin for COVID-19 — until it was pulled due to a third-party complaint, with no chance for resubmission.
“That was completely inexplicable,” Malone said. “Some third party complained to Frontiers and successfully had that pulled, even though it had passed peer review with an expert panel of peer reviewers including senior reviewers from the FDA.”4
A Coordinated Attack on Dissenters
Working in tandem with scientific censorship is a modern-day witch hunt targeting physicians. Malone describes it as a three-step process in which, first, third parties complain about physicians who are treating COVID-19 patients early on in the disease. “It’s almost never patients” who complain, Malone says, but once the third-party complaint is made, medical boards are obligated to open an investigation.
“Basically, physicians are accused of … the sin of administering licensed drugs off-label, which is about 30% of all prescriptions are off label. Then, then these complaints are filed with the medical boards,” he said. Once the investigation process is initiated, the press is alerted, which subsequently writes multiple articles about the physician being investigated, destroying their reputation.
“This destroys the credibility of the physician,” Malone said. “They’re typically fired from their hospital for creating a controversy. Often they are kicked out of their medical practice group and basically are forced to become free agents.”5 It’s a systematic attack that deprives those accused of their ability to earn a living, while frightening others who might speak out into remaining silent.
Meanwhile, scientific journals have financial motivation to print only research that’s favorable to the pharmaceutical industry. “They don’t have to advertise or buy stock in one of these companies,” Malone said. “What they do is buy very large numbers of reprints of papers that are favorable to their position.”
The reprints “don’t come cheaply,” which means “the journals end up with a large fraction of their revenue coming from the sale of these reprints to pharmaceutical companies.” The pharmaceutical companies hand the reprints out to physicians’ offices, and the scientific journals rely on this revenue — a major motivation to continue printing research that’s favorable to Big Pharma.
“It’s another nefarious way that the pharmaceutical industry has figured out how to exert influence by bending the law,” he explains. “They don’t have to disclose the conflict of interest because it’s not a direct payment.”6
High-Level Lawlessness Is Rampant
Malone believes we’ve entered a period of rampant lawlessness, in which rules and regulations about bioethics are being completely disregarded. Experimentation without proper informed consent violates the Nuremberg Code,7 which spells out a set of research ethics principles for human experimentation.
This set of principles was developed to ensure the medical horrors discovered during the Nuremberg trials at the end of World War II would never take place again, but in the current climate of extreme censorship, people are not being informed about the full risks of the shots — which are only beginning to be uncovered.
Even children are now subject to this experimentation. The FDA’s Vaccines and Related Biological Products Advisory Committee (VRBPAC) voted unanimously for emergency use authorization of COVID-19 shots for children ages 5 to 11 years — with one abstention.
The person who abstained is Dr. Michael Kurilla, director of the division of clinical innovation at the National Institutes of Health’s National Center for Advancing Translational Sciences, who said he doesn’t believe all children need a COVID-19 jab.8 Malone explained:9
“The VRBPAC committee … suddenly it’s unanimous with one abstention to go ahead and jab the kids. So who’s the one abstention who is making the position that he’s a conscientious objector? He’s one of Tony Fauci’s leading lieutenants and one of the leading candidates to replace him.
There’s the appearance of him basically staking out a position that will give them a fallback in the event that all this catches up with them. Somebody is going to be having to run the shop, and I think he now has plausible deniability. I think that was all Kabuki theater to give him plausible deniability about his position, his culpability in what’s going on, because he’s one of the leading candidates to take over the NIAID.”
Manipulation of Data at Multiple Levels
Through his professional career, Malone has worked closely with the U.S. government for many years. He’s now trying to speak out about the manipulation of data that’s occurring at multiple levels. “There are strong disincentives for physicians to report information,” he said, including at the local level, and there are also strong incentives for U.S. hospitals to over-report COVID-related deaths.
“The average cost of hospitalized COVID per patient, the average case cost, is between $300,000 and $400,000.” Part of that is driven by the antiviral drug remdesivir, which they’re required to give because it’s the licensed product in the U.S.
“Remdesivir requires a multiday stay in order to provide the infusion,” Malone said. “So by requiring remdesivir, the hospitals are getting more revenue from hospitalized patients. So there is an additional payment if the diagnosis is SARS-CoV-2.”10 He continued:
“So that’s how we end up with these grossly overinflated risk analyses for the virus. And we ended up with grossly underinflated and under-reported vaccine adverse events, because there are so many disincentives to reporting any of them. And then if they even get reported who tests whether or not they’re valid and makes a determination? It’s the CDC … There’s also multiple reports of mass deletion of adverse events by the Israeli government.”
A Threat of Global Slavery
Data that contradict or question the status quo is buried by the media, while the official narrative is pushed to the top. Malone, who travels frequently and has contacts all over the world, has witnessed firsthand that the same scripts are being used by the media globally.
“We end up with these various public service announcements that are coming out from traditional media in which you can virtually overlay the script. And yes, it’s coming from 50 or 75 different outlets simultaneously. And you can overlay the script so that you basically have multiple broadcast anchors reading a script about the threat to democracy, for instance, of anti-vaxxers, and it is all harmonized,” he said.11
If you follow the money, it all traces back to BlackRock and the Vanguard Group, the two largest asset management firms in the world, which also control Big Pharma.12 They’re at the top of a pyramid that controls basically everything, but you don’t hear about their terrifying monopoly because they also own the media.
Blackrock and Vanguard hold large interests in pivotal companies, and Vanguard holds a large share of Blackrock. In turn, Blackrock has been called the “fourth branch of government” by Bloomberg as they are the only private firm that has financial agreements to lend money to the central banking system.13
Aside from world media, the companies controlled by Blackrock and Vanguard span everything from entertainment and airlines to social media and communications. “We’re experiencing a threat of global slavery of the entire population to these financial interests,” Malone said.
The Majority Have Gone Mad
“Science” has become a loaded word, one used as a basis for decisions that affect basic freedoms, life and death itself. We’re now “at war” with a virus, and dissenters to this “war” must be silenced. What’s less clear is who gave these “orders” that dissenters must be silenced. Dr. Peter McCullough, an internist, cardiologist and epidemiologist, has described it as a form of psychosis or a group neurosis.14
Malone also believes a mass psychosis has taken over. “The documentation now about the conspiracy within the government to kill early [COVID-19] treatment is well-documented. It’s well known that we’re in a situation in which a large fraction of the population has literally gone mad.”15 He explained:16
“The governments, out of desperation, are flailing around. That’s what’s really happening is they don’t understand it. They don’t. They think that they have no other options. They are hypnotized into believing that the vaccines work. They’ve been bombarded by all this lobbying and information control and everything else to believe that the vaccines are effective.
Even though we know they aren’t, the data show that they aren’t, it doesn’t matter. You can’t penetrate through them. Why? Because they’ve undergone mass psychosis … the politicians have, they believe that this is the case and they believe that they have to do these [authoritarian] measures because there’s no other option than mass vaccination.”
Think Global, Act Local
The way to circumvent global totalitarian control, Malone says, is to think global and act local. Build communities with the people around you and stay in touch with others, especially older people and others who aren’t internet savvy. Malone also leaves three key points that he believes everyone should know — and which you can share with others in your circle:
No mandated vaccines for children
Recovered, natural immunity is equal to, or better than, the jab
Allow physicians the freedom to practice medicine
In addition, find physicians in your area who are willing to administer early treatments for COVID-19, and download the Front Line COVID-19 Critical Care Working Group (FLCCC) I-MASK+ protocol in the event you do get COVID-19.17 It provides step-by-step instructions on how to prevent and treat the early symptoms of COVID-19.
Impossible Foods, which made headlines for its meatless burgers that “bleed” like real meat, holds 14 patents, with at least 100 more pending
Impossible Foods should be called “Impossible Patents,” according to Seth Itzkan of Soil4Climate, who suggests fake meat products are destroying the environment by perpetuating a harmful reliance on genetically engineered grains while accelerating soil loss and detracting from regenerative agriculture
Impossible Foods’ products are heavily processed and produced in laboratories — not grown in or found in nature
Impossible Foods has even taken aim at regenerative farming practices, which are promoting optimal nutrition and health while at the same time helping to prevent pollution and restore damaged ecosystems
Impossible Foods’ numerous patents reveal that their products are driven by profits, and perhaps the ultimate goal is to replace real meat altogether with a highly lucrative patented product
This article was previously published August 5, 2020, and has been updated with new information.
Fake meat is all the rage, and although plant-based meat alternatives have been on the market for years, the industry is gaining speed, promoting its meatless ‘burgers’ as a sustainable solution to feed the world. The green image is an illusion, however, one predicated on a product that’s the epitome of unnatural.
Impossible Foods, which made headlines for its meatless burgers that “bleed” like real meat, is one of the leaders in the fake meat industry. Its website suggests its plant-based meat is better for you and the planet,1 but eating an Impossible burger is not akin to eating a plate full of vegetables.
Far from it, Impossible Foods should be called “Impossible Patents,” according to Seth Itzkan, environmental futurist and co-founder and co-director of Soil4Climate, who suggests fake meat products are destroying the environment by perpetuating a harmful reliance on genetically engineered (GE) grains while accelerating soil loss and detracting from regenerative agriculture.2
Impossible Foods Holds 14 Patents, Has 100+ Pending
Impossible Foods’ products resemble nothing found in nature. That’s why the company holds 14 patents, with at least 100 more pending. “It’s not food; it’s software, intellectual property — 14 patents, in fact, in each bite of Impossible Burger with over 100 additional patents pending for animal proxies from chicken to fish,” Itzkan told Medium, adding:3
“It’s iFood, the next killer app. Just download your flavor. This is likely the appeal for Bill Gates, their über investor. It’s a food operating system (FOS), a predecessor, perhaps, to a merger with Microsoft. MS-FOOD.
The business model is already etched in Silicon Valley — license core technology (protein synthesis) while seeking vertical integration of supply chains, which, in this case, is not from coders to users, but from genetic engineers to protein seekers.”
Natural foods cannot be patented, but Impossible Foods’ products certainly can be. The Impossible Burger is a meat alternative that’s unlike others on the market due to the addition of soy leghemoglobin, or heme. This, the company says, it what makes meat taste like meat, and, in plants, leghemoglobin is the protein that carries heme, an iron-containing molecule.
Originally, Impossible Foods harvested leghemoglobin from the roots of soy plants, but deemed that method unsustainable. Instead, they turned to genetic engineering, which they use to insert the DNA from soy plants into yeast, creating GE yeast with the gene for soy leghemoglobin.4
Impossible Foods’ products are heavily processed and created in production rooms — not grown in or found in nature. Their science project creations are also heavily protected, as evidenced by the 14 patents assigned to Impossible Foods, uncovered by Itzkan:5
Patent No. 10287568 — Methods for extracting and purifying nondenatured proteins
Patent No. 10273492 — Expression constructs and methods of genetically engineering methylotrophic yeast
Patent No. 10172380 — Ground meat replicas
Patent No. 10172381 — Methods and compositions for consumables
Patent No. 10093913 — Methods for extracting and purifying nondenatured proteins
Patent No. 10039306 — Methods and compositions for consumables
Patent No. 10087434 — Methods for extracting and purifying nondenatured proteins
Patent No. 9943096 — Methods and compositions for affecting the flavor and aroma profile of consumables
Patent No. 9938327 — Expression constructs and methods of genetically engineering methylotrophic yeast
Patent No. 9833768 — Affinity reagents for protein purification
Patent No. 9826772 — Methods and compositions for affecting the flavor and aroma profile of consumables
Patent No. 9808029 — Methods and compositions for affecting the flavor and aroma profile of consumables
Patent No. 9737875 — Affinity reagents for protein purification
Patent No. 9700067 — Methods and compositions for affecting the flavor and aroma profile of consumables
Patent No. 9011949 — Methods and compositions for consumables
Impossible Foods Are Junk Foods
While the industrialized meat production that occurs on the concentrated animal feeding operations (CAFOs) responsible for most meat consumed in the U.S. is an environmental and ethical atrocity, creating fake meat in high-tech laboratory settings is not the answer.
Impossible Foods is only perpetuating the consumption of ultraprocessed foods, of which Americans already eat far too much. Americans not only eat a preponderance of processed food, but 57.9% of it is ultraprocessed6 — products at the far end of the “significantly altered” spectrum that have been robustly linked to obesity,7 ill health and early death.8
Friends of the Earth (FOE), a grassroots environmental group, released a report that posed critical questions about the growing trend toward animal product alternatives. In it they pointed out the highly-processed nature of these products:9
“Various ‘processing aids’ are employed to make some of these products, including organisms (like genetically engineered bacteria, yeast and algae) that produce proteins, and chemicals to extract proteins.
For example, chemicals like hexane are used to extract components of a food, like proteins (from peas, soy, corn etc.) or compounds (from genetically engineered bacteria) to make xanthan gum … disclosure of these ingredients is not required.
Other processing aids (e.g. bacteria, yeast, algae), including those that are genetically engineered to produce proteins, are also not currently required to be disclosed on package labeling. The lack of transparency makes it difficult to assess the inputs and impact of their use.”
Many of these foods, including Impossible Foods’ fake meat, are made with GMO soy, which in itself is ecologically devastating, in part because it’s often planted where essential grasslands and prairies once stood. That soy is heavily sprayed with the cancer-linked herbicide glyphosate, posing additional environmental and potential human health risks.
Not surprisingly, testing by consumer group Moms Across America found the Impossible Burger contains Roundup ingredient glyphosate and its breakdown product AMPA,10 at levels of 11.3 parts per billion — that’s 11 times higher than the glyphosate found in the Beyond Meat Burger,11 the company’s biggest fake meat competitor.
‘There Is No Place for Nature’ at Impossible Foods
Impossible Foods has even taken aim at regenerative farming practices, which are promoting optimal nutrition and health while at the same time helping to prevent pollution and restore damaged ecosystems. Yet, as Itzkan noted:12
“In this software-as-food scenario, there is no place for nature. Manufacturing of Impossible Burger starts with glyphosate-sprayed soy grown on what was once healthy prairie. It is then infused with heme molecules produced by patented yeast in high-tech labs for the blood-like upgrade.
Finally, it ends its journey as a plastic-wrapped puck that some are brave enough to ingest. Just fry with canola oil and the illusion of a meal is complete.”
Impossible Foods also claims that they have a better carbon footprint than live animal farms and hired Quantis, a group of scientists and strategists who help their clients take actions based on scientific evidence, to prove their point.
According to the executive summary published on the Impossible Foods website, their product reduced environmental impact between 87% and 96% in the categories studied, including global warming potential, land occupation and water consumption.13 This, however, compares fake meat to meat from CAFOs, which are notoriously destructive to the environment.
“The pretense that this wealth-concentrating march of the software industry into the food sector is in any way good for people or the environment is predicated on a comparison with only the worst aspects of animal agriculture,” Itzkan said.14
Grass Fed Farms Represent a Truly Regenerative Solution
White Oak Pastures in Bluffton, Georgia, which produces high-quality grass fed products using regenerative grazing practices, commissioned the same analysis by Quantis and published a 33-page study showing comparisons of White Oaks Pastures emissions against conventional beef production.15
While the manufactured fake meat reduced its carbon footprint up to 96% in some categories, White Oaks had a net total emission in the negative numbers as compared to CAFO produced meat. Further, grass fed beef from White Oak Pastures had a carbon footprint that was 111% lower than a typical U.S. CAFO and its regenerative system effectively captured soil carbon, which offset the majority of emissions related to beef production.16
“Within our margin of error,” the report noted, “there is potential that WOP [White Oak Pastures] beef production is climate positive. This would be very rare and it is unusual that there is more benefit to producing something than to simply not produce,”17 but it’s within the realm of possibility when it comes to properly raised grass fed beef. Fake meat produced in a lab simply can’t compare.
“It [the fake meat industry] ignores, entirely, the rapidly growing regenerative movement that is offering so much hope for the planet at this key time, healing landscapes, replenishing aquifers and mitigating fires,” according to Itzkan. “Thus, because of its reliance on grains, tillage, pesticides and fertilizers, fake meat of scale exacerbates depletion of grasslands while undermining a more legitimate solution.”18
Are There Health Risks in Fake Meat?
The drive for plant-based meat alternatives isn’t due to health or even to support vegan or vegetarian diets. Those truly interested in eating a plant-based diet can do so by eating plants, after all, and in so doing can enjoy the many health benefits that eating plant foods provides.
Impossible Foods’ numerous patents reveal that their products are driven by profits, and perhaps the ultimate goal is to replace real meat altogether with a highly lucrative patented product.
It’s already known that the consumption of ultraprocessed food contributes to disease,19 but manufactured fake meat may also pose additional risks. The U.S. Food and Drug Administration, for instance, has raised concerns over the soy leghemoglobin in the Impossible Burger being a possible human allergen.20
Impossible Foods’ scientists also fed leghemoglobin to rats for 28 days to determine the risk of allergic reaction or toxicity. Dana Perls, from Friends of the Earth, pointed out that the rats exhibited alterations in blood chemistry “that could indicate kidney or other health problems,” which the company did not follow up on.21
Consumer Reports senior scientist Michael Hansen added that there are no long-term studies of soy leghemoglobin in humans, even though the process to make it creates at least 45 other proteins as byproducts, which are also consumed and in need of further evaluation.22
The fact is, fake meat cannot replace the complex mix of nutrients found in grass fed beef and other high-quality pastured meats, and it’s likely that consuming ultraprocessed meat alternatives could lead to many of the same health issues that are caused by a processed food diet. To protect your health and the environment, skip pseudofoods that require patents and stick to those found in nature instead.
The Coup of the United States of America occurring right now.
We have to unite as one nation and we have to fight for our freedom. If we don’t control our own bodies then what do we control?
Our constitution has been trashed, ripped up and thrown away. For the Courts to say your case has no standing OR they don’t want to get into this because it is too political is criminal itself. They took an OATH for a Life Appointment that was given to them for the specific reason of avoiding political tensions / pressures.
When Justice is based off of Political preferences, we have some problems. They need to wake up and get this to juries.
The way that the Court Systems and Law Firms play this is by DISCOVERY.
When you file a lawsuit you file a complaint. A complaint is where you say to the other side, “we think that you did this wrong and it is illegal.” “We are asking you the Court to make a decision on if it is illegal and to reward an appropriate remedy.” Then you name the remedies you are asking for. You put this in the Court and the Court will look at it and what the court is supposed to say is let’s go to DISCOVERY.
What is happening is that the other side is saying that we can’t have this and we can’t have that so discovery would be a complete and total waste of time. There is no standing and this whole thing needs to be thrown out.
The Pleading Requirements were met to be very basic. The Courts have decided that they don’t want to deal with these type of issues because they are difficult. It is complicated and it will take more time.
So once the Complaint is filed and assuming you can get past the Motion bullshit, then the Court will issue Discovery. Discovery means that you have to share the Relevant information/issues about the complaint.
It shouldn’t be that complicated but the courts are using this “You have no standing” bullshit because they don’t want to get involved because it could take more work, cause more attention directed their way and they are afraid of offending the wrong politicians in fear they could lose their jobs and pensions.
Everything is being run off of FEAR – False Evidence Appearing Real.
So what do they do? They FEAR – Forget Everything and Run.
What should they be doing? FEAR – Face Everything and Rise.
Our Constitution has been infringed upon. They have shut down our churches and our business. They have forced vaccinations for employment. They have forced our children to wear masks. They have changed laws to help them do this. They changed the definition of a Vaccine so they could call their experimental mRNA drug a vaccine. Why did they want it to be a Vaccine? The pharmaceuticals have an indemnification agreement in which they can not be held liable for a VACCINE injury, thus why they had to call it a vaccine.
The 2022 election will be HUGE. If we allow them to cheat once again it is over for us forever. They will take complete control and change ALL laws that protect us.
This IS a Coup of some very bad guys taking over our country and to initiate the New World Order by 2025.
The COVID Lie is being exposed more and more daily. Omicron is the VACCINE Variant, not a virus variant.
When they approved the Vaccine for children, about the same time, they say we find a mutant variant that is very strange. VAED – vaccine associated enhanced disease may present severe or very unusual clinical manifestations of Covid-19.
Where did this come from? It came from the Pfizer’s own documents that Thomas Renz just received from the FOIA – Freedom of Information Act.
Now, we know that Pfizer and Moderna and the rest of vaccine manufacturers are not liable if the vaccine accidentally hurts or kills people… BUT, what if they are INTENTIONALLY hurting and killing people?
Are they immune from liability if they knew the vaccine would hurt people?
NO, if they have or had knowledge in any way that this vaccine would hurt people they are NO longer immune from liability. Knowledge of an intentional crime vitiates all contracts of liability immunity.
There is NO immunity for Willful Misconduct. That is EXACTLY what will bring these bastards down. But the court system is very slow and it kind of follows the overall pulse of the people. Right now most people believe that Big Pharma is trying to help us.
When lid comes off that Covid was a planned and created event to provide a solution to serve a means towards a communist one world order coup which included controlling the people with vaccine passports – is when things change. When the majority of the people realize this, that is when things change fast.
They know they have to keep the FEAR levels very high as from now on you will learn how Dangerous this Omicron variant is. The propaganda will get very focused and the news anchors will use their Manchurian training to communicate that message loud and clear.
According to Thomas Renz – an attorney fighting for the American People on this attempted coup and genocide – The CDC knew that the vaccines were deadly when they approved them. He says there are 1,223 deaths in less than 2 ½ months.
He says that they pushed this ahead knowingly and immunity is no more.
Thomas says that Gov officials need to be held accountable also. BUT – he says, if he would go after someone like Fauci and he loses, they will come back on him and make him pay for the law fees and he says they will deliberately raise them.
Thomas Renz also says that he is going to eventually sue the media.
Thomas has slides from an old CDC presentation which shows the recipe for success which is how to scare people into taking a vaccine. The measure their success off of the fear and anxiety of society. If societies fear and anxiety levels are graded high, their propaganda campaign has been successful.
Their main objective is to induce fear and anxiety in people so they are forced to act. That action is going for the SOLUTION that they ALREADY had before fear propaganda campaign and that solution is of course multiple vaccinations.
If they can get people to take the vaccines they travel vaccine passports will be EASY to enforce.
The next three years 2022, 2023 and 2024 as the masses wake up and realize what is going on, we will see the most change that has ever happened in such a short period of just three years.
That is the Coup Plan that is being executed very well right as of December 15, 2021.
Despite a scary-sounding name, the Omicron variant appears to be all hype and no real threat. Primary symptoms of infection with this SARS-CoV-2 strain is a couple of days of fatigue, headache, body aches, scratchy throat and intermittent cough
South Africa reports that no patients so far have required oxygen or even hospitalization for their symptoms. All have been very mild. The first four cases in Botswana were all fully vaccinated against COVID-19
Africa’s low vaccination rate is irrationally being blamed for the emergence of Omicron, even though the continent has extremely low levels of spread compared to the U.S., Canada and Europe
A plane with 600 passengers was diverted for testing when the news about Omicron broke; 10% of the passengers were found to have COVID, 13 of the 61 positive passengers had Omicron, while the rest had Delta or some previous strain. So, clearly, vaccine passports are not preventing spread. Fully “vaccinated” people are just as likely to carry and transmit the virus as the unvaccinated
Australia, a test ground for this totalitarian takeover, is quietly trying to pass legislation to expand its digital identity system
The protocol for treating a patient according to the CDC is from Fauci and is on the NIH website for the medical industry. It says do not treat patients with Hydroxychloroquine or Chloroquine as it is bad for the Covid Patients (which by the way is now known that hundreds of doctors are saying they knew better and this helped most patients completely recover and avoid hospitalization within 24 hours). It also says that the only treatment should be Remdesivir.
By the way, Fauci’s NIH in 2005 had a study with Hydroxychloroquine and Coronavirus and it was effective but you will never ever hear about this – first because it works and second because of the cheap cost.
Remdesivir Poisoning is what is killing the patients. This is a genocide. Remdesivir can cause the Kidneys to fail and they are blaming it on Covid. No virus in history has caused Kidney failure like this and it is definitely not the so called “Coronavirus” causing this.
Remdesivir shuts down the kidneys. The kidneys remove water from the body. If the body doesn’t have the water removed it will fill up the lungs. Then they will say you have Covid Pneumonia which is a bunch of bullshit. It is the untested drug Remdesivir that caused the damage.
Once an individual begins drowning in their own fluids because of Remdesivir, the protocol is place the patient on a ventallator.
Once on a Ventilator – this cocktail or very similar will be prescribed:
Here is what they were giving their patients: all of these drugs are used for anesthesia.
There was one more it sounded like Neo which is a thyroid med.
ALL these drugs are being run into the person at the same time. Yeah, what a cocktail. The nurse says if a patient is on this for more than a week they will never wake back up and if they do will have permanent damage.
Did you ever wonder why hospitals and doctors were being SUPER Reimbursed by Insurance for Diagnosing patients with Covid-19? Because there is an agenda and the agenda has absolutely nothing to do with the health of patients, in fact quite the antonym.
A sick patient is a good patient.
All of this could be helped by taking these three prescriptions: Hydroxychloroquine, Ivermectin and Regeneron.
Supplements to be added with this are: Vitamin C – take 3,000 mg every two hours at the beginning of symptoms, Vitamin D 6,000 IU Daily, Zinc – take 30 mg every 4 hours upon onset of symptoms, Licorice Root Tinture – 3 tablespoons every hour – this will help stop the reproduction of the virus in its track and significantly reduce viral load, Cat’s Claw – this will help kill the virus at a pace in which it will NOT cause a cytokine attack, L-lysine- this will help kill the virus – must take 6,000 mg twice daily and Quercetin – this will help the zinc enter the cells to stop the virus.
COSTS: Hydroxychloroquine costs pennies, the average cost is $37 per 100 – 200 mg tablets. The cost for Remdesivir is $3,120 per patient. Hmm, so now we know that Hydroxychloroquine works very, very well (with the addition of zinc as the hydroxychloroquine opens zinc cell channels) – I have at least 10 doctors who have testified on video that they haven’t lost a patient and we now are aware that Remdesivir causes multiple organ failure leading deaths among those with multiple comorbidities and costs about 9 years worth of Hydroxychloroquine just for ONE single dose. Oh, I see, now it makes perfect sense. Are you waking up yet?
Ivermectin may be the drug of choice. Hydroxychloroquine and Ivermectin are the two SAFEST drugs in world drug history. But yet the CDC says to take Remdesivir as the two Safest Drugs in History may cause Harm. For Christ Sake people, Wake the Hell up and at the very least take a look at this for yourselves. The media is lying and controlled. They are given scripts they HAVE to tell the people. It is called propaganda.
Also before you decide to get a jab or get another booster jab, keep this in mind. THE AVERAGE AGE OF SOMEONE DYING FROM COVID-19 IS 82 YEARS OLD
If your personal physician will not prescribe these drugs. Here are doctors who will, and the very first on the list is only $25 charge. https://mrnavac.blogspot.com/2021/09/how-and-where-to-get-ivermectin.html *Note: on the bottom of that page are doctors who prescribe Nationwide if you cannot find your state listed.
‘Quarantine’ is when you restrict the movement of sick people.
‘Tyranny’ is when you restrict the movement of healthy people.
(Natural News) The World Health Organization’s (WHO) VigiBase currently shows that at least 121,559 people who got “vaccinated” for the Wuhan coronavirus (Covid-19) now suffer from one or more psychiatric disorders.
The most common problem is insomnia followed by anxiety, a “confusional state,” sleep disorders, “nervousness,” “disorientation,” “acute stress disorder,” “restlessness,” hallucinations, depression, “depressed mood,” “panic attacks,” “poor sleep quality,” “delirium,” “agitation,” nightmares, “abnormal dreams,” eating disorders, a “psychotic disorder” or “acute psychosis” or “psychotic behavior,” and tic disorder.
VigiBase also shows 213 reports of Near Death Experience following injection, 57 completed suicides and 25 cases of “exploding head syndrome,” a condition that LifeSiteNews describes as “hear[ing] a very loud noise like an explosion, gunshot or cymbals clanging as though it is right next to them.”
Nearly 30,000 cases of psychiatric disorder post-injection have also been reported to the British Yellow Card, an adverse event reporting system in the United Kingdom.
“The virus that causes COVID –SARS-CoV-2 is known to trigger a powerful immune response, which includes the release of large amounts of proinflammatory cytokines,” say case report researchers.
“It has been hypothesized that a COVID-19 triggered cytokine storm may increase the risk of psychosis,” they added, citing 42 reported cases of psychosis linked to this form of inflammation.
Seeing as how the so-called “vaccines” provoke an inflammatory response in recipients, it is believed that this is the cause behind this sharp uptick in psychiatric disorders.
Are covid “vaccines” causing people to become possessed by demons?
A 2018 study, it turns out, found that college-aged students with higher levels of serum interleukin-6 (IL-6) after vaccination showed some of the most severe depressive symptoms. This was before Fauci Flu shots, of course, but the premise is the same.
Another pilot study from 2017 that looked at childhood vaccine records found that kids who were diagnosed with neuropsychotic conditions such as anorexia nervosa, obsessive compulsive disorder (OCD) and tic disorder were more likely than healthy kids to have recently been vaccinated.
Fast-forward to the present time and people who recently got injected for Chinese Germs are flooding hospitals with all sorts of strange new illnesses that authorities are calling “covid.”
At Sharp Memorial Hospital in San Diego, for instance, a formerly healthy young woman in her 20s was rushed to the emergency department for excess urination. Her family also expressed concerns about her not sleeping well and being anxious all the time.
This young woman had no prior history of mental illness, just to be clear. However, she became so convinced that “covid” was “shutting down” her bowels and kidney function that she basically lost the ability to reason.
It turns out that all the psychological terrorism coming from the White House and mainstream media convinced this poor girl that she her body was failing because of some invisible virus.
The next day, this same young woman returned to the hospital complaining about hearing “accusatory voices.” Blood tests revealed that she had two elevated liver enzymes and high blood pressure from the day prior.
Later on, the young woman was found naked in her hospital room defecating all over the floor. The “vaccines,” it appears, caused her to become demon-possessed and completely psychotic.
Doctors tried to give her psychiatric drugs but the problem only worsened. She reportedly became “increasingly psychotic” and catatonic before eventually suffering a grand mal seizure.
“Her memory was intact, and the young woman responded to doctors’ questions, but only in short sentences, in a monotone flat voice,” reported LifeSiteNews. “She was lethargic with lingering symptoms of catatonia. She could walk, but slowly, and had to be prompted to move.”
More of the latest news about the damage being caused by Fauci Flu shots can be found at Genocide.news.
In a search of the Vaccine Adverse Events Reporting System (VAERS) and the CDC’s own data on COVID deaths, Steve Kirsch, executive director of the Vaccine Safety Research Foundation, has found that twice as many children have died after getting the COVID shots, than who have died from the infection itself.
According to the CDC, 757 children have died from COVID; the CDC doesn’t specify if the children died specifically from COVID, or if they died “with” COVID, but “from” a comorbidity such as cancer, diabetes or obesity.
A look at VAERS shows 1,312 deaths that are “highly likely to be caused by the vaccine.” “In short, our health authorities have convinced parents that it’s better to increase the chance of your kid dying than to reduce it,” Kirsch says. “But hey, we’re just getting started since not all the kids under 18 have been vaccinated yet. The authorities are rushing to get all kids vaccinated before anyone figures out what is going on. So expect the numbers to get much higher.”
While world health leaders and politicians cling to the idea that lockdowns, mask mandates and school closures are the only safe way of handling COVID-19, evidence from more than 400 studies show these interventions simply don’t work.
Taking a close look at the real evidence, the Brownstone Institute says it plainly: The COVID pandemic has been steered by politics. It’s evidence of “monumental failure of lockdown policy,” an investigation by Brownstone Institute found.
“It was clear very early on that task forces and medical advisers and decision-makers were not reading the evidence, were not up to speed with the science or data, did not understand the evidence, did not ‘get’ the evidence, and were blinded to the science, often driven by their own prejudices, biases, arrogance, and ego,” Brownstone says.
“They remain ensconced in sheer academic sloppiness and laziness. It was clear that the response was not a public health one. It was a political one from Day 1 and continues today.”
As self-appointed arbiters of medical truth in the state of Tennessee, the Tennessee Medical Board (TMB) has implemented a policy of revoking or suspending doctors’ licenses if the board decided they were spreading misinformation about COVID-19.
That policy has now been removed from the TMB website, although it hasn’t been completely rescinded, Talking Points Memo reports. The action is believed to be in response to Tennessee state Rep. John Ragan (R), who’s been demanding that the policy be rescinded. Ragan co-chairs his chamber’s Joint Government Operations Committee.
Ragan sent three letters to the board warning that the board would be called to appear before the committee if they refused to rescind the policy. His committee can also recommend dissolving the TMB. According to Talking Points, Ragan said he believes the removal from the website is the equivalent of a win, in that “the deletion had the same impact as rolling the policy back.”
Documents that Pfizer, maker of one of the mRNA COVID shots, released under New Zealand’s Freedom of Information Act show that Pfizer not only knew shortly before the rollout of its vaccines that there was “a large increase” in reported adverse events, but that the company also believed the events were probably underreported.
Up until that point, New Zealand was only aware of 21 possible side effects, all of them considered “minor.” But Pfizer’s report shows more than 100, and that means that possibly thousands of problems after the shot that were attributed to unrelated medical events and even as psychosomatic, may indeed have been due to the shot.
“Many of the new 100+ listed new adverse event types now released by Pfizer in this 38-page document pose long term risks to health,” Guy Hatchard, of the Daily Telegraph, said. “Until very recently, the document was being withheld by Pfizer, who maintained it should be kept confidential. There is a strong possibility that very large numbers of New Zealanders will suffer long term injury as a result.”
This 12-minute video features cameos of teenagers and adults alike who have been debilitated by a COVID-19 shot.
Some started with a bit of a headache, but far worse symptoms developed in the days following. What’s most upsetting is that doctors are “very adamant that it’s not the vaccine,” one girl, who was accused of having a mental problem rather than a vaccine reaction, says in the film.
Unfortunately, she’s not alone. Thousands around the world are telling similar stories — including those from people who lost family members to the vaccine.
Australian tennis player Pat Cash talks about how medical professionals convinced his 89-year-old mother to get the COVID-19 injection, and how afterward she had days of headaches culminating with a stroke.
“You’ve got blood on your hands,” he says to the unnamed doctors. She was on her own, in her apartment … then she collapsed on the floor and was resuscitated. And now Cash is angry.
The censorship and shutting down and “debunking” of independent scientists confuses him, too, he says. “What is the reasoning behind all of this? Is it just money?” he asks.
This mom knows what happened to her little boy, and she recounts how he changed from the moment he had his baby well-check shots, beginning with screeching cries and ongoing diarrhea, followed by earaches, infections and a multitude of autoimmune disorders.
He developed food allergies. He stopped smiling, stopped waving and began to drift away from her, this mom says. She laments the decision she made to vaccinate him, but she kept working with him, to help bring him back.
Yet, health professionals act like she’s crazy, and they tell her she needs to just trust them. Even so, mothers are strong, she says, and she encourages mothers everywhere to stay strong, and support their children.
A lack of quality sleep may be associated with nearly every heart-related death, and also may be associated with heart failure, stroke, diabetes and worsening obesity
The pandemic has had an influence on sleep quality; results from a survey show that 71.8% of people with disrupted sleep patterns used technology just before bed
Sleep deprivation is associated with several other health conditions, including atherosclerosis, diabetes, obesity, Alzheimer’s disease and other neurodegenerative conditions
In one survey, it was reported that the average person got just 5.5 hours of sleep each night; sleep quality is impacted by light and EMF pollution, which you can improve
This article was previously published October 8, 2020, and has been updated with new information.
According to the World Health Organization, ischemic heart disease and stroke were the top two causes of death across the world in 2016.1 Although there have been dramatic declines in cardiovascular diseases (CVDs), ailments in this category continue to remain major causes of loss of health and life.2
In the U.S., the CDC’s Division for Heart Disease and Stroke Prevention reports that 1 in every 3 deaths is from heart disease and $1 of every $6 is spent on CVD.3
While the statistics are disturbing, cardiovascular disease can also lead to nonlethal stroke, heart attack, disability, serious illness and a lower quality of life. These conditions can trigger fatigue, depression and related problems.
The American Heart Association tracks seven key health factors and behaviors they believe increase your risk for heart disease and stroke.4 They call these “Life’s Simple 7,” which they measure to track progress toward their goal of improving the cardiovascular health of people in the U.S.
While each of Life’s Simple 7 behaviors and risk factors are important to overall health, they do not address problems with sleep as contributing factors.
Pandemic Interfering With Sleep Hours and Quality
In an interview with KYW radio, Dr. Zeeshan Khan, pulmonologist from the Deborah Heart and Lung Center, talked about sleep disorders and the relationship they have with CVD, especially in the midst of the current pandemic.5 He told the reporter that the International Classification of Sleep Disorders identifies at least 60 diagnoses in seven categories.6
The two most common are insomnia and obstructive sleep apnea. With sustained poor sleep, a person may experience altered judgment, mood swings and impaired cognition. Khan also listed problems with the cardiovascular system and immunity in people who chronically get less than seven hours of sleep each night.
He warned that lack of sleep can lead to problems with a person’s general health. He recommends that on average, people should get seven hours of sleep each night, but he also shared that in America, about 35% of the people get less than that. “We are kind of a sleep-deprived nation,” he said.
Symptoms of disrupted sleep or insomnia can vary depending on the person. Although you may take a 30-minute power nap in the early afternoon, it doesn’t get rid of sleep debt. It may help you feel better in the immediate moment, but it doesn’t impact the effect of sleep debt on your overall health.
Lack of Quality Sleep Is Associated With Cardiac Morbidity
When asked about how long it should take to fall asleep, Khan said the average amount of time is 15 to 20 minutes. However, the time it takes to fall asleep is extended when people take their smartphone or computer to bed with them. Using these devices can disrupt sleep in several ways, including by engaging your mind at a time when it should be slowing down.
Khan advises people to first use nonpharmacological treatments to help them sleep, such as cognitive behavioral therapy, mindfulness, a consistent sleep routine and meditation. He also recommends steering clear of medications as they can be addictive and they only treat the symptom of sleep disruption, not the reason behind it.
Additionally, he recommends steering clear of having a nightcap to help you relax and fall asleep. This is because drinking alcohol before bed may help you fall asleep faster, but in the long term it can have a negative effect on your sleep patterns. He stresses the importance of using a routine to go to sleep to cue your biological clock.
He went on to discuss the problems with sleep apnea, which often overlap with snoring. During snoring the upper airway narrows, which causes vibrations in the membranes. Although most people with sleep apnea snore, not all people who snore have sleep apnea.
When people with diabetes, heart disease or other problems also snore, they should be evaluated for sleep apnea, especially if they start having problems during the day. Sleep apnea lowers the amount of oxygen delivered to the brain, heart and other organs during sleep. According to Khan:7
“Almost every cardiac morbidity you can think of has been linked to sleep apnea. Heart disease, heart failure, arrhythmias, strokes … inflammatory issues like diabetes, worsening obesity — the list can go on and on.”
Sleep Disorders Associated With Using Technology at Night
In a recent study in Sleep Standards, researchers evaluated the results from a survey of 1,062 people across the U.S.8 The objective was to gain an understanding of how technology may have a relationship with sleep disorders.
One key finding was that 71.8% of the respondents who reported a disruption in sleep pattern also used technology just before bed. The researchers separated the participants into five age groups, which represented the total number in the survey. They were:
Generation Z (under 25) — 22.3%
Millennials (26 to 40) — 44.8%
Generation X (41 to 55) — 23.8%
Baby Boomers (56 to 76) — 8.9%
Silent Generation (older than 76) — 0.2%
They also found that those under age 25 were the most likely to have sleep disorders. People who had a sleep disorder averaged five hours of sleep per night and spent up to 20 hours in front of a bright screen each day.9 The participants also reported that they used their technology devices within 30 minutes of bedtime: 70.2% watched television; 59.4% checked social media; 31.8% checked email; and 32.9% played video games.10
Of all the participants, 57.8% said they used cell phones, which was higher than television use at 18.5% or computer use at 14.2%. The highest percentage of participants in the survey had insomnia at 64.3%.
Although sleep apnea was the second most common disorder, it ran a far second at 14%. Other disorders reported in the survey included sleep paralysis, parasomnias, restless leg syndrome and narcolepsy. Although many experts such as Khan recommend steering clear of pharmaceutical remedies to treat insomnia, 51.2% of those surveyed reported using sleeping pills and 47.5% had tried other medications.
Sleep Deprivation Associated With More Health Conditions
Fragmented or disturbed sleep happens when you fall asleep easily but awaken during the night. This may happen frequently, and you go back to sleep easily, or you awaken and have a hard time going back to sleep. This type of sleep pattern can trigger chronic inflammation that contributes to mental health issues and neurological disorders.11
Lack of sleep also affects your immune system by reducing the number of protective cytokines available.12 In addition, it is associated with atherosclerosis, which is the buildup of plaque in the arteries. This may be called “clogged” or “hardened” arteries and can lead to lethal heart disease.
The exact mechanism of poor sleep in inducing atherosclerosis may have been clarified in a study published by UC Berkeley sleep scientists, who found that an increase in neutrophil and monocyte levels during fragmented sleep had an impact on the pathology of atherosclerosis. They wrote:13
“… these findings affirm a pathway in which the quality of human sleep, specifically the degree of fragmentation, raises inflammatory-related white blood cells, thereby conferring increased risk for atherosclerosis. This was true of sleep fragmentation assessed across a week or across a single night, which predicted increasingly higher CAC [Coronary Artery Calcification] score through a mediating association with increased neutrophils.”
Sleep deprivation is also linked to the development of Alzheimer’s disease and other neurodegenerative conditions. A recent animal study from Marche Polytechnic University in Italy revealed that astrocytes in the brain will start to break down healthy nerve synapses when you are chronically sleep deprived.14 They wrote that the results suggested:
“… that like many other stressors, extended sleep disruption may lead to a state of sustained microglia activation, perhaps increasing the brain’s susceptibility to other forms of damage.”
Average Number of Sleep Hours Dropping
For several years Mattress Firm has commissioned a survey on sleep habits and the number of hours people are sleeping each night. The 2019 results show Americans are sleeping less and less. They asked 3,000 adults about their sleep habits, how satisfied they were with their sleep and about the frequency of sleeping and naps. They compared those results to those from 2018.15
What they found was a sad commentary on the speed at which modern society has chosen to live. It seems that getting at least six hours has become more challenging with each passing year. In 2018, results from the survey showed the average person was sleeping six hours and 17 minutes each night, but by 2019 that had dropped to 5.5 hours.16
Experts currently recommend adults from 18 to 65 years sleep consistently from seven to nine hours each night.17 In other words, most people are sleeping at least 1.5 hours less each night than the minimum that experts think is important for optimal health.
While the number of hours you sleep is important, so is the quality. So, it’s even more disheartening to read that 25% of the respondents reported they also “consistently slept poorly in 2019.”18
Since the amount of quality sleep at night was on the decline, it makes sense that respondents reported they took more naps in 2019 than 2018. But, while more were taken, survey findings indicate there were many planned naps that didn’t get taken.
The survey defined a “great night’s sleep” as “quickly falling asleep and staying that way until morning.” There were about 120 nights fitting that criteria. Americans are so desperate for a good night of sleep they said they were willing to “pay $316.61 for just one night of perfect sleep.” This was $26.16 more than in 2018.
Interestingly, the people who reported the best sleep were those who slept on their back or slept with a pet in their bed. While side sleeping was the more common position reported in the survey, these were the same respondents who had the most difficult time getting to sleep.
EMF Pollution Associated With Sleep Hours and Quality
As I’ve written before, your sleep quality may be impacted by several factors, including your sleep pattern, the number of hours you spend sleeping and by the light and electromagnetic pollution in your area. If you’ve ever gone camping, you may have noticed a change in your sleep quality. Chances are you had a deeper sleep and awakened more rested.
Two factors that influence sleeping better outdoors are the drastic reduction in artificial lights and the reduction in electromagnetic fields (EMF). Your circadian clock is affected by your melatonin levels, which in turn are affected by exposure to light at night. You might enjoy the same restful sleep if you install blackout blinds, use a sleep mask and get rid of any light-emitting source in your bedroom.
Electromagnetic fields also may impair sleep quality19 and produce oxidative damage during sleep.20Consider shutting off all your electronic devices and your Wi-Fi modem and router at night to reduce your exposure and improve your sleep quality. For more tips on improving the number of hours you sleep and the quality of your sleep, see “Top 33 Tips to Optimize Your Sleep Routine.”21
According to media reports, the Omicron variant was discovered in Botswana, in four fully “vaccinated” individuals. Physicians in South Africa responded saying that while the variant has been detected, they are not seeing significant illness from it. All cases so far have been mild and none has required hospitalization
Omicron appears to be evading the COVID jab, resulting in breakthrough infections at a higher rate than previous variants. This is a sign that the mass vaccination campaign may be breeding “vaccine” resistance
There’s a curious feature of Omicron, however, that hints at it having been modified in a lab. The closest genetic sequences date back to mid-2020. It doesn’t seem to belong to any of the evolutionary branches that have emerged since
Omicron has 25 nonsynonymous and only one synonymous spike mutation compared to its most recent common ancestor, AV.1. Were it a natural occurrence, that ratio ought to be somewhere between 25 to 50 and 25 to 100
There’s no precedent for this oddity occurring in nature. There is, however, precedent for this in lab-leaked pandemics
In Bannons War Room interview above, Dr. Robert Malone, inventor of the mRNA and DNA vaccine core platform technology,1 reviews what we know so far about the so-called Omicron variant of SARS-CoV-2.
As noted by Malone, the latest media hype actually began with reports of Africa having far lower case rates than the rest of the world, despite its comparatively low COVID jab rate. That was followed by reports in the local press that South Africa was asking Pfizer to halt its shipments of the shots, as they still had plenty and most adults were refusing to take it.
The very next day, “we suddenly had this huge kerfuffle about this new virus strain, and the press was announcing it was coming out of South Africa,” Malone says. The U.K. almost immediately responded by shutting its borders to most of South Africa.
According to media reports, the Omicron variant was discovered in Botswana, in four fully “vaccinated” individuals. Physicians in South Africa responded saying that while the variant has been detected, they are not seeing significant illness from it. All cases so far have been mild and none has required hospitalization.
Coordinated Fear Porn Campaign
In rapid succession, news articles were published proposing the virus evolved in an AIDS patient and appears to spread far easier than previous variants. Calls for concern and the need for new restrictions flooded the airways. As noted by Malone, the press was talking about “everything except for the obvious, which is that this is a ‘vaccine’-escaped mutant.”
Indeed, the variant appears highly resistant to the COVID shots, which is a sign of it having mutated within one or more COVID-jabbed individuals, not in someone with no antibodies at all to attack it.
Remember, viruses mutate primarily in response to insufficient immune responses. Yet among the first recommendations from the mental giants in charge of COVID responses was to push COVID booster shots, which is as irrational as it is unscientific.
“The boosters are a perfect way to bias our immune system so we’re LESS able to respond to this new variant,” Malone explains. “This is [like] jabbing everybody with a flu vaccine from three seasons ago and expecting it to have effects against the current [flu strains].”
Is Omicron Another Lab Creation?
As for the nature and origin of Omicron, Malone says:
“It has the hallmark of a viral agent under tight genetic selection for evolution to escape the ‘vaccine’ responses against the receptor bonding domain. The question that is outstanding right now is — because this is so different from the other strains that are being tracked; it’s in its own separate little evolutionary branch — how did this happen? Why did this suddenly pop up with all these new mutations?”
The mainstream press is pushing the narrative that Omicron’s mutations are due to the low COVID jab rate in South Africa, possibly in combination with it mutating within someone with AIDS. The solution, we’re told, is to blanket Africa with COVID shots, even though the continent has enjoyed a phenomenally low case rate and mortality rate without the jabs. So, clearly, this narrative is trying to achieve an end that simply isn’t warranted by the real-world data.
Aside from shaming South Africa into getting more COVID shots, another potential reason for this narrative is that they want to hide that it’s another lab created virus. As noted by Malone, we have “the looming specter of this being further engineered in some way.”
In all, Omicron is said to have some 50 mutations from the original Alpha strain, many of which specifically allow it to circumvent COVID shot-induced antibody defenses.
While Malone admits he is not closely tracking the mutations of the virus, and is not qualified to speculate on its evolution, he points out there is a subset of experts who believe it may have undergone lab modification because, genetically, it “doesn’t look like it’s part of the prior evolutionary process that we’re seeing with many other strains.”
Until and unless we end up with conclusive proof of its origin, we need to keep all options open, Malone says, and that includes the possibility of Omicron being cooked up in a lab from a previous strain.
Omicron Cases Double in Less Than Five Days
So far, we know as little about Omicron as we did the original SARS-CoV-2 virus when it first emerged. What we do know is that it appears highly infectious, doubling in a median time of 4.8 days, and has significant “vaccine” evasion capabilities.2
According to the Economist,3 which cites data from South Africa’s National Institute for Communicable Diseases, Omicron “appears to have rapidly outcompeted Delta” in South Africa, as of the first week of December 2021 accounting for nearly all positive cases.
Omicron Is a Major Oddity
Time-lapse I made of the genomic epidemiology of SARS-COV-2 since the 2020 Wuhan strain
Notice that Omicron makes a sudden appearance inconsistent with the other variants, and contains the largest number of mutations
One particularly odd feature of Omicron is that the closest genetic sequences date back to mid-2020. It doesn’t seem to belong to any of the evolutionary branches that have emerged since. As noted by professor Trevor Bedford, a computational virologist interviewed by NPR, “This is very rare to see.”4
In a Twitter post, a user named Chief Nerd, shows a time-lapse graphic5 he created that illustrates the genomic epidemiology of SARS-CoV-2 from the original strain until now, using data from nextstrain.org.6
It’s a great illustration of just how odd an unnatural Omicron’s emergence really is. As the time-lapse gets toward the end of 2021, suddenly there’s Omicron, emerging like a straight line from a mid-2020 strain, having no semblance to any of the other strains.
There’s no precedent for this oddity occurring in nature. There is, however, precedent for this in lab-leaked pandemics, such as the 1977 Russian influenza, caused by an H1N1 flu strain that strongly resembled a strain in circulation between 1946 and 1957. There have been persistent rumors that the Russian flu might have been the result of a live-vaccine trial escape.7
Omicron, also known by the designation B.1.1.529., has a ratio of nonsynonymous to synonymous mutations of 25 to 1. According to molecular biologist and cancer geneticist Philip Buckhaults, Ph.D.,8 Omicron has 25 nonsynonymous and only one synonymous spike mutation compared to its most recent common ancestor, AV.1. Were it a natural occurrence, that ratio ought to be somewhere between 25 to 50 and 25 to 100.
Three Hypotheses of Omicron’s Origin
Researchers have tried to explain this phenomenon in a variety of ways. Bedford has suggested the mid-2020 strain might have infected and evolved within some unknown animal population before spilling back into the human population.
It’s an unlikely scenario though, Bedford says, because there ought then to be signs of the animal genetic material in the genome, and we’re not seeing that. Instead, there’s human RNA insertions, which suggests a human host.
Another hypothesis is so-called “cryptic spread” in an unmonitored region. In other words, the mid-2020 strain may have circulated in an area where testing and monitoring of cases were low or absent, allowing it to evolve under the radar, until finally becoming transmissible enough to spread into more monitored regions.
Alas, Bedford finds fault with this explanation as well, “Because it would seem that as [this strain of the virus] was on its path to becoming Omicron and becoming a quite transmissible virus, [the earlier versions] would have started to spread more widely before just now.”9
A third hypothesis involves the incubation in an immunocompromised patient, such as an AIDS patient. If the patient’s immune system was just robust enough to prevent death, but not complete clearance, the virus may have lingered for many months, slowly mutating over time.
The crux here is that the virus ought to have spread from that person earlier. Why did it take well over a year for it to finally be transmitted? Intermediate variants should have emerged, but didn’t. It just suddenly emerged with dozens of mutations already baked in that have no precedent.
Bedford told NPR,10 “That’s a good question and a legitimate one. I don’t have an obvious answer besides chance.” Despite the lack of plausible answers, Bedford believes this scenario may be the most plausible.
Two Elephants in the Room — The Missing Hypotheses
Of course, getting back to Malone’s observation, what’s missing from this list of hypotheses is the most obvious one, which is that the virus mutated in response to the pressure of widespread COVID injections. Also missing is the hypothesis that Omicron was genetically manipulated from a mid-2020 strain, and in one way or another entered into circulation.
Irrationally, Bedford and others are now stressing the importance on ramping up HIV treatment to prevent mutations from occurring in untreated individuals with low immune function, rather than taking a long hard look at how the mass “vaccination” campaign is driving the evolution of this virus and putting COVID jabbed individuals at ever-increasing risk of serious infection.
At present, one of the most plausible theories appears to be that scientists enabled an early SARS-CoV-2 variant to build antibody resistance, possibly by passaging them through human or humanized cell lines in the presence of convalescent plasma.
The Lab in South Africa Experimented on SARS-CoV-2
If Omicron is another lab creation, what lab might be responsible for its creation? A number of internet sleuths have pointed fingers at the biosafety level 3 (BSL3) lab in Durban, South Africa, where research on SARS-CoV-2 was taking place.
A paper titled “Escape of SARS-CoV-2 50IY.V2 from Neutralization by Convalescent Plasma”11 was published in the journal Nature at the end of March 2021. This appears to be just the kind of research that might train the virus to evade COVID antibodies.
The research, funded by the Bill & Melinda Gates Foundation, was conducted by a conglomerate of researchers, most from South Africa, but also one American and several with research credentials at both South African and German, British or American research facilities. Affiliates listed include several research facilities in South Africa, as well as research institutes in Israel, the U.K., U.S., Germany and Brazil.
In a series of December 3, 2021, Twitter posts,12 Yuri Deigin, a drug developer and biotech entrepreneur, points out that the initial emergence of Omicron was in Durban, where the BSL3 lab happens to be located, and where that study was done.
As yet, the Omicron lab leak theory is loosely held together, but if recent history is any indication, we’re bound to start seeing more extensive discussions and reviews of the evidence as we go along.
As noted in an October 10, 2021, New York Post editorial,13 the lab leak theory, referring to the original SARS-CoV-2 virus, “is now almost certainly proved” — and according to David Martin, Ph.D., proved beyond all doubt based on the patent trail, dating back two decades14 — but it took well over a year and a half to get to this point.
While the Omicron origin question is likely to grow, our fear of this variant doesn’t have to. So far, all indications are that Omicron is among the mildest of the variants — highly infectious with rapid spread, but very mild in terms of symptoms.
Dr. Joseph Ladapo was appointed Florida surgeon general and secretary of the Florida Department of Health by Gov. Ron DeSantis September 21, 2021
Ladapo has now issued a statewide public service announcement in support of commonsense COVID prevention strategies such as optimizing your vitamin D, staying active, eating nutrient-dense foods and boosting your immune system with supplements such as vitamin C, quercetin and zinc
Florida Health even highlights emerging treatments such as fluvoxamine and inhaled budesonide. Importantly, Florida Health now states that “Physicians should use their clinical judgment when recommending treatment options for patients’ individualized health care needs. This may include emerging treatment options with appropriate patient informed consent, including off-label use or as part of a clinical trial”
Despite publishing a scientific review on vitamin D for COVID in the peer-reviewed journal Nutrients, and the paper being the second most downloaded article this year, I’ve been vilified and targeted by the U.S. Food and Drug Administration and the Federal Trade Commission for reporting its benefits
The evidence for vitamin D against COVID-19 satisfies Hill’s criteria for causality in a biological system, and dozens of studies have demonstrated vitamin D helps reduce all risks associated with COVID
As a ray of hope in what appears to be an utterly broken medical system, Florida’s new surgeon general, Dr. Joseph Ladapo, has issued a statewide public service announcement in support of commonsense COVID prevention strategies such as optimizing your vitamin D, staying active, eating nutrient-dense foods and boosting your immune system with supplements.
The HealthierYouFL.org website1 now urges Floridians to “Talk to your health care provider about how certain supplements or foods containing vitamins and minerals might help boost your immune system, such as zinc, vitamin D, vitamin C and quercetin.” These are all well-known supplements that have been shown to have a positive impact on your COVID-19 risk.
The surgeon general also supports the use of monoclonal antibodies in acute cases, and as prevention in high-risk patients who have been exposed to COVID-19. Available treatment locations can be found on FloridaHealthCOVID19.gov.
‘Physicians Should Use Clinical Judgment’
Florida Health even highlights emerging treatments such as fluvoxamine and inhaled budesonide. Importantly, Florida Health now states that:2
“Physicians should use their clinical judgment when recommending treatment options for patients’ individualized health care needs. This may include emerging treatment options with appropriate patient informed consent, including off-label use or as part of a clinical trial.”
Well, no one could be happier about this than I. I’ve been calling for vitamin D recommendations since the earliest days of the pandemic — ideally nationwide, but statewide is at least a start, especially considering Florida is the sunshine state. Instead, I’ve been vilified and targeted by the U.S. Food and Drug Administration and mainstream media for reporting its benefits.3,4
The FDA specifically mentioned Vitamin C, Vitamin D and Quercetin in their warning letter. Now that the Florida surgeon general agrees, will they also be warned by the federal authorities?
Ladapo was appointed Florida surgeon general and secretary of the Florida Department of Health by Gov. Ron DeSantis September 21, 2021,5 and it’s refreshing to finally see COVID guidance that makes sense. In his acceptance speech, Ladapo said:6
“I am honored to have been chosen by Governor DeSantis to serve as Florida’s next Surgeon General. We must make health policy decisions rooted in data and not in fear …
I have observed the different approaches taken by governors across the country and I have been impressed by Governor DeSantis’ leadership and determination to ensure that Floridians are afforded all opportunities to maintain their health and wellness, while preserving their freedoms as Americans.”
Vitamin D Papers Top List of Most Popular Studies of the Year
October 31, 2020, I published a scientific review7 in the journal Nutrients, co-written with William Grant, Ph.D., and Dr. Carol Wagner, both of whom are part of the GrassrootsHealth expert vitamin D panel.
As of October 31, 2021, our paper, “Evidence Regarding Vitamin D and Risk of COVID-19 and Its Severity” — which you can download and read for free — was the second most downloaded study from this journal in the past 12 months. It was also No. 2 in citations and No. 4 for views.
The study with the most downloads in the past year and the all-time highest number of views was another vitamin D paper8 by Bhattoa et.al., which found vitamin D supplementation reduced the risk of influenza and COVID-19 infections and deaths. The coauthors of my paper, Grant and Baggerly, were coauthors on this paper as well.
A third vitamin D paper, by Annweiler et.al., also nabbed the No. 1 spot for most-cited study in the past 12 months. This study found vitamin D supplementation improved survival in frail elderly hospitalized with COVID-19.
Clearly, vitamin D has been on the forefront of many minds, and I’m glad the Florida surgeon general recognizes its importance as well. While mainstream media and many so-called health authorities still hold on to the ridiculous claim that there’s “no scientific basis” for the recommendation of vitamin D for COVID, that is just false.
As early as the end of September 2020, data from 14 observational studies — summarized in Table 1 of our paper9 — showed that vitamin D blood levels are inversely correlated with the incidence and/or severity of COVID-19. Many critics of vitamin D will claim that these associations are not causal. However, there are statistical tools such as Bradford Hill that can actually prove causation through these associations are strong enough.
The Bradford Hill criteria are a group of nine principles (i.e., strength of association, consistency of evidence, temporality, biological gradient, plausibility or mechanism of action, and coherence, although coherence still needs to be verified experimentally) that can be useful in establishing epidemiologic evidence of a causal relationship between a presumed cause and an observed effect.
It has been widely used in public health research and has determined that the vitamin D insufficiency for COVID is indeed causal.10
How Vitamin D Protects Against COVID
It’s important to realize that your body is well-equipped to handle just about any infection, provided your immune system is working properly, as that is your body’s first line of defense. Vitamin D receptors are found in a large number of different tissues and cells, including your immune cells. This means vitamin D plays an important role in your immune function specifically.
If vitamin D is lacking, your immune system will be impaired, which in turn makes you more susceptible to infections of all kinds, including COVID-19. As explained in our paper, having sufficient vitamin D in your system can reduce your risk of COVID-19 and other respiratory infections through several different mechanisms, including but not limited to the following:11
Reducing the survival of viruses
Inhibiting the replication of viruses12
Reducing inflammatory cytokine production
Maintaining endothelial integrity (endothelial dysfunction contributes to vascular inflammation and impaired blood clotting, two hallmarks of severe COVID-19)
Increasing angiotensin-converting enzyme 2 (ACE2) concentrations — Angiotensin II is a natural peptide hormone that increases blood pressure by stimulating aldosterone. ACE2 normally consumes angiotensin I, thereby lowering the concentration of angiotensin II. However, SARS-CoV-2 infection downregulates ACE2, resulting in excessive accumulation of angiotensin II, which worsens the infection
Boosting your overall immune function by modulating your innate and adaptive immune responses
Reducing respiratory distress13
Improving overall lung function
Helping produce surfactants in your lungs that aid in fluid clearance14
Boosting T cell immunity, which plays an important role in your body’s defense against viral and bacterial infections. When vitamin D signaling is impaired, it significantly impacts the quantity, quality, breadth and location of CD8 T cell immunity, resulting in more severe viral and bacterial infections.15
According to a December 11, 2020, paper,16 high-quality T cell response actually appears to be far more important than antibodies when it comes to providing protective immunity against SARS-CoV-2 specifically
Increasing expression of antimicrobial peptides in your monocytes and neutrophils — both of which play important roles in COVID-19
Enhancing expression of an antimicrobial peptide called human cathelicidin, which helps defend respiratory tract pathogens
From my perspective, vitamin D optimization is one of the easiest, least expensive and most impactful strategies to reduce your risk of serious SARS-CoV-2 infection and other respiratory infections.
Vitamin D optimization is particularly important for dark-skinned individuals (who tend to have lower levels than Caucasians unless they spend extended time in the sun), the elderly, and those with preexisting chronic health conditions. All of these are also risk factors for COVID-19, so population-wide optimization of vitamin D levels could significantly improve COVID outcomes among the most vulnerable.
How Vitamin D Influences Your COVID Risks
At this point, there’s no shortage of studies showing higher vitamin D levels beneficially impact all stages of COVID-19. It:
Lowers your risk of testing positive for COVID — The largest observational study17 to date, which looked at data for 191,779 American patients, found that of those with a vitamin D level below 20 ng/ml (deficiency), 12.5% tested positive for SARS-CoV-2, compared to just 5.9% of those who had an optimal vitamin D level of 55 ng/ml or higher. This inverse relationship persisted across latitudes, races/ethnicities, sexes and age ranges.
Reduces your risk of symptomatic illness — SARS-CoV-2-specific investigations have found that COVID-19 is far more common in vitamin D deficient individuals.
In one such study,18,19,20 82.2% of COVID-19 patients tested were deficient in vitamin D, compared to 47.2% of population-based controls. (Mean vitamin D levels were 13.8 ± 7.2 ng/ml, compared to 20.9 ± 7.4 ng/ml in controls.)
They also found that blood levels of vitamin D were inversely correlated to D-dimer levels (a measure of blood coagulation). Many COVID-19 patients have elevated D-dimer levels, which are associated with blood clots. This was particularly true with the original SARS-CoV-2 virus, but while less common with subsequent variants, some blood clotting, just less intense, can still occur.
Reduces infection severity — Our vitamin D paper21 also lists data from 14 observational studies that show vitamin D blood levels are inversely correlated with the incidence and/or severity of COVID-19. This is quite logical, considering vitamin D regulates inflammatory cytokine production — a lethal hallmark of COVID-19 — and is an important regulator of your immune system.
Reduces your risk of hospitalization — Reduced severity would translate into a lower risk for hospitalization, and that’s precisely what researchers have found.
A Spanish study22,23 found baseline vitamin D levels inversely correlated with the risk of ICU admission, and that giving supplemental vitamin D3 (calcifediol at 532 micrograms on the first day of admission followed by 266 mcg on days 3, 7, 15 and 30) to hospitalized patients with PCR-confirmed COVID-19 reduced ICU admissions by 82%.
Reduces your risk of death — COVID-19 patients with a vitamin D level between 21 ng/mL (50 nmol/L) and 29 ng/mL (75 nmol/L) had a 12.55 times higher risk of death than those with a level above 30 ng/mL in one study.24 Having a level below 20 ng/mL was associated with a 19.12 times higher risk of death.
Another study25,26 found the risk of severe COVID-19 and related deaths virtually disappeared when vitamin D levels were above 30 ng/mL (75 nmol/L).
A third paper27 found a marked variation in mortality depending on whether the patients lived above or below 35 degrees North latitude. As noted by the authors, having adequate vitamin D “could be very important in preventing the cytokine storm and subsequent acute respiratory distress syndrome that is commonly the cause of mortality.”28
Speeds viral clearance — While having enough vitamin D in your system will reduce your odds of infection and serious illness, taking oral vitamin D once infected can still help you recover faster.
Research29 published in November 2020 found oral vitamin D supplementation in SARS-CoV-2-positive individuals with mild symptoms who also had low vitamin D, helped speed up viral clearance.
Participants were randomly assigned to receive either 60,000 IUs of oral cholecalciferol (nano-liquid droplets) or a placebo for seven days. The target blood level was 50 ng/mL. Anyone who had not achieved a blood level of 50 ng/mL after the first seven days continued to receive the supplement until they reached the target level.
Periodically, all participants were tested for SARS-CoV-2 as well as fibrinogen, D-dimer, procalcitonin and CRP, all of which are inflammatory markers. The primary outcome measure of the study was the proportion of patients testing negative for COVID-19 before Day 21 of the study, as well as changes in inflammatory markers.
Of the 16 patients in the intervention group, 10 (62.5%) tested negative by Day 21, compared to just five of the 24 controls (20.8%). Fibrinogen levels were also significantly decreased in the treatment group, indicating lower levels of clotting.
How to Optimize Your Vitamin D Level
For optimal health, immune function and disease prevention, you want a vitamin D blood level between 60 ng/mL and 80 ng/mL year-round. In Europe, the measurements you’re looking for are 150 nmol/L and 200 nmol/L.
If you live in a sunny locale like Florida and practice sensible sun exposure year-round, you might not need any supplements. The DMinder app30 is a helpful tool to see how much vitamin D your body can make depending on your location and other individual factors.
Many, unfortunately, don’t get enough sun exposure for one reason or another, and in these cases, an oral vitamin D supplement may be required. Just remember that the most important factor here is your blood level, not the dose, so before you start, get tested so you know your baseline.
Here’s a summary of how to determine whether you might need an oral supplement, and your ideal dosage:
1. First, measure your vitamin D level — One of the easiest and most cost-effective ways of measuring your vitamin D level is to participate in the GrassrootsHealth’s personalized nutrition project, which includes a vitamin D testing kit. Once you know what your blood level is, you can assess the dose needed to maintain or improve your level.
2. Assess your individualized vitamin D dosage — To do that, you can either use the chart below, or use GrassrootsHealth’s Vitamin D*calculator. (To convert ng/mL into the European measurement (nmol/L), simply multiply the ng/mL measurement by 2.5.) To calculate how much vitamin D you may be getting from regular sun exposure in addition to your supplemental intake, use the DMinder app.31
Factors that can influence your vitamin D absorption include your magnesium32 and vitamin K233 intake. Magnesium is required for the conversion of vitamin D into its active form.34,35,36,37 If your magnesium level is insufficient, the vitamin D you ingest orally may simply get stored in its inactive form.38,39
Research by GrassrootsHealth40 shows you need 146% more vitamin D to achieve a blood level of 40 ng/ml (100 nmol/L) if you do not take supplemental magnesium, compared to taking your vitamin D with at least 400 mg of magnesium per day.
Your best bet is to take your vitamin D with both magnesium and K2. According to GrassrootsHealth,41 “combined intake of both supplemental magnesium and vitamin K2 has a greater effect on vitamin D levels than either individually,” and “those taking both supplemental magnesium and vitamin K2 have a higher vitamin D level for any given vitamin D intake amount than those taking either supplemental magnesium or vitamin K2 or neither.”
Data42 from nearly 3,000 individuals revealed 244% more oral vitamin D was required to get 50% of the population to achieve a vitamin D level of 40 ng/ml (100 nmol/L) if they weren’t concurrently also taking magnesium and vitamin K2.
3. Retest in three to six months — Remeasure your vitamin D level in three to six months, to evaluate how your sun exposure and/or supplement dose is working for you.
4. Take activated vitamin D (calcitriol) if your level is low and you come down with an acute infection like COVID. The dose is 0.5 mcg on day one and then 0.25 mcg daily for seven days.
From the start of the COVID pandemic, doctors were told they could not use any treatment that had not undergone randomized controlled trials. Most all clinical successes have been ignored and vehemently opposed
The Frontline COVID-19 Critical Care Alliance (FLCCC) was among the first to publish COVID treatment guidance. They have since developed protocols for prevention, early at-home treatment, in-hospital treatment and maintenance guidance for long-haul COVID syndrome that are updated as more becomes known
Corticosteroids can be an effective tool for reducing inflammation in general, but they appear particularly important for advanced COVID infection. Steroids should not be used early on, but can be lifesaving after you develop signs of lung dysfunction and increased oxygen requirement
Ivermectin has antiviral and anti-inflammatory properties and is beneficial in all stages of COVID-19, from prevention to advanced illness
Other effective protocols include the AAPS protocol, Tess Laurie’s World Council for Health protocol and the America’s Frontline Doctors’ protocol
Dr. Pierre Kory is one of the leaders in the movement to provide early treatment for COVID infection. Kory is a critical care physician (ICU specialist), triple board certified in internal medicine, critical care and pulmonary medicine, and is part of the Frontline COVID-19 Critical Care Alliance (FLCCC), which was among the first to publish COVID treatment guidance.
Kory spent most of his career at the Beth Israel Medical Center in Manhattan, New York, where he helped run the intensive care unit. He also had a busy outpatient practice. About six years ago, he was recruited to the St. Luke’s Aurora Medical Center in Milwaukee, Wisconsin, where he led the critical care service. “When COVID hit, I was in a leadership position,” he says. “I resigned, because of the way they were handling the pandemic.”
Treatment Options Have Been Vehemently Opposed
St. Luke’s, like most hospitals across the U.S., insisted on providing supportive care only, and Kory refused to remain in a leadership position under those circumstances. Patients were, for the first time in modern medical history, told to just suffer at home until they were near death, then go to the hospital where they were placed on deadly ventilator treatment.
“I knew there was a variety of treatments that we could use [yet] we were using nothing,” he says. Doctors were even told to not use anticoagulants, even though blood clotting was “through the roof” in many patients. “You could draw blood and actually see the blood clotting very quickly in the tubes,” he says.
Since those early days, the disease seems to have changed considerably. We don’t see the high rates of blood clotting anymore, for example, which is good news.
But for some reason, from the very start, “they were literally telling us that we needed randomized controlled trials to do anything,” Kory says, and to this day, health authorities are refusing to acknowledge any treatment protocol outside of the incredibly dangerous experimental drug remdesivir, and the experimental COVID jabs.
“People were dying, [yet] all of my ideas were getting shouted down. My superiors were showing up [to my clinical meetings] and getting me to stand down, because I was entertaining the idea that we should do this, that and the other thing, and they didn’t want anything to be done.
And so, I said, ‘I’m done.’ I resigned mid-April 2020. I then went to New York for five weeks and ran my old ICU in New York.”
The Importance of Steroids in the Treatment of COVID-19
In May 2020, Kory testified before the U.S. Senate, stressing how critical it was to use steroids during the hospital phase of this infection. At that time, he was still employed by the University of Wisconsin. His resignation date had not yet happened, and they “were livid that I was speaking in public, giving my opinion.”
This is remarkable, because when you’re an expert in a field, “you’re actually responsible to share your insight and expertise,” Kory says. “Yet they were very unhappy that I was doing that.”
Seven weeks later, Kory was vindicated when the British Recovery trial results came out, showing the benefits of corticosteroids. Since then, steroids have become part of standard of care in the hospital phase.
Steroids are an effective tool for reducing inflammation in general, but they appear particularly important for advanced COVID infection. I had a close friend who contracted a very serious case of COVID-19 and kept worsening despite taking everything I suggested.
He knew Dr. Peter McCullough, so he texted him and was told to add prednisone and aspirin to his current regimen. As soon as he took the prednisone, he started getting better.
As explained by Kory, this is a common experience. Importantly, the evidence shows that when used early, during mild infection, corticosteroids do more harm than good. But once you are entering into moderate illness, as soon as you start to see lung dysfunction or the need for oxygen, steroids are critical and are clearly lifesaving.
Steroids Must Be Used at the Correct Time
One of the reasons for this is because SARS-CoV-2 infection triggers a very complex cascade of inflammation. More specifically, Kory says, severe COVID-19 is a macrophage activation syndrome. It’s the hyperinflammatory macrophages (a subtype of macrophages) that end up causing organ damage. So, you want to use medicines that either suppress their activity or repolarize them into hypoinflammatory macrophages.
The key is to use the steroids at the correct time — not too early and not too late, the “Goldilocks” window. There are no hard and fast rules for that, as each patient is different, but as a rule of thumb, do NOT use it until or unless you are seeing a significant worsening of symptoms to where breathing is getting more difficult.
Kory’s outpatient protocol includes prednisone on Day 7, 8 or 9, if you’re still going downhill. It is important to NOT use it early in the course of the illness as it will actually worsen the infection by increasing viral replication.
The suggested dosage is 1 milligram of prednisone or methylprednisolone per kilogram of bodyweight. When using methylprednisolone (Medrol) (which Kory prefers, in part because lung tissue concentrations are higher than prednisone), he divides it into two daily doses. Kory does not recommend the use of dexamethasone, as it doesn’t work as well for lung disease. Yet, most doctors in the U.S. use dexamethasone if they’re using steroids at all.
The dose may be increased depending on the severity and trajectory of the infection. “I probably will either double or triple the [dose] until I can get them stable,” he says.
“Once they’re off oxygen, then I taper off [the steroid] over about a week to 10 days, sometimes shorter. Depends how long they were on oxygen. If they were on it for a short time, I do a fast taper; if they were on oxygen for a longer time, I’ll do a slower taper. But I don’t start fully tapering until they’re off oxygen.”
Anticoagulants — When to Use Them
As mentioned earlier, while early COVID-19 cases often involved severe blood clotting, that feature of the infection appears to have receded. Even when clotting occurs, it’s typically much milder than what we saw in the beginning. Still, anticoagulants can be an important component in these cases.
“What I do with coagulation is, I generally follow the D dimer on admission. D dimer is a marker of endothelial injury and clotting. In patients with normal D dimers, I’ll just do routine prophylaxis doses. If it’s moderately elevated, I do moderate [doses] and if it’s severely elevated, I’ll do full dose anticoagulants,” Kory explains.
He typically uses an anticoagulant called Lovenox. Patients are also given full-dose aspirin, unless there’s a contraindication. I suspect fibrolytic enzymes like lumbrokinase and nattokinase, which help degrade fibrin, may be a better alternative to aspirin. N-acetyl cysteine (NAC) is another potential candidate. Kory is not convinced, however:
“We have used NAC in different disease models over the years. It’s a standard treatment for acetaminophen overdose, but not for pulmonary fibrosis. In pulmonary medicine, of which I’m an expert, we had decades where we studied NAC for that. None of those studies panned out. In sepsis, it didn’t really pan out.
And so, for severe disease, we think it’s an effective drug and it’s a good antioxidant. I think it does have anticoagulation [effects], but our opinion is that it’s generally weak. So, for the hospital phase, we think it’s too weak.”
Vitamin C
Another important component is intravenous vitamin C. While some university hospitals may carry IV vitamin C, most don’t but might be able to get it from another local hospital. Importantly, the vitamin C needs to be administered within the first six hours of admittance to the ICU in order to work, and it may be similar for COVID.
This is especially true for the relatively low doses recommended by the Math+ protocol of 1,500 mg or 1.5 grams. Many outpatient natural medicine physicians will use 25 grams to 50 grams of IV vitamin C, but most hospitals will not allow this high a dose, even though it is likely that higher doses will work if you missed the early treatment window (the first six hours). So pragmatic logistics is why the Math+ protocol uses relatively low doses.
One suggestion would be to call the hospital you’re thinking of using if you ever had to be admitted for COVID and ask if they have it. If not, you can ask your doctor to order it for you and bring it to the hospital, if you or a family member are admitted for COVID or sepsis. The key, of course, is having a doctor who is willing to use it. Some aren’t.
“You should’ve seen the resistance I got. At one point, I was the director of the main ICU at the University of Wisconsin and the data was so overwhelming, I said, ‘Hey, guys, can’t we just start a protocol where we just give everybody on admission IV vitamin C? What’s the downside?’
Everyone started talking about kidney stones and all of this nonsense, and we have so much data to show that doesn’t happen in acute illness, or in IV formulations … I feel like I live in a cartoon of medicine, because every time I discuss something with someone, they just don’t believe anything works. Because if it worked, they would be doing it. It’s bizarre.”
The FLCC Protocol
Sadly, the willful ignorance of many doctors is literally killing many COVID patients who could have, and should have, been saved. There’s just no doubt that protocols such as the one developed by the FLCC and the other groups listed below could have saved many, had it been widely implemented. Yet despite its success, many hospitals to this day do not use it.
“Our protocol is always evolving,” he notes. “We’re not saying that this is the only way to treat it. This is how we decided to treat it. We reserve the right to deprioritize or change the dose, or substitute a new medicine.
We want to follow the data, the experience and the knowledge of this disease. That’s No. 1. No. 2, all of our protocols are combination therapy protocols.
And by the way, that gives doctors fits. You know why? Because they want to know, how do you know that this is necessary? There are trials of each individual component showing that they’re effective. We believe they’re synergistic, but we’re never going to do a trial to test every component on our protocols.
But there are a number of other protocols. The AAPS has a protocol.1 The World Council for Health,2 they have a number of options. So there are many doctors who might emphasize or de-emphasize a medicine on our protocol. And we do not pretend that ours is the only way. But we do put a lot of thought into it.
Most of our medicines are repurposed, so they’re not novel. They’re very well-known over decades, their safety profiles are well known, they tend to be generally low cost, and their mechanisms are well-known. A central medicine to all of our protocols — prevention, early treatment, hospital, and late phase like long-haul [syndrome] is ivermectin, for many reasons.”
Why Ivermectin?
As noted by Kory, ivermectin is a potent antiviral. “That’s been demonstrated for 10 years now in the lab on a number of viruses,” he says. “They’ve shown that it interrupts replication of Zika, Dengue, West Nile, even HIV. And then the clinical studies are just overwhelming.” He continues:
“Can I just take one minute to say that if anyone wants to call ivermectin a controversial medicine, I just want to call out it is absolutely not controversial.
It is a medicine that is buried in corruption, and the corruption is in the suppressing of its efficacy. There are immense powers that do not want the efficacy of that drug to be known because, if it is known and becomes standard of care, it will obliterate the market for a number of novel pharmaceutical products.
When you look at the actions taken against ivermectin, it can only be understood that it’s threatening something big and powerful, because boy has it been attacked [even though it’s been used in] 64 controlled trials, almost every single one of them showing benefit, many of them large benefits.
Yet they distort it to make it seem like it’s controversial. It’s absurd. We know it works. We know it from in vitro, in vivo animal studies, and case series.”
One of the first case series, from the Dominican Republic, was published in June 2020. They treated 3,300 consecutive emergency room COVID patients with ivermectin. Of those, only 16 went on to be hospitalized and one died. That’s pretty profound, considering these were severely ill individuals.
Importantly though, there is a dose-response relationship to the viral load. The Delta variant has been shown to produce viral loads that are 250 times higher than Alpha, and as Delta became predominant, breakthrough cases in the prevention protocol started happening.
“I’m one of them. I got COVID while I was taking it weekly,” Kory says. “Now we’re doing it twice weekly. Is it the right dose? We’re not sure. But we’re seeing much fewer breakthroughs now on a higher dose. Could it be higher? Maybe. But, but we know it works as prevention.”
Higher doses of ivermectin are also used for treatment of Delta. In more advanced stages, the drug is useful thanks to its anti-inflammatory properties. Contrary to many other drugs, ivermectin is beneficial in all stages of the infection.
Vitamin D Optimization Is Crucial
Other components of the FLCC’s prevention and treatment protocols include products that have either antiviral or anti-inflammatory properties, or a combination thereof, such as melatonin, quercetin and zinc, and anticoagulants such as aspirin.
Ideally, everyone would optimize their vitamin D level before ever needing treatment for COVID. If you haven’t done so already, check your vitamin D blood level and if it’s below 40 ng/mL, start taking an oral supplement. Don’t wait until you’re sick. The medical literature suggests population-wide vitamin D optimization, to a level above 40 ng/mL, could have reduced COVID morbidity and mortality by about 80%.
“No question,” Kory says. “In fact … there was a study that came out, a huge database of patients, where they looked at patients who tested their vitamin D levels before they got ill. They estimated — and they did no fancy statistical modeling logistic regression — that at 50 ng/mL, there was zero mortality.
The federal government knows that vitamin D deficiency … is ubiquitous in nursing homes [and minorities] … So, that we didn’t have a vitamin D protocol nationally is criminal. Literally, it’s criminal.”
In the hospital treatment protocol, the FLCCC recommends using calcitriol, 0.5 micrograms on Day 1 and 0.25 mcg daily thereafter for six days. Calcitriol is the active form of vitamin D typically produced in your kidneys.
This is because merely taking regular oral vitamin D fails in acute conditions as it takes weeks to be metabolized to its active form. Calcitriol is the active form, so it will start to work immediately. One can also take the vitamin D, though, as eventually adequate blood levels will be reached and the calcitriol can be discontinued.
Why Men Do Worse than Women in COVID
As mentioned earlier, the protocol also includes a number of nutraceuticals, such as quercetin and zinc. Another drug that looks promising is fluvoxamine, an antidepressant. Kory says:
“The studies continue to pan out, and even clinically, some of my colleagues who incorporated ivermectin with fluvoxamine saw much less treatment failures. I rank it as highly effective, but it doesn’t cure everybody. They saw an occasional treatment fail and they said it really disappeared once they use the combo.
For someone older or with more advanced disease, more comorbidities, obese patients, diabetics, I tend to throw the kitchen sink at those folks. I try to use as many elements in the protocol as I can. So there, I’ll add fluvoxamine.
The game changer now is antiandrogens. We use spironolactone, which is a potassium-sparing diuretic, at doses above 100 mg a day. It has potent antiandrogen properties, as well as dutasteride, a 5-alpha reductase inhibitor, which also suppresses testosterone.
Androgens seem to be a huge potential driver of this illness, not only in terms of driving viral replication, but also in potentially aiding inflammation … The trials on that are really, really potent … so, we have an antiandrogen aspect. I’ve been using that on some of my older or more advanced disease patients. I’ll add that on pretty quick.”
Home Treatment Recommendations for COVID
While it can be difficult to find a doctor who is willing to actually treat COVID-19 with the FLCCC protocol (or any other for that matter), many of those who are willing are making full use of telemedicine.
This is a load of information to review, especially if you are fatigued and sick with COVID or have a family member struggling. So, I reviewed all the protocols and believe the FLCCC one is the easiest and most effective to follow. I’ve posted it below.
However, I’ve altered some of the dosages, and added a few more therapies that they have yet to include, such as:
Nebulize hydrogen peroxide 5 ml of 0.1% peroxide dissolved in 0.9% normal saline every hour or two. It’s best to use nebulizer that plugs into the wall, as these are more effective than battery operated ones.
Intravenous ozone administered by a trained ozone physician.
NAC 500 mg twice a day.
Make sure the honey is raw honey, not normal honey from the grocery store. Raw honey can be obtained online or at a health food store.
Fibrinolytic enzymes like lumbrokinase, serrapeptidase or nattokinase, two to four tablets, two to three times a day, on an empty stomach (one hour before or two hours after a meal). This will help break down any microclots.
Decrease zinc dose from 100 mg to 50 mg elemental zinc, but only for three days, then decrease to 15 mg elemental zinc.
Increased quercetin from 250 mg to 500 mg.
Change vitamin C to liposomal C 1,000 to 2,000 mg four to six times per day.
CoQ10 is the third-most consumed supplement, after sh oil and multivitaminsCoQ10 keeps your mitochondria healthy and plays a crucial role in the production of ATP, the cellular energy required to keep you alive CoQ10 deciencies have been linked to many health problems, including migraines, heart disease and cancer Conversely, supplementing with CoQ10, or the natural form called ubiquinol, may help improve several chronic health conditions such as AFib, NAFLD and heart failure.
While 89% of people aged 65 and older take at least one prescription medication, 54% take four or more
A commentary by Dr. Mark E. Williams detailed the case of “Allison,” who was taking 43 different medications and suffering multiple side effects as a result
Polypharmacy is a preventable risk factor for hospital admission in older adults, due to adverse drug events
The risks of polypharmacy include mortality, falls, adverse drug reactions, increased length of hospital stay and hospital readmission
A holistic approach, one that addresses the key tenets of good health and creates real wellness instead of attempting to cover up symptoms with more pills, is needed to achieve optimal health
Polypharmacy, or the use of multiple medications, is common in older adults. While 89% of people aged 65 and older take at least one prescription medication, 54% take four or more.1 Data from Merck similarly found that nearly 80% of older adults regularly take at least two prescription drugs while 36% regularly use five or more different drugs — and this doesn’t include over-the-counter medications.2
Adverse effects from polypharmacy are common and may drive patients to seek out ever-more drugs to treat the side effects caused by their unsafe drug regimen. It’s a vicious cycle, one that’s perpetuated by a broken health care system that revolves around pharmaceutical-driven, fragmented care.
Not only do many patients see multiple doctors, each of whom may prescribe their own set of medications, but patients may pressure doctors to prescribe drugs they’ve seen on direct-to-consumer advertisements. Instead of looking at the big picture of how to get healthy, tending to essential factors like diet, stress and physical activity, “health care” for seniors often turns into “drug care,” with potentially disastrous results.
One Patient — 43 Prescription Drugs
A commentary by Dr. Mark E. Williams published on Medscape highlights just how extreme polypharmacy can become. In some cases, it’s not “just” four or five medications but dozens of them, and in the case of Williams’ patient “Allison,” it was 43. The woman had been transferred to a chronic care facility for long-term care due to bipolar illness.
Days earlier, she was treated at a hospital for mental health issues, which Williams said “was probably related to inappropriate polypharmacy.”3
“Despite being admitted to the hospital for adverse drug reactions related to polypharmacy, Allison was discharged to my facility on 43 prescription medications and an almost equal number of over-the-counter (OTC) drugs. It took more than 10 minutes for the nurse to review the admission medications with me over the phone,” he wrote.4
Allison’s symptoms included fatigue, dizziness, muscle aches, headache, nausea, insomnia and more, and she requested additional medications to treat them. Not only was the woman taking duplicate medications meant to treat the same symptoms, but she was also taking medications intended to treat common adverse effects.
“The ‘chemical soup’ in her body is leading to mental and physical problems,” Williams told the patient’s daughter, but she, too, bought into the notion that more drugs equaled better care. After overcoming the patient’s resistance to going off the drugs, over a three-month period Williams was able to reduce Allison’s medications to about 15 — still a staggering number, but less so than 43.
“Allison improved, both mentally and physically,” Williams wrote,5 but challenges still ensued, including the patient demanding a memory drug she had seen advertised on television, and an incident in which her daughter gave her an over-the-counter sleep aid, leading to lethargy, confusion and slurred speech.
Ultimately, Allison was transferred to another facility, where the dangerous polypharmacy undoubtedly continued. While Williams’ commentary highlights an extreme case, it’s not unique — polypharmacy is prevalent among seniors.
Polypharmacy Worsens Health
When medications are prescribed in excess, including to treat the side effects of other drugs, the patient’s health suffers. “The use of numerous medications may result in medication-related problems such as inappropriate indications, therapeutic duplication, adverse effects, drug interactions, unnecessary medications, poor adherence and a strain on health care resources,” according to a featured article in The Journal for Nurse Practitioners.6
It also noted that polypharmacy is a preventable risk factor for hospital admission in older adults, due to adverse drug events. The risks of polypharmacy, meanwhile, are well noted. In BMC Geriatrics, adverse outcomes including mortality, falls, adverse drug reactions, increased length of hospital stay and hospital readmission are listed, and the risk of harm increases with the number of medications.7 According to the systematic review:8
“Harm can result due to a multitude of factors including drug-drug interactions and drug-disease interactions. Older patients are at even greater risk of adverse effects due to decreased renal and hepatic function, lower lean body mass, reduced hearing, vision, cognition and mobility.”
In 2007, Dr. Michael Stern, geriatric emergency medicine specialist at New York Presbyterian Hospital, even told a New York Times reporter that polypharmacy accounts for more than one-fourth of all admissions to the hospital and that it would be considered the fifth leading cause of death if it were categorized that way.9
Older People Are More Vulnerable to Drug Side Effects
The fact that older people are more likely to be taking more prescription drugs is a double-edged sword, as the elderly are already at increased risk of drug side effects. In fact, the elderly are estimated to be twice as susceptible to adverse drug events compared to younger people.
“Side effects are also likely to be more severe, affecting quality of life and resulting in visits to the doctor and in hospitalization,” according to the Merck Manual, which also explains several reasons why older people are so vulnerable to drug side effects:10
Older people have less water and more fat tissue in the body; this allows higher concentrations of drugs that dissolve in water and increased accumulation of drugs that dissolve in fat
The kidneys are less effective at excreting drugs into urine
The liver is less able to metabolize drugs, so they’re not removed as readily from the body
“Older people are more likely to have chronic medical disorders that may be worsened by drugs or that may affect how the drugs work”
Some common examples of how drugs may affect seniors differently include blood pressure drugs, which may lead to more dramatic drops in older people, leading to symptoms of dizziness and falls. Older adults may also become confused and sleepy when using antianxiety drugs, more so than typically seen in younger people. Such effects may only be compounded when multiple drugs are being taken at the same time.
In fact, due to changes that occur during biological aging, it’s now recognized that medications should be clinically tested specifically with older adults in mind. However, older adults are often excluded from clinical trials, which means the safety and efficacy of drugs in this population is often unknown, with supportive evidence lacking.
“Inevitably, this lack of evidence has often led to inappropriate drug treatment and, consequently, to various adverse clinical outcomes,” according to a review published in March 2021 in European Geriatric Medicine.11
Why Are so Many More Seniors Taking Antidepressants?
Overprescribing is rampant among the senior population, and antidepressants are one such example. There’s been a major rise in the number of antidepressants being prescribed for older adults over the last two decades, without a similarly sharp increase in the number depressed, according to a study published in The British Journal of Psychiatry.12
The findings suggest seniors may be being overprescribed antidepressant drugs, which could have serious implications for their health, although the researchers weren’t willing to state this, noting instead, “we can’t infer that older patients are prescribed antidepressants unnecessarily.”13
In the first study group, 4.2% of the adults were taking antidepressants, but this jumped to 10.7% in the later study. During this time, the prevalence of depression decreased, but only slightly, from 7.9% to 6.8%.14 Also noteworthy, among older adults living in care homes, the prevalence of depression was unchanged but the use of antidepressants rose from 7.4% to 29.2%.15
There were a few suggestions offered for why antidepressant prescribing rates increased so steeply without a similar increase in depression, including overdiagnosis or prescribing the drugs for conditions other than depression. However, most of those prescribed antidepressants had not been diagnosed with depression.
Further, antidepressants carry a risk of side effects that could easily spiral into more drug prescriptions. For instance, antidepressant users have an increased risk of developing Type 2 diabetes,16 and antidepressant use has been linked to thicker arteries, which could contribute to the risk of heart disease and stroke.17
Nearly Half of Over 75s Take Statins
Statin cholesterol-lowering drugs are another example of a wildly overprescribed drug class that’s contributing to polypharmacy risks. In the U.S., close to 50% of U.S. adults over 75 years take a statin,18 even though their use may also harm brain health — more than doubling risk of dementia in some cases.19
A connection also exists between statins and diabetes, to the extent that people who take statins are more than twice as likely to be diagnosed with diabetes than those who do not, and those who take the drugs for longer than two years have more than triple the risk.20,21 With a diabetes diagnosis, of course, comes more drugs.
Often, statins are unnecessary in the first place. While they are effective at lowering cholesterol, whether this is the panacea for helping avoid heart disease and extend lifespan is a topic of heated debate. In 2018, a scientific review presented substantial evidence that high LDL and total cholesterol are not an indication of heart disease risk, and that statin treatment is of doubtful benefit as a form of primary prevention for this reason.22
Drugs Don’t Equate to Good Health
Overprescribing pills is setting up seniors for a downward spiral of increasing side effects and worsening health. A holistic approach is needed, one that addresses the key tenets of good health and creates real wellness instead of attempting to cover up symptoms with more pills.
As just one example, in a study of older depressed adults, 80% experienced a significant reduction in depressive symptoms after taking up strength training for 10 weeks, such that researchers concluded that the exercise was “an effective antidepressant in depressed elders, while also improving strength, morale and quality of life.”23
It’s important to work with a health care provider who understands the risks of polypharmacy and the fact that good health doesn’t come from a pill. Only by building a health plan that addresses diet, exercise, sleep, emotional wellness and toxic exposures, along with only targeted and truly necessary medications and/or supplements, can you reach optimal health.
A September 2020 meta-analysis concludes there is a significant relationship between autism and concentrations of lead and mercury in the body
According to the researchers, mercury concentration is a pathogenic cause for autism, meaning it’s a causative factor
According to a 2014 review, there is evidence of malfeasance and conflicts of interest in studies claiming that thimerosal in vaccines is safe
Serious flaws and errors also plague studies that claim aluminum in vaccines is safe. A mathematical error found in a key FDA study has reignited concerns about the safety of aluminum in vaccines
Glutathione is the dominant agent that binds to and helps move mercury and other heavy metals out of your tissues. Part of effective detox involves upregulating your biochemistry to facilitate the mobilization and elimination of metals
This article was previously published October 13, 2020, and has been updated with new information.
The controversy over whether mercury overexposure can trigger autism is a long-standing one. A new meta-analysis of previous studies sheds much needed light on the matter, concluding there’s a “significant relationship” between the two.
The review,1,2 published in the September 2020 issue of Pediatric Health, Medicine and Therapeutics, looked at 18 studies conducted between 1982 and 2019 that examined the relationship between concentrations of copper, lead or mercury in blood, plasma, hair or nails and the prevalence of autism. While no relationship was found between autism and copper concentrations, a high degree of correlation was found for mercury and lead.
According to the authors,3 the relationship between mercury and autism is so strong that “the concentration of mercury can be listed as a pathogenic cause (disease-causing) for autism.” This held true even when outlier studies that might unduly influence the results were removed.
Mercury Is a Causative Factor
In the introduction, the authors point out that studies carried out in this area suggest mercury and other toxins are involved in the cause of autism, which include abnormal brain development that affects social interaction and communication skills.
“Metals’ biological effects are associated with their chemical properties, suggesting that excessive metal exposure can cause brain abnormalities around the world,” the researchers state.4
“Mercury is considered as a risk factor for autism since, according to previous studies, it has been recognized as a neurotrophic toxin. Reduction in mercury content in hair and teeth of the children with autism aroused the low disposal of mercury hypothesis.
Blaurock-Bush et al found that heavy metals are effective in the development of autism disorder. The role of mercury in the pathogenesis of autism has also been proven in other studies …
According to points raised in the present study … it would be quite reasonable to advise prevention of exposure to mercury and lead in children and provision of suitable conditions during the sensitive period of mothers’ pregnancy as vital measures to prevent the disease …”
A 2017 review paper,5 “The Toxicology of Mercury: Current Research and Emerging Trends,” details the “kinetics of this metal,” including “its metabolism, interaction with other metals, distribution, internal doses and targets and reservoir organs.” The paper cites several studies linking mercury and autism among its references, noting that:6
“Autism spectrum disorder (ASD) has been demonstrated to be accompanied by distorted metal homeostasis. The degree to which people are affected by the metals seems to be largely influenced by the individual genetic makeup.
Especially Hg [mercury] exposure has become a suspected causative factor for many pathological conditions, and several sources of exposure to Hg compounds can be listed, including dental amalgam fillings, seafood, vaccines and increasingly from energy saving light bulbs as well.”
Malfeasance in Research Showing Thimerosal Safety
In the video above, the University of Calgary faculty of medicine illustrates how mercury causes neuronal degeneration in your brain. While there are many environmental sources of mercury exposure, some of the most prominent ones include high-mercury fish, dental amalgam and thimerosal-containing vaccines.
Thimerosal is a mercury-based preservative used in certain vaccines. While it has been removed from most childhood vaccines, it is still used in some multidose vials, meaning vials that contain more than a single dose of the vaccine.
Remarkably, while the fact that mercury is neurotoxic is noncontroversial, health authorities still insist injected thimerosal is perfectly safe and has never been linked to neurological dysfunction. How could that be?
In 2014, a review article7 in the BioMed Research International journal titled, “Methodological Issues and Evidence of Malfeasance in Research Purporting to Show Thimerosal in Vaccines Is Safe,” noted that:
“The studies upon which the CDC relies and over which it exerted some level of control report that there is no increased risk of autism from exposure to organic Hg in vaccines, and some of these studies even reported that exposure to Thimerosal appeared to decrease the risk of autism.
These six studies are in sharp contrast to research conducted by independent researchers over the past 75+ years that have consistently found Thimerosal to be harmful … Many studies conducted by independent investigators have found Thimerosal to be associated with neurodevelopmental disorders.
Several studies, for example, including three of the six studies covered in this review, have found Thimerosal to be a risk factor for tics. In addition, Thimerosal has been found to be a risk factor in speech delay, language delay, attention deficit disorder, and autism.
Considering that there are many studies conducted by independent researchers which show a relationship between Thimerosal and neurodevelopmental disorders, the results of the six studies examined in this review, particularly those showing the protective effects of Thimerosal, should bring into question the validity of the methodology used in the studies …
Importantly … five of the publications examined in this review were directly commissioned by the CDC, raising the possible issue of conflict of interests or research bias, since vaccine promotion is a central mission of the CDC.
Conceivably, if serious neurological disorders are found to be related to Thimerosal in vaccines, such findings could possibly be viewed as damaging to the vaccine program.”
Aluminum Is Another Neurotoxic Poison
Today, the most commonly used vaccine preservative is aluminum, not thimerosal. It’s unfortunate that the Pediatric Health, Medicine and Therapeutics review did not include it, because it’s likely that aluminum has a similar impact on autism as mercury.
According to a 2018 study,8 people with autism were found to have high amounts of aluminum in their brains.
“The mean (standard deviation) aluminium content across all 5 individuals for each lobe were 3.82(5.42), 2.30(2.00), 2.79(4.05) and 3.82(5.17) μg/g dry wt. for the occipital, frontal, temporal and parietal lobes respectively,” the researchers noted.9
The lead author on this paper was Dr. Christopher Exley, a leading expert in aluminum toxicology. He and a team of international scientists have also published a paper10 in the December 2020 issue of the Journal of Trace Elements in Medicine and Biology.
In it, they provide evidence for their position that “the safety of aluminium-based vaccine adjuvants … must be seriously evaluated without further delay, particularly at a time when the CDC is announcing a still increasing prevalence of autism spectrum disorders, of 1 child in 54 in the USA.”
As with thimerosal above, serious flaws and errors plague studies that claim aluminum in vaccines is safe, including a mathematical error found in a key U.S. Food and Drug Administration study has reignited concerns about its safety.
The FDA study,11 published in 2011, compared aluminum exposure from vaccines in infants to the Agency for Toxic Substances and Disease Registry’s (ATSDR) safety limit of oral aluminum, concluding that:12
“… the body burden of aluminum from vaccines and diet throughout an infant’s first year of life is significantly less than the corresponding safe body burden of aluminum modeled using the regulatory MRL.
We conclude that episodic exposures to vaccines that contain aluminum adjuvant continue to be extremely low risk to infants and that the benefits of using vaccines containing aluminum adjuvant outweigh any theoretical concerns.”
The problem, found by Physicians for Informed Consent, is that the FDA based its calculations on 0.78% of oral aluminum being absorbed into the bloodstream instead of the value of 0.1% used by the ATSDR.
“As a result,” Physicians for Informed Consent noted,13 “the FDA paper assumed that nearly 8 (0.78%/0.1%) times more aluminum can safely enter the bloodstream, and this led the authors to incorrectly conclude that aluminum exposure from vaccines was well below the safety limit.” Christopher Shaw, a professor at the University of British Columbia who has studied the effects of injected aluminum, explained in a news release:14
“We knew that the [2011] Mitkus et al. paper modeling aluminum clearance had to be inaccurate since it was assuming that injected aluminum kinetics were the same as the kinetics of aluminum acquired through diet.
Now, in addition, we see that they did their modeling based on using the incorrect level of aluminum absorption. What is particularly striking is that despite all these errors, since 2011, Mitkus et al. is used by CDC and other entities as the basis for claiming that aluminum adjuvants are safe.”
The Dangers of Lead
Lead is a naturally occurring metal that was once commonly used in gasoline, paint and children’s toys, and is still a part of batteries, pipes, pottery, roofing materials and cosmetics. Due to environmental pollution, food and water has also become a source of this dangerous toxin.
If you live in an urban area or near a busy road, it’s probably best to assume that your soil is contaminated with lead to some extent. This is also an issue if you plan to plant a vegetable garden, as vegetables can take up lead from the soil very efficiently.
Lead damages your brain and nervous system, and has been shown to lower IQ. Even small amounts can be dangerous, as lead builds up in your body over time. Children under 6 are especially at risk, as they absorb lead more easily than adults.
Herbert Needleman was a researcher who studied neurodevelopmental damage caused by lead poisoning,15 and he performed much of the foundational research showing even low levels of lead were dangerous. Another crucial crusader against lead was geochemist Clair Cameron Patterson, Ph.D.
It’s thanks to Patterson’s tireless work that lead was finally removed from gasoline, thereby saving untold billions of people from serious harm.16 He’s an unsung public health hero of the 20th century that most people have never heard of.
The video below is a short summary of the evolution of leaded gas, and ultimately, its removal, which was no small feat. Unfortunately, there are many other sources of toxic metals, and unless we address them all, we’re unlikely to get a handle on the autism epidemic.
We’re Getting Mercury Out of Dentistry
As mentioned, dental mercury is one pernicious source of mercury. Here, there is good news. After years of pressure from Consumers for Dental Choice and its allies, the FDA has finally released a long-overdue safety communication on dental amalgam.17 September 24, 2020, the FDA issued a warning that mercury fillings may adversely affect:
Pregnant women and their developing fetuses
Women who are planning to become pregnant
Nursing women and their newborns and infants
Children, especially those younger than 6
People with pre-existing neurological disease such as multiple sclerosis, Alzheimer’s disease or Parkinson’s disease
People with impaired kidney function
People with known heightened sensitivity (allergy) to mercury or other components of dental amalgam
While the FDA downplays the importance of its changed recommendation by stressing that the benefits of dental amalgam likely “outweigh their risks for most patients,” this update is nothing short of monumental, and opens the door, finally, for the elimination of dental mercury for all patients in the U.S., as has been done in many other countries already.
Detoxifying Heavy Metals
Heavy metal detoxification is no simple matter. Glutathione is the dominant agent that binds to and helps move mercury and other heavy metals out of your tissues. Part of effective detox involves upregulating your biochemistry to facilitate the mobilization and elimination of metals. In summary, the three pillars of heavy metal detox are:
Cleanse and clear your GI tract of metals and toxins
Optimize glutathione
Upregulate detox genes
One way to help improve your glutathione is by taking N-acetylcysteine (NAC), which is a precursor to and rate-limiting nutrient for the formation of glutathione. Glutathione is poorly absorbed so, in many cases, it’s easier to raise your glutathione by taking NAC instead.
In addition to upregulating your biochemistry to mobilize and eliminate heavy metals, sauna bathing can also go a long way toward eliminating mercury and other toxins from your body.
In January 2020, I interviewed Boyd Haley, Ph.D., a chemist specializing in the development of chemicals to chelate toxic metals. Haley has developed a nontoxic chelating compound called emeramide or NBMI (brand name Irminix), which tightly binds to mercury and free iron (which is also highly toxic), and acts as a potent antioxidant, as it has two glutathione arms.
Emeramid is still under drug development but can be obtained via expanded access, named patient use, compassionate use or special use, depending on the country you’re in. An early access application and prescription, required by the EMA, is available on the company’s website, EmeraMed.com.18
In closing, the evidence strongly suggests exposure to mercury, lead and aluminum are significant risk factors for autism and other neuropathologies. The simplest answer to the autism epidemic is therefore to prevent children from these kinds of exposures. That includes banning dental amalgam and getting thimerosal and aluminum out of all vaccines.
One study published in Nutrients found supplementing with vitamin D in patients with confirmed COVID-19 shortened the length of hospitalization, even in those with comorbidities
This data is part of mounting evidence that those with optimal levels of vitamin D may have a reduced risk of getting infected and, if infected, a lowered risk of severe disease and mortality
The only way to definitively identify a deficiency is through a blood test. Look for these general signs and symptoms that you need to get tested sooner rather than later. They include frequent infections, fatigue, daytime sleepiness and head sweating
Since the start of the pandemic, natural supplements have been a bone of contention with researchers, pharmaceutical companies, doctors and health experts. Newly published data1 again support past research that vitamin D has a significant impact on COVID-19.
Vitamin D was discovered in the early 1900s. Work by Sir Edward Mellanby from Great Britain and Elmer McCollum from the University of Wisconsin demonstrated that vitamin D could cure rickets.2 In the early 1970s, 25-OH-D3 was identified as scientists focused on the endocrine system, and the function that vitamin D has in the body.
Your body is capable of producing vitamin D with exposure to sunlight.3 In fact, with adequate exposure, your skin can produce enough vitamin D to support your health. Early research showed that too little vitamin D led to poor calcium homeostasis. In turn, this can lead to osteoporosis, osteomalacia and rickets.
Multiple studies4,5 have since demonstrated that a deficiency “is associated with increased risk and greater severity of infection, particularly of the respiratory tract.”6 While nearly every study finds a relationship between vitamin D and upper respiratory infections, not all find that vitamin D has the same impact on the infections.
One factor that may influence the varied results is how the researchers measure the intervention and data. In other words, are they measuring the amount of supplementation being given or are they looking at the vitamin D blood levels demonstrating deficiency against the impact on infection?7
Study Shows Vitamin D Shortens COVID and Decreases Mortality
A study8 published in November 2021 sought to identify if vitamin D may play a role in the treatment of COVID-19. The researchers noted that patients admitted to the intensive care unit had high plasma levels of biomarkers indicating inflammation. They wrote:9
“Given the natural three-stage clinical course of the disease, inadequate innate immune response in the first stage and immune-mediated damage due to dysregulated immune response in the second stage are considered to be the major determinants of poor outcomes.”
Should a supplement or drug be able to support the immune response in the first or second stage, it may help reduce the severity and mortality of the illness. The researchers first gathered retrospective data from 867 patients at the Istanbul University-Cerrahpasa Faculty Hospital.
The patients had a confirmed diagnosis of COVID-19 but were excluded from the cohort if they had comorbidities associated with vitamin D deficiency, such as cancer, kidney disease, cardiovascular disease or autoimmune diseases. Each of the patients received an antiviral and some received anti-cytokine treatment. Clinical outcomes were measured against serum vitamin D status.
In the retrospective arm of the study, the researchers split the participants into four groups determined by their serum 25OHD level. The data from this arm revealed that the risk of hospitalization longer than eight days was 1.9 times higher in patients in three of the groups.
The second part was designed as a prospective study involving 210 people with confirmed COVID-19. The researchers included 23 healthy individuals. In this group there were 163 participants with serum 25OHD levels less than 30 ng/mL. These individuals received vitamin D3 treatment according to the protocol that was created by reviewing evidence from past literature.
The researchers administered vitamin D3 based on whether patients were an inpatient or in the ICU and which group they were in. The total time the vitamin D was administered ranged from 14 days for inpatients to three days for ICU patients.
Researchers measured peripheral blood samples in all their patients on Days 1 through 3 before treatment and on Day 7 and Day 14 in those who received treatment. Participants in the prospective group were also treated according to the current national guidelines, which at the time did not recommend vitamin D supplementation.
The treatment protocol increased the serum 25OHD level significantly above 30 ng/mL within two weeks in those receiving the intervention. They found that vitamin D treatment shortened the length of hospitalization in those with COVID-19, even when there were comorbidities present. They concluded:10
“Having vitamin D treatment decreased the mortality rate by 2.14 times. It has been determined that vitamin D supplementation is effective on various targeted parameters; therefore, it is an important parameter for the course of COVID-19, and serum vitamin D levels and correlation analyses between these parameters confirm this inference.”
Further Evidence Vitamin D Impacts COVID Outcome
There is strong scientific evidence that vitamin D plays a central role in your immune response and your ability to fight infections. In this video, Ivor Cummins, biochemist and chief program officer for Irish Heart Disease Awareness, explains how recent studies supporting higher levels of vitamin D may reduce your risk of negative outcomes from COVID-19.
He also identifies some of the conditions known to be associated with low vitamin D levels. These include low sun exposure, insulin and leptin resistance, high levels of inflammation and a poor diet. One study Cummins reviews was released by Mark Alipio, who received no funding for his work.11
The data was an analysis of 212 people who had lab-confirmed COVID-19 and for whom serum 25OHD levels were available. Alipio used the classification system based on past research similar to the four categories used in the featured Nutrients study. The difference was that two categories from the featured study were combined, but the classification of the other two remained the same.
Alipio discovered that vitamin D levels were strongly correlated to the severity of illness. As you can see in the graphic Cummins used from the study at minute 2:20 in the video above, of the 49 who had mild illness, 47 had vitamin D levels above 30 ng/mL. It is important to note that most experts consider this level roughly half of what optimal vitamin D levels should be, which is 40ng/mL to 60ng/mL.12
This means 96% of the patients with mild illness had normal levels of vitamin D.13 Of the other two categories combining severe or critical illness, only 4% had normal levels of vitamin D.
One early study14 hypothesized that vitamin D protects the body against SARS-CoV-2 infections and sought to assess if there was an association between vitamin D levels and the number of COVID-19 infections. The data included only European countries and found a significant relationship between the mean (average) vitamin D level and the number of infections.15
People who were most vulnerable to this respiratory infection were the most deficient. Another early study that evaluated the role vitamin D deficiency plays in preventing respiratory infections found similar results.16 The researchers wrote that vitamin D had:17
“… significant protective effect when it was given daily or weekly to people with lowest vitamin D levels: the risk of having at least one ARI was reduced from 60% to 32% in these people.”
Later studies throughout 2020 and 2021 have added to the mounting evidence that vitamin D has a significant effect on the severity and mortality of people with COVID-19 and may help reduce hospitalization rates.
Low vitamin D is associated with rising inflammatory cytokines and increased risk of pneumonia and respiratory tract infections.18
Vitamin D influences the regulation of the inflammatory cascade and deficiency is associated with “increased risk of infections including influenza virus, tuberculosis (TB), human immunodeficiency virus (HIV) and the recent pandemic due to severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2).”19
Vitamin D deficiency increases risk of COVID-19 severity and mortality.20
Vitamin D reduces inflammation caused by T-cells, which could potentially benefit people with COVID-19.21,22
Literature review showed serum levels of vitamin D are associated with the risk of infection, severity of illness and mortality from COVID-19.23
Vitamin D deficiency is associated with increased risk of infection, severity of illness and mortality from COVID-19; presented at the American Society for Bone and Mineral Research 2021 Annual Meeting.24
Data revealed that 83% of 11,901 patients from 23 studies were either deficient or had insufficient levels of vitamin D making the odds of getting infected 3.3 times higher and developing severe disease five times higher in those with deficiency.25
The active form of vitamin D can inhibit the replication of SARS-CoV-2, the virus that causes COVID-19.26,27
Vitamin D deficiency in 489 patients increased the risk of testing positive by 1.77 times compared to those with sufficient levels. Deficiency was defined by levels of 25OHD of less than 20ng/mL.28
Bolus vitamin D supplementation in frail elderly just before or during COVID-19 was associated with better survival rates and less severe disease.29
Study demonstrated the association between vitamin D deficiency and severity and mortality from COVID-19.30
Vitamin D supplementation may prevent COVID-19 or treat the disease in adults and children.31
Top Signs You May Have a Vitamin D Deficiency
The only way to definitively identify a vitamin D deficiency is through blood testing. However, there are some general signs and symptoms that may indicate you should get your vitamin D tested sooner rather than later.
Ongoing musculoskeletal pain or achy bones32
Frequent illnesses or infections33
Neurological symptoms,34 including depression35
Fatigue and daytime sleepiness36,37
Head sweating38
One of the easiest and most cost-effective ways of measuring your vitamin D level is to participate in GrassrootsHealth’s D*Action,39 which is a vitamin D intervention population program. The test is done in the convenience of your home and the results are sent directly to you.
Those at highest risk of dying from COVID-19 are also at highest risk of dying from the COVID shot. The shots are also causing severe heart damage in younger people whose risk of dying from COVID is inconsequential
While you only get at most six months’ worth of protection from the COVID shot, each injection will cause damage for 15 months as your body continuously produces toxic spike protein
The spike protein is responsible for COVID-19-related heart and vascular problems, and it has the same effect when produced by your own cells. It causes blood clots, myocarditis and pericarditis, strokes, heart attacks and neurological damage, just to name a few
The safety signal is very clear, with 19,249 deaths having been reported to the U.S. Vaccine Adverse Events Reporting System as of November 19, 2021. Historically, drugs and vaccines are pulled off the market after about 50 suspected deaths
Children aged 12 to 17 are five times more likely to be hospitalized with COVID jab-induced myocarditis than they are to be hospitalized for COVID-19 infection
The video above features Dr. Peter McCullough, a cardiologist, internist and epidemiologist, and editor of two peer-review journals, who has been on the media and medical frontlines fighting for early COVID treatment. McCullough has also been outspoken about the potential dangers of the COVID shots, and the lack of necessity for them. Curiously, agencies that are currently calling the shots do not have the authority to dictate how medicine is practiced.
The U.S. Food and Drug Administration, for example, has no power to tell doctors what to do or how to treat patients. The National Institutes of Health are a government research organization and cannot tell doctors how to treat patients.
Ditto for the U.S. Centers for Disease Control and Prevention, which is an epidemiologic analysis organization. It is the job of practicing doctors to identify appropriate and effective treatment protocols, which is precisely what McCullough has been doing since the start of this pandemic.
In August 2020, McCullough’s landmark paper “Pathophysiological Basis and Rationale for Early Outpatient Treatment of SARS-CoV-2 Infection” was published online in the American Journal of Medicine.1
A follow-up paper, “Multifaceted Highly Targeted Sequential Multidrug Treatment of Early Ambulatory High-Risk SARS-CoV-2 Infection (COVID-19)” was published in Reviews in Cardiovascular Medicine in December 2020.2 It became the basis for a home treatment guide.
COVID Shots Are Dangerous and Ineffective
When it comes to the COVID injections, McCullough cites research showing those at highest risk of dying from COVID-19 are also at highest risk of dying from the COVID shot. Additionally, the shots are causing severe heart damage in younger people whose risk of dying from COVID is inconsequential.
He points out the safety signal is very clear, with 19,249 deaths having been reported to the U.S. Vaccine Adverse Events Reporting System as of November 19, 2021.3
The signal is also consistent both internally and externally. A number of side effects are reported in high numbers, and very close to the time of injection, that validate the suspicion that the shots are at fault. The U.S. data are also consistent with data from other countries, such as the Yellow Card system in the U.K.
Despite that, not a single safety review has been conducted to weed out risk factors and the like. “We’re almost a year into the program and there’s been no attempt at risk mitigation,” McCullough says. At the same time, there have been gross attempts to coerce Americans into taking the shots — everything from free beer or a free lap dance, to million-dollar lotteries and paid scholarships to state universities.
Such enticements are an undeniable violation of research ethics that strictly forbid any and all kinds of coercion of human subjects. As suspected and predicted, no sooner had bribery stopped working than government officials started talking about vaccine mandates.
President Biden infamously stated that his patience with “vaccine hesitancy” was “wearing thin.” The insinuation was that if people didn’t get the shot, they’d face serious repercussions, and we’re now seeing those repercussions play out day by day, as people are being fired and kicked out of school for refusing the jab.
Meanwhile, they haven’t even determined which vaccine is the most effective, which is remarkable. If government really wanted to end the pandemic with a vaccine, wouldn’t they determine which shot works the best and promote the use of that? But no, they tell us any shot will do.
“The fact that there’s no safety report, they’re not telling you if you’re taking the best vaccine, the fact that it’s kind of in a distorted way linked to your ability to work and go to school, that we’re violating the Nuremberg Code, violating the declaration of Helsinki — it’s just not adding up. It’s not looking good for those who are promoting the vaccine,” McCullough says.
Add to all that the now-clear finding that the shots offer only limited protection for a very short time — six months at best. According to McCullough, there are more than 20 studies showing efficacy drops to nothing at the six-month mark. They’ve also had very limited effectiveness against the Delta variant, which has been the predominant strain for several months.
Why Booster Treadmill Is Such a Health Hazard
I’ve often stated that, in all likelihood, your risk of side effects will rise with each additional shot. McCullough cites research showing your body will produce the toxic SARS-CoV-2 spike protein for 15 months.
If your body is still producing the spike protein — which is what’s causing the blood clots and cardiovascular damage — and you take an additional shot every six months, there will come a time when your body simply cannot withstand the damage being caused by all the spike protein being produced.
Also consider this: While you only get at most six months’ worth of protection from any given shot, each injection will cause damage for 15 months. If we continue with boosters, eventually, it’s going to be impossible to ever clear out the spike protein.
While the spike protein is the part of the virus chosen as the antigen, the part that triggers an immune response, it’s also the part of the virus that causes the worst disease. The spike protein is responsible for COVID-19-related heart and vascular problems, and it has the same effect when produced by your own cells.
It causes blood clots, myocarditis and pericarditis, strokes, heart attacks and neurological damage, just to name a few. As noted by McCullough, the spike protein of this virus was genetically engineered to be more dangerous to humans than any previous coronavirus, and that is what the COVID shots are programming your cells to produce. “They’re just grossly unsafe for human use,” McCullough says.
Myocarditis Will Likely Be Widespread
He goes on to discuss research from 2017,4 which showed myocarditis in children and youth occurs at a rate of four cases per million per year. Assuming there are 60 million American children, the background rate for myocarditis would be 240 cases a year. How many cases of myocarditis have been reported to VAERS following COVID injection so far? 14,428 as of November 19, 2021.5
“Doctors have never seen so many cases of myocarditis,” McCullough says, citing research showing that among children between the ages of 12 and 17, 87% are hospitalized after receiving the shot. “That’s how dangerous it is,” he says. “It is frequent, and it is severe.”
Yet the FDA claims myocarditis after the COVID shot is “rare and mild.” We’re now also getting reports of fatal cases of myocarditis in adults in their 30s and 40s. “Myocarditis right now looks like an unqualified disaster,” McCullough says, both for younger people and adults.
Sadly, children also reap no benefit from the shots, so it’s all risk and no benefit for them. McCullough points out there has been no recorded school outbreaks and no child-to-teacher transmission. He estimates 80% of school aged children are already immune, which would explain this.
Meanwhile, research cited in the interview found that children aged 12 to 17 are five times more likely to be hospitalized with COVID jab-induced myocarditis than they are to be hospitalized for COVID infection. These data counter the claim that COVID-induced heart problems are a far greater problem than “vaccine”-induced heart damage.
And let’s not forget, if you take a COVID shot, you have a 100% chance of being exposed to whatever risk is associated with that shot. On the other hand, if you decline the injection, it’s not 100% chance you’ll get COVID-19, let alone die from it. You have a less than 1% chance of being exposed to SARS-CoV-2 and getting sick.
So, it’s 100% deterministic that taking the shot exposes you to the risks of the shot, and less than 1% deterministic that you’ll get COVID if you don’t take the shot.
COVID-19 Unrelated to Vaccination Rates
As noted by McCullough, rates of COVID are higher now in the highest vaccinated areas than they were before the vaccine rollout. That too tells us they aren’t working and not worth the risk.
He cites research6 published September 30, 2021, in the European Journal of Epidemiology, which found no relationship between COVID-19 cases and levels of vaccination in 68 countries worldwide and 2,947 counties in the U.S. If anything, areas with high vaccination rates had slightly higher incidences of COVID-19. According to the authors:7
“[T]he trend line suggests a marginally positive association such that countries with higher percentage of population fully vaccinated have higher COVID-19 cases per 1 million people.”
Iceland and Portugal, for example, where more than 75% of their populations are fully vaccinated, had more COVID-19 cases per 1 million people than Vietnam and South Africa, where only about 10% of the populations are fully vaccinated.8 Data from U.S. counties showed the same thing. New COVID-19 cases per 100,000 people were “largely similar,” regardless of the percentage of a state’s population that was fully vaccinated.
“There … appears to be no significant signaling of COVID-19 cases decreasing with higher percentages of population fully vaccinated,” the authors wrote.9 Notably, out of the five U.S. counties with the highest vaccination rates — ranging from 84.3% to 99.9% fully vaccinated — four of them were on the U.S. Centers for Disease Control and Prevention’s “high transmission” list. Meanwhile, 26.3% of the 57 counties with “low transmission” have vaccination rates below 20%.
The study even accounted for a one-month lag time that could occur among the fully vaccinated, since it’s said that it takes two weeks after the final dose for “full immunity” to occur. Still, “no discernable association between COVID-19 cases and levels of fully vaccinated” was observed.10
Hospitalization rates for severe COVID infection have also risen, from 0.01% in January 2021 to 9% in May 2021, and the COVID death rate rose from zero percent to 15.1% in that same timeframe.11 In short, everything is getting worse, not better, the more people get these shots.
Allowing natural immunity to build is really the only rational way forward. But then again, the COVID jabs aren’t about protecting public health. They’re about ushering in a socio-economic control system via vaccine passports, which is something McCullough doesn’t discuss in this interview. Nothing makes sense if you look at it from a medical standpoint. It only makes sense if you see it for what it is, which is a control system.
Natural Immunity Is ‘Infinitely Better’ Than Vaccine Immunity
According to McCullough, “natural immunity is infinitely better than vaccine immunity,” and studies have borne that out time and again. The reason natural immunity is superior to vaccine-induced immunity is because viruses contain five different proteins.
The COVID shot induces antibodies against just one of those proteins, the spike protein, and no T cell immunity. When you’re infected with the whole virus, you develop antibodies against all parts of the virus, plus memory T cells.
This also means natural immunity offers better protection against variants, as it recognizes several parts of the virus. If there are significant alternations to the spike protein, as with the Delta variant, vaccine-induced immunity can be evaded. Not so with natural immunity, as the other proteins are still recognized and attacked.
Here’s a sampling of scholarly publications that have investigated natural immunity as it pertains to SARS-CoV-2 infection. There are several more in addition to these:12
Science Immunology October 202013 found that “RBD-targeted antibodies are excellent markers of previous and recent infection, that differential isotype measurements can help distinguish between recent and older infections, and that IgG responses persist over the first few months after infection and are highly correlated with neutralizing antibodies.”
The BMJ January 202114 concluded that “Of 11, 000 health care workers who had proved evidence of infection during the first wave of the pandemic in the U.K. between March and April 2020, none had symptomatic reinfection in the second wave of the virus between October and November 2020.”
Science February 202115 reported that “Substantial immune memory is generated after COVID-19, involving all four major types of immune memory [antibodies, memory B cells, memory CD8+ T cells, and memory CD4+ T cells].
About 95% of subjects retained immune memory at ~6 months after infection. Circulating antibody titers were not predictive of T cell memory. Thus, simple serological tests for SARS-CoV-2 antibodies do not reflect the richness and durability of immune memory to SARS-CoV-2.”
A 2,800-person study found no symptomatic reinfections over a ~118-day window, and a 1,246-person study observed no symptomatic reinfections over 6 months.
A February 2021 study posted on the prepublication server medRxiv16 concluded that “Natural infection appears to elicit strong protection against reinfection with an efficacy ~95% for at least seven months.”
An April 2021 study posted on medRxiv17 reported “the overall estimated level of protection from prior SARS-CoV-2 infection for documented infection is 94.8%; hospitalization 94.1%; and severe illness 96·4%. Our results question the need to vaccinate previously-infected individuals.”
Another April 2021 study posted on the preprint server BioRxiv18 concluded that “following a typical case of mild COVID-19, SARS-CoV-2-specific CD8+ T cells not only persist but continuously differentiate in a coordinated fashion well into convalescence, into a state characteristic of long-lived, self-renewing memory.”
A May 2020 report in the journal Immunity19 confirmed that SARS-CoV-2-specific neutralizing antibodies are detected in COVID-19 convalescent subjects, as well as cellular immune responses. Here, they found that neutralizing antibody titers do correlate with the number of virus-specific T cells.
A May 2021 Nature article20 found SARS-CoV-2 infection induces long-lived bone marrow plasma cells, which are a crucial source of protective antibodies. Even after mild infection, anti-SARS-CoV-2 spike protein antibodies were detectable beyond 11 months’ post-infection.
A May 2021 study in E Clinical Medicine21 found “antibody detection is possible for almost a year post-natural infection of COVID-19.” According to the authors, “Based on current evidence, we hypothesize that antibodies to both S and N-proteins after natural infection may persist for longer than previously thought, thereby providing evidence of sustainability that may influence post-pandemic planning.”
Cure-Hub data22 confirm that while COVID shots can generate higher antibody levels than natural infection, this does not mean vaccine-induced immunity is more protective. Importantly, natural immunity confers much wider protection as your body recognizes all five proteins of the virus and not just one. With the COVID shot, your body only recognizes one of these proteins, the spike protein.
A June 2021 Nature article23 points out that “Wang et al. show that, between six and 12 months after infection, the concentration of neutralizing antibodies remains unchanged. That the acute immune reaction extends even beyond six months is suggested by the authors’ analysis of SARS-CoV-2-specific memory B cells in the blood of the convalescent individuals over the course of the year.
These memory B cells continuously enhance the reactivity of their SARS-CoV-2-specific antibodies through a process known as somatic hypermutation. The good news is that the evidence thus far predicts that infection with SARS-CoV-2 induces long-term immunity in most individuals.”
Reinfection Is Very Rare
McCullough stresses there is also no need to worry about reinfection if you’ve already had COVID once. The fact is, while breakthrough cases continue among those who have gotten one or more COVID-19 injections, it’s extremely rare to get COVID-19 after you’ve recovered from the infection.
How rare? Researchers from Ireland conducted a systematic review including 615,777 people who had recovered from COVID-19, with a maximum duration of follow-up of more than 10 months.24
“Reinfection was an uncommon event,” they noted, “with no study reporting an increase in the risk of reinfection over time.” The absolute reinfection rate ranged from 0% to 1.1%, while the median reinfection rate was just 0.27%.25,26,27
Another study revealed similarly reassuring results. It followed 43,044 SARS-CoV-2 antibody-positive people for up to 35 weeks, and only 0.7% were reinfected. When genome sequencing was applied to estimate population-level risk of reinfection, the risk was estimated at 0.1%.28
There was no indication of waning immunity over seven months of follow-up, unlike with the COVID-19 injection, which led the researchers to conclude that “Reinfection is rare. Natural infection appears to elicit strong protection against reinfection with an efficacy >90% for at least seven months.”29
“It’s a one-and-done,” McCullough says. If you’ve had it once, you won’t get it again. He also advises against using PCR testing after you’ve had confirmed COVID-19 once, as any subsequent positive tests are just going to be false positives.
Early Treatment Options
In closing, should you get COVID-19, know there are several very effective early treatment options, and early treatment is key, both for preventing severe infection and preventing “long-haul COVID.” Here are a few suggestions:
• Oral-nasal decontamination — The virus, especially the Delta variant, replicates rapidly in the nasal cavity and mouth for three to five days before spreading to the rest of the body, so you want to strike where it’s most likely to be found right from the start.
Research30 has demonstrated that irrigating your nasal passages with 2.5 milliliters of 10% povidone-iodine (an antimicrobial) and standard saline, twice a day, is an effective remedy.
Another option that was slightly less effective was using a mixture of saline with half a teaspoon of sodium bicarbonate (an alkalizer). You can also gargle with these to kill viruses in your mouth and throat. When done routinely, it can be a very effective preventive strategy. You can find printable treatment guides on TruthForHealth.org.
• Nebulized peroxide — A similar strategy is to use nebulized hydrogen peroxide, diluted with saline to a 0.1% solution. Both hydrogen peroxide and saline31,32 have antiviral effects.
In a May 10, 2021, Orthomolecular Medicine press release,33 Dr. Thomas E. Levy — board-certified in internal medicine and cardiology — discussed the use of this treatment for COVID-19 specifically. Levy has in fact written an entire book on peroxide nebulization called “Rapid Virus Recovery,” which you can download for free from MedFox Publishing.
• Vitamin D optimization — Research has shown having a vitamin D level above 50 ng/mL brings the risk of COVID mortality down to near-zero.34
• Other key nutraceuticals — Vitamin C, zinc, quercetin and NAC all have scientific backing.
• Key drugs — For acute infection, ivermectin, hydroxychloroquine or monoclonal antibodies can be used. While monoclonal antibodies and hydroxychloroquine must be used early on in the disease process, ivermectin has been shown to be effective in all stages of the infection.
Doxycycline or azithromycin are typically added as well, to address any secondary bacterial infection, as well as inhaled budesonide (a steroid). Oral steroids are used on and after the fifth day for pulmonary weakness and aspirin or NAC can be added to reduce the risk of clotting. In the interview, McCullough discusses the use of each of these, and other, drugs.
One drug I disagree with is full-strength aspirin. I believe a potentially better, at least safer, alternative would be to use the enzymes lumbrokinase and serrapeptase, as they help break down and prevent blood clots naturally.
Sidney Powell revealed that she’s discovered that the Department of Defense patented an algorithm in 2006 that can predetermine the outcome of elections. The DoD then gave that patent to a University in New Jersey, which Sidney calls an “international think tank.”
She also says that Dominion Voting Systems assigned all of their patents in 2019 to the Hong Kong Shanghai Bank, and then there was an “infusion of over $400 million to State Street Capital which owns Dominion now.”
It’s all tied together and it looks like we are starting to get a better understanding of how they’ve rigged our elections for years and more importantly, WHO has been doing it.
This is mind blowing stuff. If you watch the full 8 minute clip, you’ll understand why they are trying to destroy Sidney.
As she says, it’s appears she is over the target 🎯
The food industry shifted away from saturated fat and cholesterol to improve public health, and the medical industry has massively promoted the use of cholesterol-lowering statin drugs for the same reason. Despite that, the rate of heart disease deaths has steadily risen
Research has found that the more LDL (so-called “bad”) cholesterol is lowered, the greater the risk of heart attacks and strokes
The Minnesota Coronary Experiment, published in 2016, found replacing saturated fat with vegetable oil increased mortality and cardiovascular events, even though total cholesterol was lowered by 13.8%. For each 30 mg/dL reduction in serum cholesterol, the death risk rose by 22%
Since the commercialization of statin drugs in the late ‘80s, total sales have reached nearly $1 trillion. Lipitor is the most profitable drug in the history of medicine. Yet these drugs have done nothing to derail the rising trend of heart disease
While there are studies claiming to show statins lower your risk of heart attack, many involve misleading plays on statistics. Statins also have many serious side effects
This article was previously published August 26, 2020, and has been updated with new information.
The lecturer in the featured video, Maryanne Demasi, Ph.D., produced the 2014 Australian Catalyst documentary, “Heart of the Matter: Dietary Villains,” which exposed the cholesterol/saturated fat myths behind the statin fad and the financial links which lurk underneath.
The documentary was so thorough that vested interests actually convinced ABC TV to rescind the two-part series.1 The Australian Heart Foundation, the three largest statin makers (Pfizer, AstraZeneca and Merck Sharp & Dohme) and Medicines Australia, Australia’s drug lobby group, complained2 and got the documentary expunged from ABC TV.
Cholesterol and saturated fat have been the villains of heart disease for the past four decades, despite the many studies showing neither has an adverse effect on heart health.
The entire food industry shifted away from saturated fat and cholesterol, ostensibly to improve public health, and the medical industry has massively promoted the use of cholesterol-lowering statin drugs for the same reason. Despite all of that, the rate of heart disease deaths continues to be high.3 That really should tell us something.
Statins Are a Colossal Waste of Money
Since the release of Demasi’s documentary, the evidence against the cholesterol theory and statins has only grown. As noted in an August 4, 2020, op-ed by Dr. Malcolm Kendrick, a general practitioner with the British National Health Service:4
“New research shows that the most widely prescribed type of drug in the history of medicine is a waste of money. One major study found that the more ‘bad’ cholesterol was lowered, the greater the risk of heart attacks and strokes.
In the midst of the COVID-19 pandemic, almost every other medical condition has been shoved onto the sidelines. However, in the UK last year, heart attacks and strokes (CVD) killed well over 100,000 people — which is at least twice as many as have died from COVID-19.
CVD will kill just as many this year, which makes it significantly more important than COVID-19, even if no one is paying much attention to it right now.”
According to a scientific review5 published online August 4, 2020, in BMJ Evidence-Based Medicine, lowering LDL is not going to lower your risk of heart disease and stroke. “Decades of research has failed to show any consistent benefit for this approach,” the authors note.
Since the commercialization of statin drugs in the late ’80s (lovastatin being the first one, gaining approval in 19876), total sales have reached nearly $1 trillion.7,8 Lipitor — which is just one of several brand name statin drugs — was named the most profitable drug in the history of medicine.9,10 Yet these drugs have done nothing to derail the rising trend of heart disease.
Lowering Cholesterol Does Not Show a Beneficial Impact
According to a press release announcing the BMJ Evidence-Based Medicine review, the analysis found that:11
“… over three quarters of all the trials reported no positive impact on the risk of death and nearly half reported no positive impact on risk of future cardiovascular disease.
And the amount of LDL cholesterol reduction achieved didn’t correspond to the size of the resulting benefits, with even very small changes in LDL cholesterol sometimes associated with larger reductions in risk of death or cardiovascular ‘events,’ and vice versa. Thirteen of the clinical trials met the LDL cholesterol reduction target, but only one reported a positive impact on risk of death …”
In their paper,12 the study authors argue that since dozens of randomized controlled trials looking at LDL-cholesterol reduction “have failed to demonstrate a consistent benefit, we should question the validity of this theory.”
They also cite the Minnesota Coronary Experiment,13 a double-blind randomized controlled trial involving 9,423 subjects that sought to determine whether replacing saturated fat with omega-6 rich vegetable oil (corn oil and margarine) would reduce the death rate from heart disease by lowering cholesterol.
It didn’t. Mortality and cardiovascular events increased even though total cholesterol was lowered by 13.8%. For each 30 mg/dL reduction in serum cholesterol, the death risk rose by 22%. In conclusion, the Evidence-Based Medicine study authors note that:14
“In most fields of science the existence of contradictory evidence usually leads to a paradigm shift or modification of the theory in question, but in this case the contradictory evidence has been largely ignored, simply because it doesn’t fit the prevailing paradigm.”
Deception Through Statistics
If lowering cholesterol doesn’t reduce mortality or cardiovascular events, there’s little reason to use them, considering they come with a long list of adverse side effects. Sure, there are studies claiming to show benefit, but many involve misleading plays on statistics.
One common statistic used to promote statins is that they lower your risk of heart attack by about 36%.15 This statistic is derived from a 2008 study16 in the European Heart Journal. One of the authors on this study is Rory Collins, who heads up the CTT Collaboration (Cholesterol Treatment Trialists’ Collaboration), a group of doctors and scientists who analyze study data17 and report their findings to regulators and policymakers.
Table 4 in this study shows the rate of heart attack in the placebo group was 3.1% while the statin group’s rate was 2% — a 36% reduction in relative risk. However, the absolute risk reduction — the actual difference between the two groups, i.e., 3.1% minus 2% — is only 1.1%, which really isn’t very impressive.
In other words, in the real world, if you take a statin, your chance of a heart attack is only 1.1% lower than if you’re not taking it. At the end of the day, what really matters is what your risk of death is the absolute risk. The study, however, only stresses the relative risk (36%), not the absolute risk (1.1%).
As noted in the review18 “How Statistical Deception Created the Appearance That Statins Are Safe and Effective in Primary and Secondary Prevention of Cardiovascular Disease,” it’s very easy to confuse and mislead people with relative risks.
Statins Sabotage Your Health
A stunning review of statin trials published in 2015 found that in primary prevention trials, the median postponement of death in those taking statins was a mere 3.2 days. While potentially extending life span by 3.2 days, those taking statins are also at increased risk for:
Diabetes (if taken for more than two years, your risk for diabetes triples)
Dementia, neurodegenerative diseases and psychiatric problems such as depression, anxiety and aggression
Musculoskeletal disorders
Osteoporosis
Cataracts
Heart disease
Liver damage
Immune system suppression
Oftentimes statins do not have any immediate side effects, and they are quite effective, capable of lowering cholesterol levels by 50 points or more. This is often viewed as evidence that your health is improving. Side effects that develop over time are frequently misinterpreted as brand-new, separate health problems.
Crimes Against Humanity
The harm perpetuated by the promotion of the low-fat, low-cholesterol myth is so significant, it could easily be described as a crime against humanity. Ancel Keys’ 1963 “Seven Countries Study” was instrumental in creating the saturated fat myth.19,20
He claimed to have found a correlation between total cholesterol concentration and heart disease, but in reality this was the result of cherry picking data. When data from 16 excluded countries are added back in, the association between saturated fat consumption and mortality vanishes.
In fact, the full data set suggests that those who eat the most saturated animal fat tend to have a lower incidence of heart disease, which is precisely what other, more recent studies have concluded.
Procter & Gamble Co.21 (the maker of Crisco22), the American Heart Association and the Center for Science in the Public Interest (CSPI) all promoted the fallacy for decades, despite mounting evidence that Keys had gotten it all wrong.
The AHA was issuing stern warnings against butter, steak and coconut oil as recently as 2017.23That same year, Procter & Gamble partnered with University Hospitals Harrington Heart & Vascular Institute to promote heart health by lowering cholesterol.24
CSPI was also instrumental in driving heart disease skyward with its wildly successful pro-trans fat campaign. It was largely the result of CSPI’s campaign that fast-food restaurants replace beef tallow, palm oil and coconut oil with partially hydrogenated vegetable oils, which were high in synthetic trans fats linked to heart disease and other chronic diseases.
As late as 1988, CSPI praised trans fats, saying “there is little good evidence that trans fats cause any more harm than other fats” and that “much of the anxiety over trans fats stems from their reputation as ‘unnatural.'”25
CSPI and AHA Omit Their Role in Heart Disease Epidemic
Today, you’ll have to dig deep to unearth CSPI’s devastating public health campaign. In an act of deception, they erased it from their history to make people believe they’ve been doing the right thing all along. Their historical timeline26 of trans fat starts at 1993 — the year CSPI decided to change course and start supporting the elimination of the same trans fat they’d spent years promoting.
Similarly, the AHA conveniently omits saturated fat and cholesterol from its history of “lifesaving” breakthroughs and achievements.27 It makes sense, though, considering the AHA’s and CSPI’s recommendations to swap saturated fat for vegetable oils and synthetic trans fat never resulted in anything but an epidemic of heart disease.
The idea that the harms of trans fats were unknown until the 1990s is simply a lie. The late Dr. Fred Kummerow started publishing evidence showing trans fat, not saturated fat, was the cause of heart disease in 1957. He also linked trans fat to Type 2 diabetes.
The Truth About Saturated Fat
In addition to the more recent studies mentioned earlier, many others have also debunked the idea that cholesterol and/or saturated fat impacts your risk of heart disease. For example:
• In a 1992 editorial published in the Archives of Internal Medicine,28 Dr. William Castelli, a former director of the Framingham Heart study, stated:
“In Framingham, Mass., the more saturated fat one ate, the more cholesterol one ate, the more calories one ate, the lower the person’s serum cholesterol. The opposite of what … Keys et al [said] …”
• A 2010 meta-analysis,29 which pooled data from 21 studies and included 347,747 adults, found no difference in the risks of heart disease and stroke between people with the lowest and highest intakes of saturated fat.
• Another 2010 study30 published in the American Journal of Clinical Nutrition found that a reduction in saturated fat intake must be evaluated in the context of replacement by other macronutrients, such as carbohydrates.
When you replace saturated fat with a higher carbohydrate intake, particularly refined carbohydrate, you exacerbate insulin resistance and obesity, increase triglycerides and small LDL particles, and reduce beneficial HDL cholesterol. According to the authors, dietary efforts to improve your cardiovascular disease risk should primarily emphasize the limitation of refined carbohydrate intake, and weight reduction.
• A 2014 meta-analysis31 of 76 studies by researchers at Cambridge University found no basis for guidelines that advise low saturated fat consumption to lower your cardiac risk, calling into question all of the standard nutritional guidelines related to heart health. According to the authors:
“Current evidence does not clearly support cardiovascular guidelines that encourage high consumption of polyunsaturated fatty acids and low consumption of total saturated fats.”
Will Saturated Fat Myth Soon Be Upended?
Nina Teicholz, a science journalist, adjunct professor at NYU’s Wagner Graduate School of Public Service and the executive director of The Nutrition Coalition, is the author of “The Big Fat Surprise: Why Butter, Meat and Cheese Belong in a Healthy Diet,” which reviews the many myths surrounding saturated fat and cholesterol.
In an interview I did with Dr. Paul Saladino and Teicholz, they reviewed the history of the demonization of saturated fat and cholesterol, starting with Keys, and how the introduction of the first Dietary Guidelines for Americans in 1980 (which recommended limiting saturated fat and cholesterol) coincided with a rapid rise in obesity and chronic diseases such as heart disease.
Teicholz also reviewed a paper32 in the Journal of the American College of Cardiology, published online June 17, 2020, which actually admits the long-standing nutritional guideline to limit saturated fat has been incorrect. This is a rather stunning admission, and a huge step forward. As noted in the abstract:
“The recommendation to limit dietary saturated fatty acid (SFA) intake has persisted despite mounting evidence to the contrary. Most recent meta-analyses of randomized trials and observational studies found no beneficial effects of reducing SFA intake on cardiovascular disease (CVD) and total mortality, and instead found protective effects against stroke.
Although SFAs increase low-density lipoprotein (LDL)-cholesterol, in most individuals, this is not due to increasing levels of small, dense LDL particles, but rather larger LDL which are much less strongly related to CVD risk.
It is also apparent that the health effects of foods cannot be predicted by their content in any nutrient group, without considering the overall macronutrient distribution.
Whole-fat dairy, unprocessed meat, eggs and dark chocolate are SFA-rich foods with a complex matrix that are not associated with increased risk of CVD. The totality of available evidence does not support further limiting the intake of such foods.”
In the week ending November 12, 2021, the U.K. reported 2,047 more deaths than occurred during the same period between 2015 and 2019; heart disease and strokes appear to be behind many of the excess deaths
In the last 13 weeks alone, about 107,700 seniors died above the normal rate, despite a 98.7% injection rate
In Vermont, where the majority are also injected, excess deaths are the highest they’ve been since before the pandemic
An investigation using official data from NHS and the U.K.’s Office for National Statistics (ONS) found that deaths among teenagers increased 47% since they started getting COVID-19 shots
Deaths from COVID-19 also went up among 15- to 19-year-olds after the shots were rolled out for this age group
Even with mass injections and some receiving two and even three shots in their arm, excess deaths are rising
Throughout the pandemic, mass injections have been dangled as the way back to normalcy — the only solution to end the pandemic and save lives from COVID-19. Now even with mass injections and some receiving two and even three shots in their arm, excess deaths are rising nonetheless.
In the week ending November 12, 2021, the U.K. reported 2,047 more deaths than occurred during the same period between 2015 and 2019. However, COVID-19 cannot be entirely to blame, as it was listed on the death certificates for only 1,197 people.1 Further, since July, non-COVID deaths in the U.K. have been higher than the weekly average in the five years prior to the pandemic.
Heart disease and strokes appear to be behind many of the excess deaths, with the Financial Times reporting, “The new phase of excess deaths raises the possibility that since the summer more people have been losing their lives as a result of strains on the NHS or lack of early diagnosis of serious illness …”2 A similar scenario is playing out in the U.S.
More Seniors Dying, Despite Mass Injections
On Twitter, Silicon Valley software engineer Ben M. (@USMortality) revealed that in the last 13 weeks alone, about 107,700 seniors died above the normal rate, despite a 98.7% vaccination rate.3In another example, he used data from the U.S. Centers for Disease Control and Prevention, census.gov and his own calculations to show excess deaths rising in Vermont even as the majority of adults have been injected.
“Vermont had 71% of their entire population vaccinated by June 1, 2021,” he tweeted. “That’s 83% of their adult population, yet they are seeing the most excess deaths now since the pandemic!”4
Deaths Among Teenagers Increase After Jabs
An investigation by The Exposé, using official data from NHS and the U.K.’s Office for National Statistics (ONS), found that deaths among teenagers increased 47% since they started getting COVID-19 shots.5 Not only that, but deaths from COVID-19 also went up among 15- to 19-year-olds after the shots were rolled out for this age group.
“We decided to take a look at official Office for National Statistics (ONS) data on deaths registered weekly to see if there was an uptick in deaths in people aged between 15 and 19 following the rollout of the Covid-19 vaccine to this age group,” the report notes.6
Between the week ending June 26 and the week ending September 18, 2020, 148 deaths were reported among 15- to 19-year-olds. However, between the week ending June 25, 2021, and the week ending September 17, 2021, 217 deaths occurred among 15- to 19-year-olds. According to the investigation:7
“This shows that the number of deaths between June 19th 2021 and September 17th 2021 among teens aged 15 and over were 47% higher than the number of deaths in this age group during the same period in 2020, and the increase in deaths began at precisely the same time teens started receiving the Covid-19 vaccine.
Our investigation of ONS data also revealed further concerns about Covid-19 deaths in people between the age of 15 and 19. The same 2021 ONS dataset shows that since teens started getting the Covid-19 vaccine there has been at least one Covid-19 related death recorded in seven of the thirteen weeks between June 19th and September 17th 2021. A total of 8 deaths in this time frame.
Yet in the fifteen weeks prior to teens over the age of 15 receiving the Covid-19 vaccine, just a single death was recorded associated with Covid-19 among this age group.
Correlation does not equal causation, but it is extremely concerning to see that deaths have increased by 47% among teens over the age of 15, and Covid-19 deaths have also increased among this age group since they started receiving the Covid-19 vaccine, and it is perhaps one coincidence too far.”
Significant concerns have been raised, for instance, surrounding antibody‐dependent enhancement (ADE), and the possibility that COVID-19 vaccines could worsen COVID-19 disease via ADE.8
Florida Has Been Heavily Criticized — Wrongly
Certain states have stood out for their refusal to buy into the draconian public health measures that were adopted throughout much of the U.S. Florida is chief among them. After a spring 2020 lockdown, Florida business, schools and restaurants reopened, while mask mandates were rejected.
“If Florida had simply done no worse than the rest of the country during the pandemic, that would have been enough to discredit the lockdown strategy,” John Tierney, a contributing science columnist for The New York Times, stated, noting that the state acted as the control group in a natural experiment. By summer 2021, the results spoke for themselves:9
“Florida’s mortality rate from Covid is lower than the national average among those over 65 and also among younger people, so that the state’s age-adjusted Covid mortality rate is lower than that of all but ten other states. And by the most important measure, the overall rate of ‘excess mortality’ (the number of deaths above normal), Florida has also done better than the national average.
Its rate of excess mortality is significantly lower than that of the most restrictive state, California, particularly among younger adults, many of whom died not from Covid but from causes related to the lockdowns: cancer screenings and treatments were delayed, and there were sharp increases in deaths from drug overdoses and from heart attacks not treated promptly.”
After an uptick in cases in late summer, rates plummeted by the fall. In late October 2021, Florida had one of the lowest COVID-19 daily average case rates per 100,000 residents in the U.S. “Without mandates or lockdowns, COVID-19 cases in Florida have decreased 90% since August,” said Gov. Ron DeSantis. “In addition to cases, hospitalizations have plummeted in our state.”10
Also since August, COVID-19 cases in school-aged children decreased 87% since school started back into session, while cases in young adults ages 18 to 24 decreased 93%11 Lt. Gov. Jeanette Nuñez added in a press release, “As Florida now ranks lowest in the continental U.S. in terms of COVID-19 rates per capita, we are proud to have stood firm in protecting liberty throughout the pandemic.”12
By the end of November 2021, Florida was the only state in the U.S. with low community transmission in virtually every county. While the rest of the U.S. was seeing high, substantial or moderate spread, COVID-19 was largely absent in the sunshine state.13 On Twitter, Scott Ruesterholz wrote:14
“I’ve spoken frequently about how COVID waves clearly are driven by weather (South struggles in the summer; North in the winter). This should be considered when assigning “blame” or “credit” to a governor–some trends supercede policy. Nonetheless this map is something–Florida!”
Shots Double Risk of Acute Coronary Syndrome
It’s concerning that heart-related events appear to be a leading factor behind the excess deaths being seen in the U.K., especially considering researchers have found Pfizer and Moderna mRNA COVID-19 shots dramatically increase biomarkers associated with thrombosis, cardiomyopathy and other vascular events following injection.16
The study, published in the November 16, 2021, issue of the journal Circulation, concluded that “the mRNA vacs dramatically increase inflammation on the endothelium and T cell infiltration of cardiac muscle and may account for the observations of increased thrombosis, cardiomyopathy, and other vascular events following vaccination.”
People who had been jabbed more than doubled their risk of acute coronary syndrome (ACS), an umbrella term that includes not only heart attacks, but also a range of other conditions involving abruptly reduced blood flow to your heart. Signs and symptoms of ACS typically begin very suddenly and include:17
Chest pain/discomfort, often described as aching, pressure, tightness or burning sensations
Pain that radiates from your chest to your shoulders, arms, upper abdomen, back, neck and/or jaw
Nausea and/or vomiting
Indigestion
Shortness of breath
Sudden heavy sweating
Lightheadedness, dizziness and/or fainting
Unusual or inexplicable fatigue
Patients who received a two-dose regimen of mRNA more than doubled their five-year ACS risk, driving it from an average of 11% to 25%. In a November 21, 2021, tweet, cardiologist Dr. Aseem Malhotra wrote:18
“Extraordinary, disturbing, upsetting. We now have evidence of a plausible biological mechanism of how mRNA vaccine may be contributing to increased cardiac events. The abstract is published in the highest impact cardiology journal so we must take these findings very seriously.”
Can You Lessen the Damaging Effects?
If you now believe that getting the COVID-19 jab was a mistake and wish to lessen your doubled risk of cardiac complications, there are a few basic strategies I would advise.
Make certain you measure your vitamin D level and take enough vitamin D orally (typically about 8,000 units/day for most adults) and/or get sensible sun exposure to make sure your level is 60 to 80 ng/ml (150 to 200 nmol/l).
Eliminate all vegetable (seed) oils in your diet, which involves eliminating nearly all processed foods and most meals in restaurants unless you convince the chef to only cook with butter. Avoid any sauces or salad dressings in restaurants as they are loaded with seed oils. Also avoid chicken and pork as they are very high in linoleic acid, the omega-6 fat that is far too high in nearly everyone and contributes to oxidative stress that causes heart disease.
Consider taking around 500 milligrams/day of NAC, as it helps prevent blood clots and is a precursor for your body to produce the important antioxidant glutathione.
Consider fibrinolytic enzymes that digest the fibrin that leads to blood clots, strokes and pulmonary embolisms. The dose is typically two, twice a day, but must be taken on an empty stomach, either an hour before or two hours after a meal. Otherwise, the enzymes will digest your food and not the fibrin in the blood clot.
(Natural News) A new Axios-Ipsos poll has found that 82 percent of all Democrats in the United States are willing to wear a mask indoors at all times now that the “Omicron” (Moronic) variant has arrived. Conversely, only 38 percent of Republicans are willing to do the same.
Axios, which is admittedly far-left, complained that these results show that “[m]ost Americans aren’t willing to make big changes in their behavior to minimize the risk from the Omicron variant, like avoiding indoor restaurant dining or canceling their holiday travel plans.”
It turns out that only 33 percent of Americans overall are willing to stop eating inside at restaurants this winter, and only 28 percent are willing to stop gathering with other people outside of their own household.
That same 28 percent do not want to have to self-quarantine for 14 days again just because the government came up with a new scary “mutation,” and only 23 percent say they would cancel their holiday travel plans over this latest scariant.
Even fewer, just 13 percent, indicated that they will stop going into work. Apparently the vast majority of the country is just not scared about Moronic like the media and government hoped people would be. (RELATED: the only people we know of so far who are “catching” Moronicare the fully vaccinated.)
67 percent of America supposedly supports vaccine mandates for flying
As for another round of mask mandates, a whopping 94 percent of Democrats say they support the government forcing these ‘medical devices’ on people who visit local businesses.
When it comes to murdering unborn children (abortion), Democrats demand that the government stay out of it – my body, my choice, they say. But when it comes to forcing everyone to cover their breathing holes with Chinese plastic, Democrats are all about some medical fascism.
Shockingly, 43 percent of Republicans (if you believe the poll’s results) also said they would support more mask mandates. Overall, 69 percent of the country is supposedly in favor of this.
Axios-Ipsos further claims that 67 percent of the country, including 72 percent of Democrats and 66 percent of Republicans, support a government-imposed travel mandate to help “flatten the curve.”
Where the poll gets even further questionable is the results to the question about whether or not Wuhan coronavirus (Covid-19) “vaccination” should be required in order to fly on commercial airlines. Sixty-seven percent of the country supposedly supports this.
As for more lockdowns, however, only 35 percent of respondents indicated that they support another round of that.
The government claims that the Moronic variant has now been detected in the following 18 states: California, Colorado, Connecticut, Georgia, Hawaii, Louisiana, Maryland, Massachusetts, Minnesota, Missouri, Mississippi, Nebraska, New Jersey, New York, Pennsylvania, Utah, Washington, and Wisconsin.”
Fake “president” Joe Biden has promised to “shut down the virus,” which does not sound too promising for the future of Americans’ last remaining rights and liberties.
“I think 82% of Democrats should wear plastic bags over their heads and tightly tied around their necks,” joked one commenter at Breitbart News about the poll results.
“82% of Democrats are severely mentally ill,” wrote another.
Another wrote that these are the same people he sees “driving in their car alone and wearing a mask with all the windows up.”
“I guess it would be asking too much for them to just shut up and let us enjoy the flu season,” wrote another.
“Remember when the ‘cold and flu season’ was marked by TV ads for Dristan, Nyquil, etc.? We just dealt with it and lived our lives,” wrote another.
You will find more of the latest news about the Omicron variant deception at Propaganda.news.
“VACCINATION GIVES AN INCREASE IN ALL-CAUSE DEATHS; IT’S KILLING OUR NATURAL IMMUNE SYSTEM”.
None of the covid19 vaccines reduce all causes mortality. Worse than that, he is showing that vaccination is slightly INCREASING all causes mortality. It’s been my opinion for sone time that the covid19 vaccines don’t do anything (but they carry risks of injury & deaths)
Source: Norman Fenton YouTube: https://youtu.be/Jxkb2yhdLiA
In this interview Norman Fenton explains the results of a new report that analyses the latest ONS data on mortality of vaccinated v unvaccinated.
Dr Reiner Fuellmich is.a German American lawyer with experience going after large companies like Deutsche Bank. He is a member of the German Corona Investigative Committee. He discusses the current situation and his efforts to bring justice to the situation. This interview was done as apart of the full length documentary. We are releasing the full interview for the betterment of public understanding of the situation. The full film, when released, will be available at PlanetLockdownFilm.com
STORY AT-A-GLANCE Africa Lowest Vaccination Rate = Lowest Death Rate
Scientists appear stymied by the low number of infections and deaths in sub-Saharan Africa where the vaccination rate is less than 6%
Africa has 17.46% of the world’s population and 3% of the COVID-19 global death toll while countries with better health care have higher death rates, including the Americas with 46% and Europe with 29%
Nigeria, with the highest population, has had 3,000 deaths in 200 million people, which is what is recorded in the U.S. every two or three days. Yet, Nigeria has announced an all-out vaccination program to “prepare for the next wave” (fraud)
Factors that may have influenced the low infection and death rate are outdoor living that raises vitamin D levels, a younger population and access to medications and herbs used for other local conditions, but which are also known to reduce the severity of COVID, ie Ivermectin and HCQ Hydroxychloroquine
Whether or not lockdowns, shutdowns and other restrictive measures can work to lower the number of COVID-19 infections and deaths has been a topic of great debate since early 2020. As health experts look at global statistics, they have been stymied by the low rate of infection and death across the sub-Saharan African continent,1 compared to industrialized nations that used various lockdown procedures to contain the spread.
Across the world, countries have taken different approaches to address the spread of SARS-CoV-2. In one short documentary released by CAN films, they compare the COVID-19 outcomes in Scotland and Sweden.2 By March 2020,3 Scotland had implemented strict lockdowns and closed schools and other social venues. People were threatened with police fines if they went outside other than to exercise once a day, go to work or buy food.4
On the other hand, Sweden handled the pandemic differently than most of the globe and was initially vilified for looser restrictions and a lack of severe lockdown measures.5 In October 2020, TIME called the response a “disaster,”6 but data have shown that the death rate in Sweden was in line with other years.7 In other words, excess deaths that may have been attributed to COVID-19 were minimal.
Information compiled by CAN films showed the response in Sweden, which has nearly double the population of Scotland, had significantly less impact on the economy and health of their population, as well as nearly half the percentage of excess deaths as did Scotland.8 Scotland had three lockdowns, 64 school closures and a 54% increase in weight gain, while Sweden had no lockdowns, no school closures and zero weight gain.
Sub-Saharan African Continent Has Avoided COVID-19
Over the Thanksgiving 2021 break, media outlets broke the news of a new COVID-19 variant, dubbed Omicron, that was identified in South Africa.9 This variant is different in that doctors are reporting “unusual,” but mild symptoms, with fatigue being the most common complaint. In response, the rest of the world immediately instituted travel bans to and from South Africa.
Interestingly, the steps taken in Africa throughout the pandemic have varied depending on the country, yet the infection and death rate were relatively stable and low across the continent.10 Over the last year there have been reports of small areas in the world where the number of infections, deaths or case fatality rates have been significantly lower than the rest of the world.
For example,11 India’s Uttar Pradesh State reported a recovery rate of 98.6% and no further infections. On the other hand, the entire continent of Africa appears to have sidestepped the massive number of infections and deaths predicted for these poorly funded countries with overcrowded cities.
Early estimations were that millions would die when the pandemic swept across Africa. However, that scenario has not materialized. According to AP News,12 less than 6% of the continent is vaccinated and for months, the World Health Organization has called Africa “one of the least affected regions in the world.”13
In a busy crowded market outside Harare, AP News spoke with Nyasha Ndou, who carries a mask in his pocket. Hundreds of other people, mostly unmasked, were in the marketplace. Ndou explained the mask in his pocket:14
“COVID-19 is gone, when did you last hear of anyone who has died of COVID-19? The mask is to protect my pocket. The police demand bribes so I lose money if I don’t move around with a mask.”
According to data from WorldoMeter, the population of Africa15 makes up 17.46% of the world’s population16 Yet, AP News reports that the WHO data reveal deaths in Africa are 3% of the global total, while deaths in countries with better health care are much higher, such as 46% in the Americas and 29% in Europe.17
Nigeria has the highest population in Africa and the government has recorded just 3,000 deaths in the 200 million people who live in the country. In the U.S., AP News reports there are that many deaths every two or three days.18
Some Credit Early Lockdowns With Low Number of Infections
Across the world, countries and communities went into lockdown to supposedly help “flatten the curve” and slow the spread of the virus. Lesotho, the southernmost landlocked country in the world and surrounded by South Africa, locked down their country and their borders before a single person got sick.19
In March 2020, the country declared an emergency, closed the schools and went into a three-week lockdown. In early May, the lockdown was lifted, and the country recorded its first confirmed cases. The BBC reported in October 2020 that in a country of 2 million people they recorded 40 deaths in five months and approximately 1,700 cases.20
That number rose to 4,137 cases by January 2021 as citizens from South Africa were crossing the border during the holiday season.21 In addition to border crossings, the government had been releasing people early from quarantine over cost concerns.
However, experts believe thousands of people had crossed the border illegally because they were unable to afford to pay for their COVID-19 test.22 In response to the rising number of COVID-19 cases in January, the prime minister imposed a curfew on social venues such as bars and nightclubs at 8 pm.
While the quick action that some countries took to lock down their population may have slowed the spread of the virus in the early days, the SARS-CoV-2 is endemic. This means that it is in the environment and no amount of lockdown will eliminate the virus.
It also means that once lockdowns are opened again, the virus will continue to spread, just like flu and cold viruses. Countries like Lesotho that locked down early have experienced infections after the lockdown was lifted. The one advantage to flattening the curve and reducing the number of infections early in the pandemic was that doctors could have used the time to improve treatment protocols.
Dr. Vladimir Zelenko23 and the Front Line COVID-19 Critical Care Alliance24 are two examples of physicians and physician groups that developed treatment protocols during 2020 that have proven to be successful25,26,27,28 and reduce the number of individuals with severe disease or long-haul symptoms.
Factors That May Influence the Infection Rate
There are several factors that may influence the infection rates in Africa. In the video above, Dr. John Campbell points to the dramatic reduction in COVID-19 cases in Japan that began in August, just 12 days after doctors were allowed to legally prescribe ivermectin to their patients.29
Using Google Translate,30 Campbell learned Dr. Haruo Ozaki, chairman of the Tokyo Medical Association, had taken notice of the low number of infections and deaths in Africa where many use ivermectin prophylactically31 and as the core strategy to treat onchocerciasis,32 a parasitic disease also known as river blindness. More than 99% of people infected live in 31 African countries.
Other medications that are commonly available in Africa have also demonstrated effectiveness against COVID-19. For example, hydroxychloroquine and chloroquine have long been used in the treatment and prevention of malaria.33 Zelenko has published successful results using hydroxychloroquine against COVID-19.
Malaria is one of the leading causes of death in many developing nations in Africa. The illness is triggered by a parasite carried by an infected female mosquito34 and characterized by flu-like symptoms. Delays in treatment increase the severity of the illness and the risk of death. According to the WHO35 there were 219 million cases of malaria diagnosed in 2017 and 92% of those were in the African region.
Finally, Artemisia annua, also known as sweet wormwood, is an herb used in combination therapies to treat malaria.36 It was used in traditional Chinese medicine for more than 2,000 years to treat fever. Today artemisinin, a metabolite of Artemisia, is the current therapeutic option for malaria. The plant has also been studied since the 2003 SARS outbreak for the treatment of coronaviruses, with good results.37,38
As the BBC39 points out, the average age in most African countries is much lower than in the rest of the world. Since many who have died are over the age of 80, and the median age in Africa is 19 years, infections are far less likely to result in death. Only 3% of the population is over age 65 as compared to 16.9% in North America40 and 19.2% in Europe.41
In addition, residential care facilities for the elderly are rare in most African countries.42 Weather may also play a part in who gets COVID: Early in the pandemic, researchers from the University of Maryland43,44 discovered there was a correlation between the spread of COVID-19 and temperature, humidity and latitude. They found the virus appears to spread better when humidity and temperatures drop.
In addition, temperate weather and sunny skies such as those you see in Africa increase the likelihood that a population will have optimal levels of vitamin D. Researchers have discovered that maintaining optimal levels of vitamin D reduces the potential for infection and lowers the risk of severe disease.45,46,47
How Does Vaccination in Sub-Saharan Africa Make Sense?
The low numbers of COVID-19 in the sub-Saharan African population continue despite a less than 6% vaccination rate. Meanwhile. Western nations’ vaccination rates are soaring, yet they struggle with rising infection and death rates. With statistics like this, why are Nigerian officials seemingly overlooking the country’s low numbers and health status by announcing they would be stepping up their immunization schedule, with hopes to give the shot to half the population before February.48
Put simply, their target is “herd immunity” in a population that is not suffering. Oyewale Tomori, is a virologist from Nigeria who sits on several WHO advisory groups. He believes the vaccination level does not need to be as high as it is in the West. Salim.
But Abdool Karim, an epidemiologist in South Africa who has advised the government in the past on COVID-19, disagrees. He is calling for an all-out vaccination program to “prepare for the next wave,”49 which negates what has happened in Africa in the last 20 months. He says, “Looking at what’s happening in Europe, the likelihood of more cases spilling over here is very high.”
So, as African countries which have had lower rates of infection and deaths since the start of the pandemic vaccinate more and more of their population, one can’t help but wonder: Once vaccination programs are underway, will the death rates climb as they have in other areas of the world where vaccination levels are high?50,51,52
And if they do, how will the “health experts” explain the sudden rising number of infections and deaths on a continent that has thus far avoided pandemic levels of COVID-19?
Robert F. Kennedy Jr., the nephew of former American President John F. Kennedy, in a lengthy piece exposed Bill Gates activities in India and his “obsession with vaccines”. Interestingly, as GreatGameIndia readers may recall, Jr Kennedy’s message come days after Robert Kennedy’s grand-daughter and her son were found dead in suspicious circumstances. Almost as if sounding a warning to the impending tragedy on the Kennedy family, legendary American singer Bob Dylan came out of a decade-long isolation to revive JFK murder mystery with a cryptic single.
UPDATE: A month later, based on an intercepted human intelligence report, a controversy erupted in Nigeria whereby it was revealed that Bill Gates offered $10 million for vaccination program for Coronavirus to the Nigerian House of Representatives.
In Robert Kennedy Jr.’s own words:
Vaccines, for Bill Gates, are a strategic philanthropy that feed his many vaccine-related businesses (including Microsoft’s ambition to control a global vaccination ID enterprise) and give him dictatorial control of global health policy.
Gates’ obsession with vaccines seems to be fueled by a conviction to save the world with technology.
Promising his share of $450 million of $1.2 billion to eradicate Polio, Gates took control of India’s National Technical Advisory Group on Immunization (NTAGI) which mandated up to 50 doses (Table 1) of polio vaccines through overlapping immunization programs to children before the age of five. Indian doctors blame the Gates campaign for a devastating non-polio acute flaccid paralysis (NPAFP) epidemic that paralyzed 490,000 children beyond expected rates between 2000 and 2017. In 2017, the Indian government dialed back Gates’ vaccine regimen and asked Gates and his vaccine policies to leave India. NPAFP rates dropped precipitously.
In 2014, the Gates Foundation funded tests of experimental HPV vaccines, developed by Glaxo Smith Kline (GSK) and Merck, on 23,000 young girls in remote Indian provinces. Approximately 1,200 suffered severe side effects, including autoimmune and fertility disorders. Seven died. Indian government investigations charged that Gates-funded researchers committed pervasive ethical violations: pressuring vulnerable village girls into the trial, bullying parents, forging consent forms, and refusing medical care to the injured girls. The case is now in the country’s Supreme Court.
In 2010, the Gates Foundation funded a phase 3 trial of GSK’s experimental malaria vaccine, killing 151 African infants and causing serious adverse effects including paralysis, seizure, and febrile convulsions to 1,048 of the 5,949 children.
In 2010, Gates committed $10 billion to the WHO saying, “We must make this the decade of vaccines.” A month later, Gates said in a Ted Talk that new vaccines “could reduce population”. In 2014, Kenya’s Catholic Doctors Association accused the WHO of chemically sterilizing millions of unwilling Kenyan women with a “tetanus” vaccine campaign. Independent labs found a sterility formula in every vaccine tested. After denying the charges, WHO finally admitted it had been developing the sterility vaccines for over a decade. Similar accusations came from Tanzania, Nicaragua, Mexico, and the Philippines.
A 2017 study (Morgenson et. al. 2017) showed that WHO’s popular DTP vaccine is killing more African children than the diseases it prevents. DTP-vaccinated girls suffered 10x the death rate of children who had not yet received the vaccine. WHO has refused to recall the lethal vaccine which it forces upon tens of millions of African children annually.
Global public health advocates around the world accuse Gates of steering WHO’s agenda away from the projects that are proven to curb infectious diseases: clean water, hygiene, nutrition, and economic development. The Gates Foundation only spends about $650 million of its $5 billion dollar budget on these areas. They say he has diverted agency resources to serve his personal philosophy that good health only comes in a syringe.
In addition to using his philanthropy to control WHO, UNICEF, GAVI, and PATH, Gates funds a private pharmaceutical company that manufactures vaccines, and additionally is donating $50 million to 12 pharmaceutical companies to speed up development of a coronavirus vaccine. In his recent media appearances, Gates appears confident that the Covid-19 crisis will now give him the opportunity to force his dictatorial vaccine programs on American children.
Watch Robert Kennedy Jr’s interview to RT below:
Article authored by Robert Kennedy Jr on Children’s Health Defense titled Gates’ Globalist Vaccine Agenda: A Win-Win for Pharma and Mandatory Vaccination.
Send in your tips and submissions by filling out this form or write to us directly at the email provided. Join us on WhatsApp for more intel and updates.
GreatGameIndia is a journal on Geopolitics and International Relations. Get to know the Geopolitical threats India is facing in our exclusive book India in Cognitive Dissonance. Past magazine issues can be accessed from the Archives section.
Disturbing video out of the UK showing what’s next if we don’t stop the covid mandate hysteria. I also address a ridiculous speech on the House floor by a member of the squad, which proves the left is bedrocked in dishonesty.
Looking for news?
The Bongino Report brings you the top conservative and libertarian news stories of the day, aggregated in an easy to read format to assist the public in getting accurate information. https://bonginoreport.com/
Robert F. Kennedy Jr. describes the coalition of sinister forces — intelligence agencies, pharmaceutical companies, social media titans, medical bureaucracies, mainstream media and the military — that are using a health crisis to impose totalitarian control worldwide
Anthony Fauci isn’t acting alone, but he’s become a prominent face of the medical cartel and medical technocracy that is wrapped up in obliterating constitutional rights globally
Big Pharma’s infiltration of regulatory and public health agencies goes back more than 100 years to the creation of the Rockefeller Foundation in 1913, which took control of the U.S. medical school system
Fauci controls a $6.1 billion budget that he distributes to colleges and universities to do drug research for various diseases, and another $1.7 billion that comes from the military to do bioweapons research
Fauci’s NIAID conducted barbaric and illegal drug experiments on foster children; at least 85 children died as a result
Waking up to Fauci’s façade is necessary to understand the orchestrated planned use of pandemics to clamp down totalitarian control
We’re facing the greatest battle of our lifetimes, possibly of all time, according to Robert F. Kennedy Jr. in this riveting interview with James Corbett.1 I urge you to set aside 60 minutes to watch it in its entirety, as it succinctly sums up the coalition of sinister forces — intelligence agencies, pharmaceutical companies, social media titans, medical bureaucracies, mainstream media and the military — that are using a health crisis to impose totalitarian control worldwide.
You can find all of the details in Kennedy’s bestselling book, “The Real Anthony Fauci,” which contains more than 2,200 footnotes backing up its data. The truth is, Fauci, the director of the National Institute of Allergy and Infectious Diseases (NIAID) — part of the U.S. National Institutes of Health (NIH) — isn’t acting alone.
But he’s become the prominent face of the medical cartel and medical technocracy that is wrapped up in obliterating constitutional rights globally. And, as an authoritative medical figure and trusted adviser to six presidents, Fauci’s words are treated as gospel, despite the atrocities he’s committed.
Regulatory Agencies Turned Into Pharmaceutical Companies
Because of financial entanglements between pharmaceutical companies and the agencies that regulate them, public health agencies in the U.S. have been turned into veritable pharmaceutical companies. The U.S. Food and Drug Administration, for instance, receives 45% of its annual budget from Big Pharma, Kennedy explains.2
The NIH, meanwhile, owns thousands of pharmaceutical patents, and the U.S. Centers for Disease Control and Prevention spends $4.9 billion a year out of its $12 billion budget buying and distributing vaccines. “It is the biggest vaccine company in the world,” Kennedy says. The NIH actually owns half the patent for Moderna’s COVID-19 injection, which means that if the shot is approved and/or mandated, it will make billions of dollars as a result.
“Tony Fauci was able to choose, to designate, four of his high-level employees who each get individual patent shares,” Kennedy explained. “They will collect $150,000 a year for life if the Moderna vaccine is approved, which it has been.”3 Fauci’s agency, the NIAID, in particular, no longer looks out for public health — and Fauci doesn’t either; his priority is pharmaceutical promotion.
How Rockefeller Took Control of the Medical School System
One of the important parts of Kennedy’s new book is exposing the connection of Fauci to Bill Gates and helping uncover how Gates patterned his strategy after Rockefeller. The information was so compelling that I had my team create the video above to put together the facts in the book into an easy-to-watch video so you can digest the material more easily.
Big Pharma’s infiltration of regulatory and public health agencies goes back more than 100 years to the creation of the Rockefeller Foundation in 1913. Just two years earlier, John Rockefeller’s Standard Oil Company had been ruled an unreasonable monopoly and split into 34 companies, which became Exxon, Mobil, Chevron, Amoco, Marathon and others.
The breakup only served to increase Rockefeller’s wealth, however, and the foundation he created under his named was deemed “a menace to the future political and economic welfare of the nation.”
The Foundation, in partnership with Andrew Carnegie and educator Abraham Flexner, then set out to centralize U.S. medical schooling, orienting it to the “germ theory” of disease, which states that germs are solely responsible for disease and necessitates the use of pharmaceuticals to target said germs.
With that narrative in hand, Rockefeller financed the campaign to consolidate mainstream medicine, adopt the philosophies of the growing pharmaceutical industry and shutter its competition.
Rockefeller’s crusade caused the closure of more than half of U.S. medical schools, fostered public and press scorn for homeopathy, osteopathy, chiropractic, nutritional, holistic, functional, integrative and natural medicines, and led to the incarceration of many practicing physicians.
The full story, including how the Rockefeller Foundation imbued its philosophy, precepts and ideologies into the League of Nations Health Organization, which turned into the World Health Organization, can be found in “The Real Anthony Fauci.”
Chronic Diseases Skyrocket Under Fauci’s Lead
In 1984, when Fauci was appointed director of NIAID, 11.8% of Americans had a chronic disease. Contrast that to today, when 54% are now suffering from chronic illness.4 Fauci doesn’t talk about this public health failure — at least not publicly — but as Kennedy noted, it was Fauci’s job to figure out why autism, allergies and so many other diseases have increased, identify the toxins causing them and eliminate them.
“Fauci could have prevented the whole thing,” Kennedy noted, referring to the epidemic of chronic diseases now plaguing Americans, but instead of running a true public health agency he turned it into an incubator for pharmaceutical products. According to Kennedy, between 2009 and 2016, 240 new drug products were approved by the FDA, and all of them came from Fauci.
“He has a $6.1 billion budget that he distributes to colleges and universities to do drug research for various diseases,” Kennedy said. “He has another $1.7 billion that comes from the military to do bioweapons research, and that is why he had to do the gain of function … He was locked into that; 68% of his personal salary comes from doing military/bioweapons research that used to be called ‘dual use.’”5
Fauci Has Long Promoted Gain-of-Function Research
Dual use research is so named because it involves research on select agents and toxins that could either benefit society or destroy it, depending on whether or not it falls into the wrong hands. Fauci specifically spoke about dual use research of concern (DURC), which involves 15 potentially deadly pathogens like smallpox and Ebola virus, at a hearing before the Committee on Homeland Security and Governmental Affairs at the U.S. Senate, held April 26, 2012.6
DURC involves seven categories of research experiments, according to the CDC, which includes gain of function (GOF) and which may enhance the harmful consequences of the agent or toxin, among others.7 Because GOF and DURC can be used to make pathogens more readily able to infect humans, they pose major biosecurity risks.
After the 2001 anthrax attacks, the CIA began pouring money into bioweapons research. The Pentagon was nervous about conducting such studies because it was prohibited, so cohorts funneled money to Fauci to do it, Kennedy said. Because he called it dual use “vaccine research,” it was allowed to continue.
Another moratorium was placed on U.S.-funded GOF research in October 2014, after a string of concerning events, including publication of controversial GOF studies and high-profile “incidents” at U.S. biocontainment laboratories, led to more than 300 scientists launching a petition calling for an end to GOF research.8
That moratorium was lifted in December 2017,9 but in the meantime Fauci continued his controversial research by funneling money to the Wuhan lab in China, partnering with Chinese military scientists, and teaching them how to take bat coronaviruses and make them transmissible to human beings.
“Fauci was giving them millions and millions of dollars,” Kennedy said, “but the biggest contributor was the CIA, and the Pentagon through DARPA.” The three were all working in tandem, teaching the Chinese how to weaponize bat viruses.
Fauci Experiments Killed at Least 85 Children
Fauci’s sordid past goes back to the AIDS crisis, which is now being used as a template for what’s happening during COVID-19, and the fabrication of past pandemics, including Zika virus, for the purpose of selling pharmaceuticals and advancing totalitarian control.
One of the most atrocious acts, however, included barbaric and illegal experiments that the NIAID conducted on children, testing pharmaceuticals. Fauci “got control of foster homes in seven states and turned pharmaceutical companies loose on these children,” Kennedy said.
“The children were tortured. They did not have legal representation, which is illegal. They did not have guardians. You cannot put a child into a clinical trial in this country without a legal guardian. And he made sure that those kids did not have guardians. They were literally tortured to death … many of the kids did not have HIV, they were just guinea pigs.
The children who refused or were noncompliant were sent to Columbia Hospital and had feeding tubes installed in them so the drug companies could administer the drugs even when the kids fought back. At least 85 of these kids died during the experiments.”10
A graveyard was found in Hawthorne, New York, with a pit covered by an Astroturf carpet that had hundreds of tiny coffins piled up with the bodies of these children inside, Kennedy said. “After New York, he took that roadshow to Africa and ended up killing many pregnant mothers and getting away with it.”
Using Fear to Disable Critical Thinking
Waking up to Fauci’s façade is necessary to understand the orchestrated planned use of pandemics to clamp down totalitarian control. One sign of the ensuing control is the deep involvement of intelligence agencies in the pandemic process, even though they’re not health agencies. Kennedy explains:11
“The intelligence agencies and health agencies have developed these extraordinary techniques for using fear to disable critical thinking. If you look at the whole rationale behind this pandemic, all of these rationales collapse.
Why are we mandating vaccines that don’t prevent transmission? What is the possible reason? That’s just one of many absurdities of what we’re doing today. But people who are subsumed in the orthodoxy, which is the product of orchestrated fear, misinformation and propaganda, need to be woken up.”
He references the now-infamous experiment conducted by Yale University psychologist Stanley Milgram in 1962, during which he tested the limits of human obedience to authority. The Milgram experiment was conducted following the trial of Nazi Adolf Eichmann, who used the Nuremberg defense, or “befehl ist befehl,” which translates to “an order is an order.”
The Milgram experiment clearly showed that people would act against their own judgment and harm another person to extreme lengths simply because they were told to do so.12 What does this mean for the future, if people blindly obey and submit to totalitarian control? Kennedy said:13
“I think this is historical jeopardy to humanity that we’ve never seen before. You know, the black plague and WWII are arguably rivals for it. But I would argue that this is the worst thing that has ever happened to humanity because the essential ambition of the totalitarian state is to control, not just conduct, but self-expression and thought.
And for the first time in history, because of the technological revolution, the capacity for totalitarian forces to literally control every aspect of human expression and even human thought is now unprecedented.”
Waking Up to the Truth
In China, a vast array of facial recognition technology that claims to be able to read guilt on a person from a distance has reportedly already been deployed. “This is precrime,” Kennedy says, like the movie “Minority Report.” In such a technocratic world, however — unlike at any point in history — there’s nowhere to run, and nowhere to hide:14
“In Hitler’s time you could run for the border, and there were ways that a certain number of people were going to escape. They were going to regroup and there was opposition from other countries.
Today, we have this situation where the U.S. military and the CIA are conspiring with the Chinese CDC and military scientists, developing bioweapons together and conspiring to lie to the public … We have U.S. federal officials who are conspiring with Chinese military officials to hide truth from the American public.”
“I would say this is Armageddon,” Kennedy said. “This is the apocalyptical forces of ignorance and greed and totalitarianism. This is the final battle. We need to win this one,” and the first step to doing so is waking up to the truth.
Not one single, healthy, child between the ages of 5 and 18 has died in Germany due to COVID, according to a huge new study.
Even when counting children and adolescents who had preexisting conditions, still, only six in that specific age range died. According to Slate, about 1.5 million German children or adolescents were infected with Sars-Cov-2 between March 2020 and May 2021.
When counting anyone under age 18, just “14 Germans under 18 died of COVID, about one per month. The data “again raises the question of how health authorities can possibly justify encouraging children or teenagers to be vaccinated,” Slate said.
The complete study was published on the preprint site medRxiv.org.
 Skip to the content
Skip to the content